Introduction
Community-acquired pneumonia (CAP) is one of the main causes of childhood mortality in the underdeveloped world, causing over 800 000 deaths annually in children under 5 years of age. In the developed world, CAP is still a common and potentially serious illness associated with significant morbidity [1, 2].
Vaccination with the pneumococcal vaccine reduced the incidence of classical bacterial pneumonia in developed countries. However, Streptococcus pneumoniae remains an important cause of CAP in children [3]. Most children with CAP can be treated as outpatients, and antibiotics are often prescribed, as there are no widely available biomarkers for the differentiation of viral from bacterial causes [4, 5].
The excessive use of broad-spectrum antibiotics promotes the spread of resistance across multiple bacterial species and has a detrimental effect on the host microbiome [6]. Therefore, most guidelines encourage the use of narrow-spectrum and penicillin-based antibiotics in children with (presumed) bacterial CAP [4]. The European Society for Paediatric Infectious Diseases 2012 guidance recommends either penicillin G or aminopenicillins [7] for children with CAP aged 3 months to 5 years. Similarly, clinical practice guidelines from the Pediatric Infectious Disease Society and Infectious Disease Society of America suggest either ampicillin or penicillin G for inpatient treatment of CAP in a fully immunized child when local epidemiologic settings do not document high-level penicillin resistance [8]. However, broad-spectrum antimicrobial agents (including macrolides) are often prescribed in clinical practice in Europe and in the United States [9–11].
In Slovenia, the susceptibility of S. pneumoniae to penicillin is over 90% and is among the highest in the world [12]. Therefore, our national guidelines recommend intravenous penicillin as a first-choice treatment for bacterial CAP in hospitalised children, and the combination of amoxicillin and clavulanic acid is provided as an alternative, as shown in Table I [13]. However, the resistance of pneumococci to penicillin in Slovenia is increasing, and recent data from 2017 showed 0.4% resistance and 14.9% intermediate susceptibility to intravenous penicillin [14].
Table I
Intravenous antibiotic treatment of bacterial CAP in children according to the Slovenian national guidelines [13]
| Age | Antibiotic | Daily dose/kg: n1 |
|---|---|---|
| 4 months to 5 years | Benzylpenicillin G (C) | 150 000–250 000 units: 4 |
| Amoxicillin/clavulanic acid (A) | 100 mg (amoxicillin): 3–4 | |
| 5–18 years | Benzylpenicillin G or Amoxicillin/clavulanic acid | 150 000–250 000 units: 4 maximal daily dose 24 million units 100 mg (amoxicillin): 3–4 maximal daily dose (amoxicillin): 4 g |
| 4 months – 18 years – allergy to penicillin | Cefuroxime | 100 mg: 3 maximal daily dose – 4.5 g |
Several studies compared the effect of broad- and narrow-spectrum antibiotics in children with CAP and have shown comparable efficacy, measured by the length of stay, complication rate, decrease of white blood cells (WBC) count and C-reactive protein (CRP) level as well as by interval to permanent defervescence [15–17]. However, these studies were performed a decade ago and to the best of our knowledge, no such studies have been recently performed in European countries.
The research question of our study was: “Is penicillin G as effective as other β-lactam antibiotics in treating the bacterial CAP in hospitalized children?” We hypothesised that the effectiveness of treatment with penicillin G is comparable to that of broad-spectrum antibiotic treatment. More specifically, the duration of fever, regression of pneumonic consolidations, improvement of laboratory results, length of stay and complication rate in patients treated with penicillin G are comparable to those of treatment with broad-spectrum antibiotics. Therefore, the aim of the present research was to perform a prospective study comparing the effect of intravenous treatment with penicillin G and broad-spectrum β-lactam antibiotics.
