Introduction
Kawasaki disease (KD) is one of the most common vasculitides of childhood [1]. It is typically a self-limited condition, with fever and manifestations of acute inflammation lasting for an average of 12 days without therapy [2]. However, complications such as coronary artery (CA) aneurysms may develop and lead to significant morbidity and mortality [3]. Kawasaki disease is the most prominent cause of acquired coronary artery disease (particularly coronary aneurysms and obstruction) in childhood [2]. Treatment with intravenous immune globulin (IVIG) within the first 10 days of illness reduces the prevalence of CA aneurysms fivefold when compared with children not treated with IVIG [4, 5]. Early diagnosis is critical to achieve the optimal treatment result. However, timely identification is challenging because the diagnosis is based upon nonspecific clinical signs, and there is no definitive diagnostic test [3].
The diagnostics of KD have become more recognised only in recent years, and there are no official data for Latvia about the incidence rate, patient characteristics, or received treatments. In this study, the authors analysed data taken from the database of hospital discharge codes regarding hospitalised children classified with a KD code for a period of 8 years. This data were used to calculate the mean annual incidence of KD and the resistance to treatment among children in Latvia, and to understand the correspondence with European data.
Risk stratification has proven useful in identifying Japanese children treated for KD in Japan, who are at high risk of IVIG resistance [6–8]. Further studies are needed to prospectively validate criteria for identifying high-risk patients in other populations [6], therefore the Kobayashi risk score was calculated for each patient in this study.
Material and methods
In Latvia, the Children’s Clinical University Hospital (CCUH) is the only children’s hospital in the country; therefore, patients with suspected KD from all Latvian regions are transferred to CCUH to receive their initial treatment. The data were collected using the CCUH’s electronic database.
In this study, we identified all children who were discharged from the hospital with an International Classification of diseases (ICD) coding for KD (ICD10 M30.3). Retrospective medical data retrieved over 8 years (January 2012 to December 2019) were collected and reviewed. The patients’ demographic, clinical, laboratory, echocardiographic, and treatment data were recorded. All patients below 18 years of age diagnosed with KD were included in the study. Hospitalisation rates and estimates of annual incidence were expressed per 100,000 children, using national census estimates for the years 2012–2019.
Resistance to the treatment was defined as persistence of fever 36 h after the end of initial IVIG infusion. Criteria that increases the risk for IVIG resistance (Kobayashi risk score) was calculated for each patient [6]:
sodium ≤ 133 mmol/l (2 points),
aspartate aminotransferase (AST) ≥ 100 int. units/l (2 points),
C-reactive protein (CRP) ≥ 10 mg/dl (≥ 100 mg/l) (1 point),
neutrophils ≥ 80% of the white blood cell (WBC) count differential (2 points),
platelet count ≤ 300,000/mm3 (1 point),
early diagnosis, with initial treatment at or before the fourth day of illness (2 points),
age ≤ 12 months (1 point).
(Score ≥ 4 identifies patient with KD at a high risk of being resistant to IVIG).
Statistical analysis
The data were analysed using descriptive statistical methods.
Thirty-six patients were included in the study during the period 2012–2019. P < 0.05 was considered statistically significant. All patient data were anonymised prior to use. The non-parametric Mann-Whitney U test was used to calculate the median treatment initiation day, for 2 independent patient groups with and without CA dilatation.
Ethical approval for this study was obtained from the Research Ethics Committee of Riga Stradins University (RSU).
Results
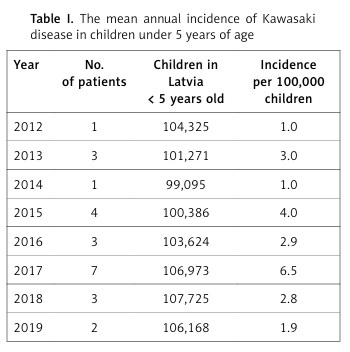
During the study period of 2012–2019 there were 36 patients with KD as the primary diagnosis in Latvia. The median age at admission was 2.8 years (youngest 2 months, oldest 14 years). 67% of cases occurred in patients under 5 years of age, and the male/female ratio was 1.3 : 1. The mean annual incidence rate was 1.3 per 100,000 children 0–18 years old, and 2.9 per 100,000 for children below 5 years old (Table I). Incomplete KD was diagnosed in 33% of cases. The average length of disease until hospitalisation was 6 days (minimum 1 day, maximum 18 days). The mean number of days with disease before diagnosis was 10 (minimum 4, maximum 21 days). The median number of days from fever onset to IVIG administration was 7. The mean length of hospital stay was 14 days, ranging from 6 to 32 days. Coronary dilatation was recorded in 3 (8%) patients, all of whom were male, and 67% of this group under the age of 12 months. The reported mortality rate was 0%, and 14% of patients were hospitalised in the ICU. The epidemiological and clinical features are shown in Table II. The laboratory test results are shown in Table III.