Material and methods
Participants
We performed a prospective study and included 136 children with bacterial CAP who were hospitalised in our Department of Pediatrics from October 1, 2014 to August 31, 2019. The age of the patients ranged from 4 months to 16 years. Pneumonia was diagnosed according to the British Thoracic Society (BTS) criteria [18] and confirmed with lung ultrasound (LUS). All the studied children were previously healthy and were not born prematurely. We excluded patients who had already been treated with antibiotics in the last 2 weeks before admission. In addition, we excluded patients who had already been admitted with severe CAP and immediately required management in the paediatric intensive care unit (ICU) or had a large pleural effusion (> 1 cm thick) at admission. Some patients were excluded only after the completion of treatment when alternative diagnoses or aetiologies were established. Bacterial CAP was excluded in all patients in whom we detected atypical bacteria (e.g., Mycoplasma pneumoniae or Chlamydophila pneumoniae) as well as in all patients with normal serum procalcitonin (PCT) level (< 0.25 ng/ml) [19]. When no viruses or atypical bacteria were detected, either leucocytosis (> 15 × 109/l) or alveolar infiltrate on CXR was sufficient for the diagnosis of bacterial CAP [20–22]. Bacterial CAP (co-infection or superinfection) was still considered in patients with leucocytosis and alveolar infiltrate on CXR, even when viruses were detected in the nasopharyngeal swab. When no aetiology could be established, the patient was also excluded from the study. The recruitment of patients for the study is presented in Figure 1. The final diagnosis of bacterial CAP was confirmed at discharge from the hospital by two senior paediatric pulmonologists.
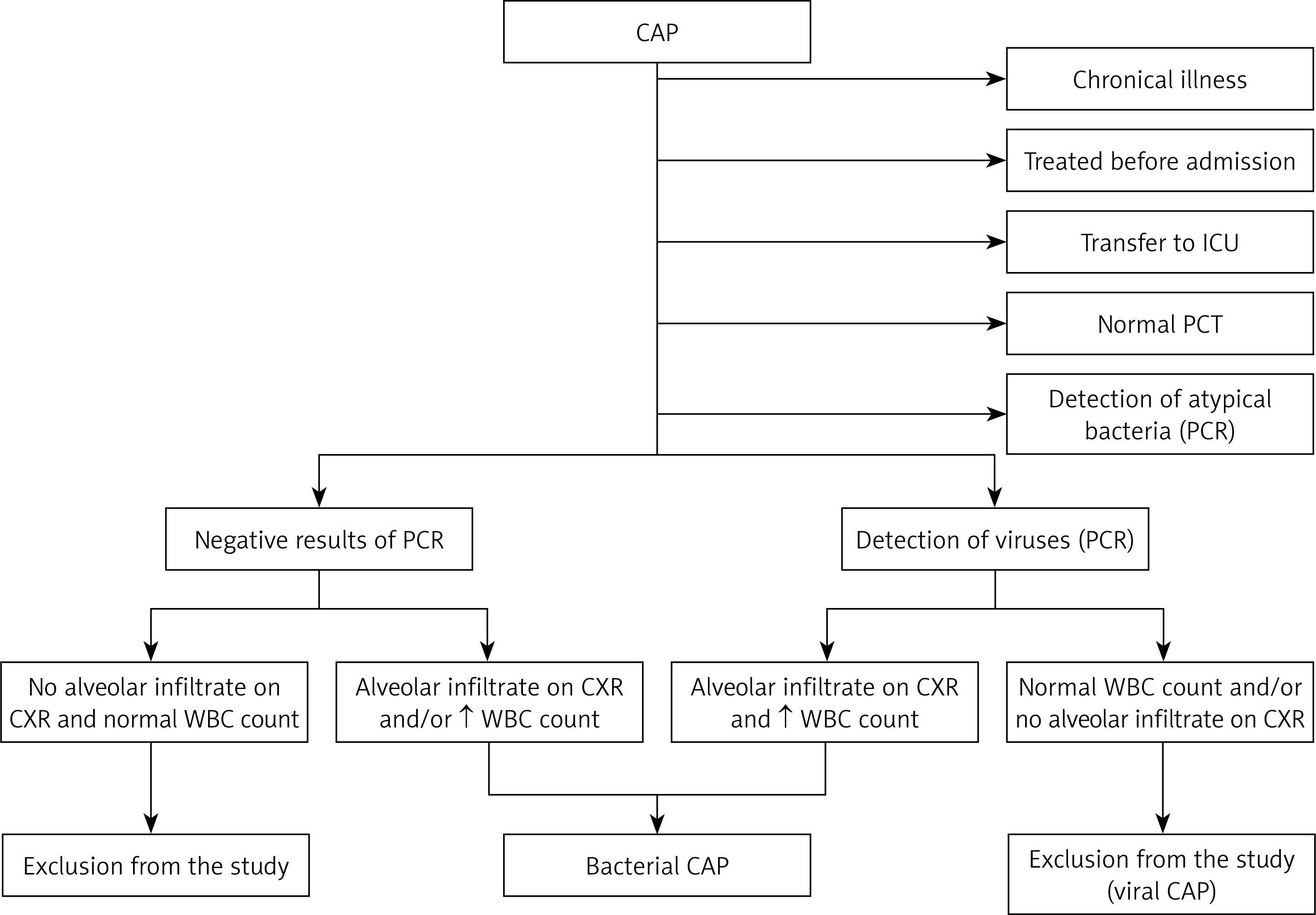
Figure 1
Recruitment of patients with bacterial community-acquired pneumonia. 271 patients with community- acquired pneumonia were enrolled initially. Of those, 5 were treated in the intensive care unit from admission, 37 had chronical illness or have been born premature, 68 had normal procalcitonin level, 27 received antibiotics before the admission, 27 were identified as atypical bacterial pneumonia, 62 as viral pneumonia and in 42 patients no aetiology could be identified. A large proportion of patients were excluded by more than one criterion
CAP – community-acquired pneumonia, PCR – polymerase chain reaction-based assay from nasopharyngeal swabs, normal PCT – serum procalcitonin level < 0.25 ng/ml, ↑ WBC – increased white blood cell count (> 15 × 109/l), CXR – chest X-ray, ICU – intensive care unit.
Clinical characteristics and length of hospital stay were recorded. Body temperature was measured with a tympanic thermometer every hour from admission until permanent normalisation of body temperature (below 37.5°C), and the interval from administration of antibiotics to permanent defervescence was recorded. Complications that emerged during the treatment, such as large pleural effusion (> 1 cm thick – measured with LUS) or empyema, pulmonary abscess, need for transfer to the ICU and need for readmission (in 7 days), were recorded.
Ethical approval and informed consent
The study was approved by the Ethics Committee of University Medical Centre, Maribor, Slovenia. The study was performed according to the World Medical Association Declaration of Helsinki, revised in 2000, Edinburgh, and with the understanding of all participants or their legal guardians (for children younger than 16 years), who signed an informed consent form.
Diagnostic investigations
Venous blood was collected from all participants at admission to obtain complete and differential blood counts, C-reactive protein levels and blood cultures. White blood cell and neutrophil counts were recorded. PCT levels were determined in most patients. Laboratory results of WBC count and CRP tests were repeated 48 h after admission. We collected nasopharyngeal swabs from all patients for the detection of respiratory viruses and atypical bacteria using polymerase chain reaction (PCR)-based assays. All microbiological assays were performed by the National Laboratory of Health, Environment and Food, Maribor, Slovenia.
All patients underwent LUS on the day of admission, followed by CXR in 119 (87.5%) patients. LUS was repeated after 48 h in 64 (47.1%) patients. CXR was performed in all patients with uncertain aetiology (e.g., detected viruses and leucocytosis) and at the discretion of the treating physician. A standard posteroanterior (PA) view was used, and the images were evaluated by a paediatric radiologist.
Lung ultrasound
In the last decade, several studies and meta-analyses have proven lung ultrasound (LUS) to be an excellent alternative to CXR [23, 24]. LUS is especially suitable for follow-up and monitoring of CAP [25, 26]. LUS was performed with a Sonosite (SonoSite, Inc. Bothell, WA, USA) portable ultrasound machine by a paediatric pulmonologist. We used a linear probe (13–6 MHz) in infants and toddlers and a curved probe (8–5 MHz) in older children and adolescents. LUS was performed according to the technique described by Copetti and Cattarossi [27]. Pleural effusion presence was also recorded. However, only the presence of consolidation was considered a diagnostic criterion for pneumonia in our study. Pneumonic consolidation was defined as the presence of hypoechoic or isoechoic (echogenicity similar to that of the liver) areas with dynamic air bronchograms and/or shred signs to distinguish between pneumonic consolidation and lung collapse [28, 29].