Table I
The mean annual incidence of Kawasaki disease in children under 5 years of age
Table II
Epidemiological and clinical features of patients with Kawasaki disease
Table III
Laboratory markers in children with Kawasaki disease
Coronary artery dilatation was present in 8% (3) of cases: in the first patient the coronary dilatation spontaneously regressed, and no dilatation was observed in the follow-up diagnostic angiography; in the second patient, coronary dilatation persisted with LCA 3 mm, LMCA 4.1-4.4 mm (+2.1z) and RCA 4.9–5.0 mm (+2.7z). The patient is still being regularly observed by cardiologists. In the third patient the coronary dilatation was not present at the time of diagnosis but developed during follow-up. The dilatation currently persists without negative dynamics with LMCA 3.3 mm (+3.82z), RCA 3.5 mm (+4.9z).
All 36 patients received an IVIG infusion. Resistance to treatment was observed in 25% of cases (19% received additional steroid pulse therapy and 6% received a second IVIG infusion).
Of the patients with increased risk for IVIG resistance (19%), 29% received additional steroid pulse therapy. However, for 71% of patients the treatment was successful with 1 infusion of IVIG. There were no statistically significant differences between higher risk and prolonged hospital stay.
In the patient group that received additional steroid therapy treatment (19%), 71% had a low risk score of 1–2, and 29% had a risk score of 4. Those who received the second IVIG infusion had a low risk score of 1–2.
All patients with CA dilatation (8%) received 1 IVIG infusion, had a risk score ≥ 3, and a treatment initiation of ≥ 9 days.
Although the number of patients included is low, there were statistically significant differences between patients with and without CA dilatation, and day of treatment initiation. The treatment in all patients with CA dilatation was delayed, and the median day of treatment initiation was 19. For patients without CA dilatation, the median day of treatment initiation was 7 (p < 0.05).
Discussion
This is the first epidemiologic study of KD in Latvia. This study revealed a mean annual incidence of 2.9 per 100,000 children under 5 years of age, from 2012 to 2019. The mean incidence varied between 1.0 and 6.5 during the 8-year study period. In comparison, the incidence rate in Europe for children under 5 years of age is 5–10 per 100,000 [9], which suggests that the incidence rates in Latvia are lower than those reported for other European countries. This could be due to factors such as unawareness of the disease, the resemblance of KD with other infectious diseases, and the lack of any specific diagnostic test. The incidence rate in recent years has not increased significantly.
Sixty-seven percent of cases occurred in patients under 5 years of age, which corresponds to the northern European results. In comparison, 86.4% of Japanese KD patients were aged < 5 years, compared to only 67.8% in the northern European countries (Finland, Norway, Sweden), which remains unexplained [10].
Fever persisting for 5 or more days was the most frequent clinical manifestation of KD, followed by exanthema, changes of lips, and the least frequent symptom – acute non-purulent lymphadenitis [11].
Other studies describe the incidence of CA dilatation in 25–30% of patients with KD at the time of diagnosis in untreated cases [12–14]. The percentage of CA dilatation in our study was 8%, which corresponds to the fivefold reduction of CA aneurysms in treated cases [4, 5].
The CA dilatation developed in patients with a delayed treatment initiation. This once again proves that timely diagnostics and treatment are crucial in the management of KD.
The percentage of refractory treatment in our study was higher (25%) than in other studies with refractory KD, appearing in about 10–20% of patients who were initially treated with IVIG and aspirin [2, 15]. This could be due to the limited number of patients included in the study.
Additional steroids were given to 19% of children in our study, who had a poor response to the initial dose of IVIG.
Although the number of patients in the study was low, the known risk scores did not accurately reflect the resistance to treatment in this population, which corresponds to the low sensitivity reported in other studies for non-Japanese children [16–18]. It would be beneficial to validate a score for non-Japanese children, which could predict the risk of treatment failure.
However, this study does have some limitations. The number of KD-associated hospitalisations could have been underestimated, due to the inclusion of misdiagnosed KD cases, or lack of inclusion of cases in which patients were not hospitalised. Overall, the number of patients included in the study is low; therefore, it is difficult to draw conclusions. The retrospective character of our study is also a limitation, due to missing data in some parameters, such as clinical characteristics.
As the first Latvian study, this may serve as a useful tool for further clinical and epidemiological studies.