The dimensions of each consolidation were measured in the longitudinal, transverse and sagittal axes, and the largest diameter was recorded. At follow-up, the LUS regression/progression of consolidation sizes was evaluated as described above.
Antibiotic treatment
All the patients were treated with antibiotics administered intravenously according to the Slovenian national guidelines [13], as presented in Table I. The choice of antibiotic was at the discretion of the treating physician, and monotherapy was prescribed in all cases.
Statistical analysis
Statistical analysis was performed with IBM SPSS 24.0 software (IBM Inc., Armonk, NY, USA). Initial data were matched between treatment groups using propensity score matching by means of logistic regression (sampling without replacement) and using predictors such as age, presence of respiratory distress, need for additional oxygen, pretreatment CRP level and WBC count and pretreatment size of LUS-detected consolidation. Match tolerance was set to 0.1. The Mann-Whitney U-test was performed to compare the quantitative variables between the different treatment groups after a Kolmogorov-Smirnov test of normality. To avoid the ceiling effect, laboratory results and consolidation sizes at follow-up were normalised to the initial values to obtain post/pre ratios. Ratios between groups were then analysed using the Mann-Whitney U-test. In addition, we analysed the effect of therapy using binomial generalised linear models, adjusting for sex and age. Kaplan-Meier survival analysis was used to compare the effect of both antibiotic treatment regimens regarding the normalisation of body temperature. For comparison of qualitative (clinical or radiographic) characteristics, Fisher’s exact or χ2 test was used. The α level for all tests was set to 0.05, and p-values are presented for two-tailed tests.
Results
Demographic and clinical characteristics
We included 136 children with CAP, 60 (44.1%) of whom were girls. Eighty-seven (64.0%) patients were treated with penicillin G and 49 (36.0%) with broad-spectrum β-lactam antibiotics; of those treated with broad-spectrum β-lactams, 42 (85.7%) were treated with a combination of amoxicillin and clavulanic acid and 7 (14.3%) with a third-generation cephalosporin antibiotic. Epidemiological, clinical, laboratory and LUS characteristics before the treatment are presented in Table II. No cases were excluded after propensity score matching.
Table II
Epidemiological, clinical, laboratory and ultrasound characteristics of children with community-acquired pneumonia before antibiotic treatment according to the treatment regime
| Characteristic | Penicillin treatment (n = 87) | Broad-spectrum antibiotic treatment (n = 49) | P-value |
|---|---|---|---|
| Crackles on auscultation, n (%)1 | 19 (21.8) | 20 (42.6) | 0.03 |
| Upper respiratory tract infection, n (%)1 | 37 (42.5) | 25 (51.0) | 0.37 |
| Wheezes on auscultation, n (%)1 | 5 (5.7) | 6 (12.2) | 0.20 |
| Chest/abdominal pain2, n (%)1 | 42 (52.5) | 19 (45.2) | 0.57 |
| Diminished breath sounds, n (%)1 | 25 (28.1) | 15 (30.6) | 0.85 |
| Respiratory distress, n (%)1 | 7 (8) | 9 (18.4) | 0.10 |
| Bronchial breathing, n (%)1 | 16 (18) | 6 (12.2) | 0.47 |
| Need for additional oxygen, n (%)1 | 4 (4.6) | 2 (4.1) | 1.00 |
| Chest X-ray infiltrate, n (%)1 | 62 (83.8) | 35 (77.8) | 0.47 |
| Pleural effusion, n (%)1 | 5 (1) | 8 (5) | 0.20 |
| Age, median (IQR) [months] | 39.8 (31) | 34.7 (39) | 0.30 |
| WBC count, median (IQR) [× 109/l] | 22.8 (13.6) | 22.4 (13.4) | 0.15 |
| CRP, median (IQR) [mg/dl] | 149 (106) | 142 (146) | 0.59 |
| Neutrophil count, median (IQR) [× 109/l] | 16.7 (12.6) | 16.2 (12) | 0.12 |
| LUS infiltrate size, median (IQR) [mm] | 30 (20) | 30 (23) | 0.39 |
Effect of treatment
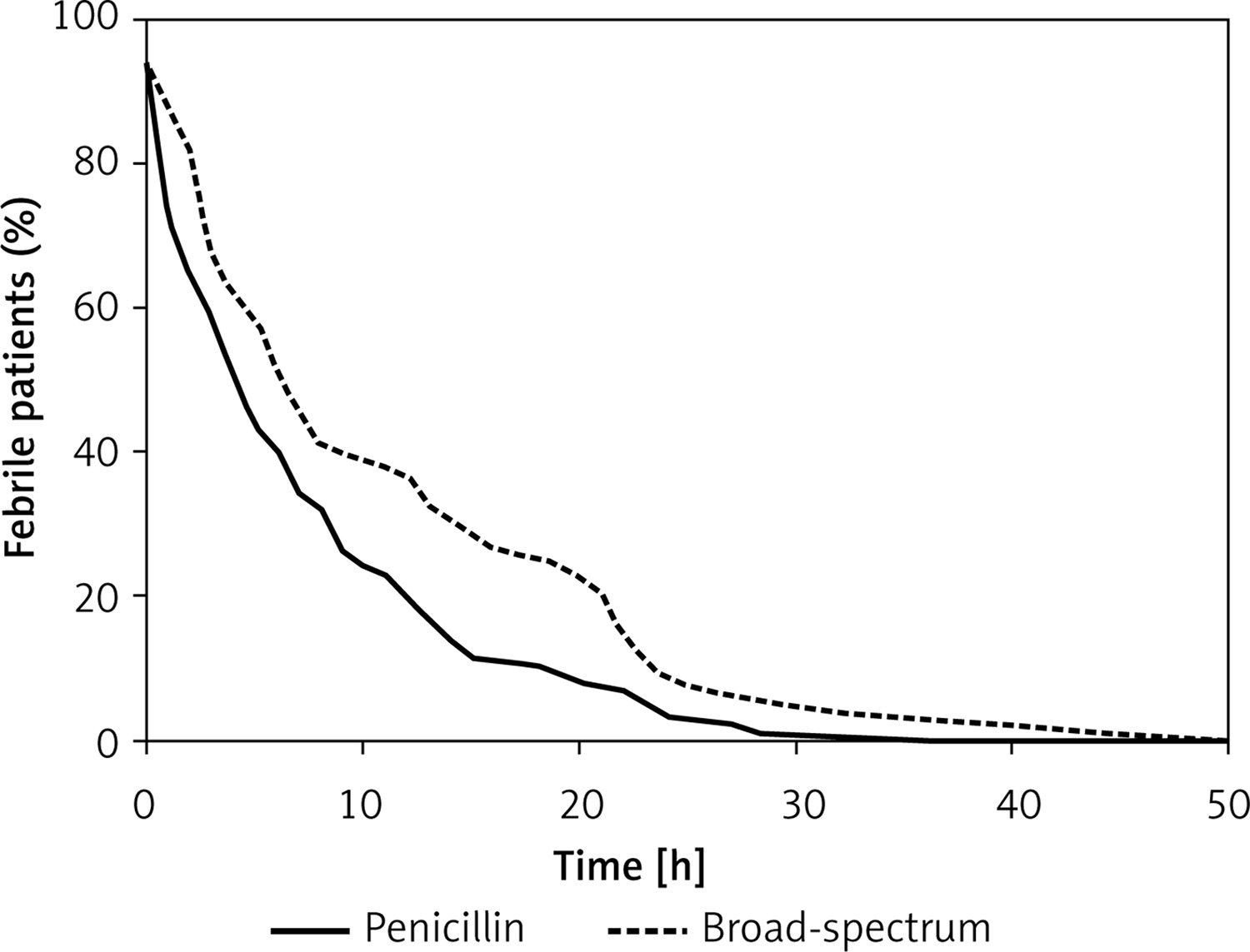
The median time to persistent defervescence was 5 h (IQR = 9) in the penicillin group and 8 h (IQR = 17) in the broad-spectrum group (p = 0.18). The effect of therapy on the normalisation of body temperature is presented with a survival (Kaplan-Meier) graph – Figure 2.
Figure 2
Kaplan-Meier survival curves comparing the effect of penicillin and broad-spectrum β-lactam antibiotic treatment on the normalisation of body temperature in children with community-acquired pneumonia
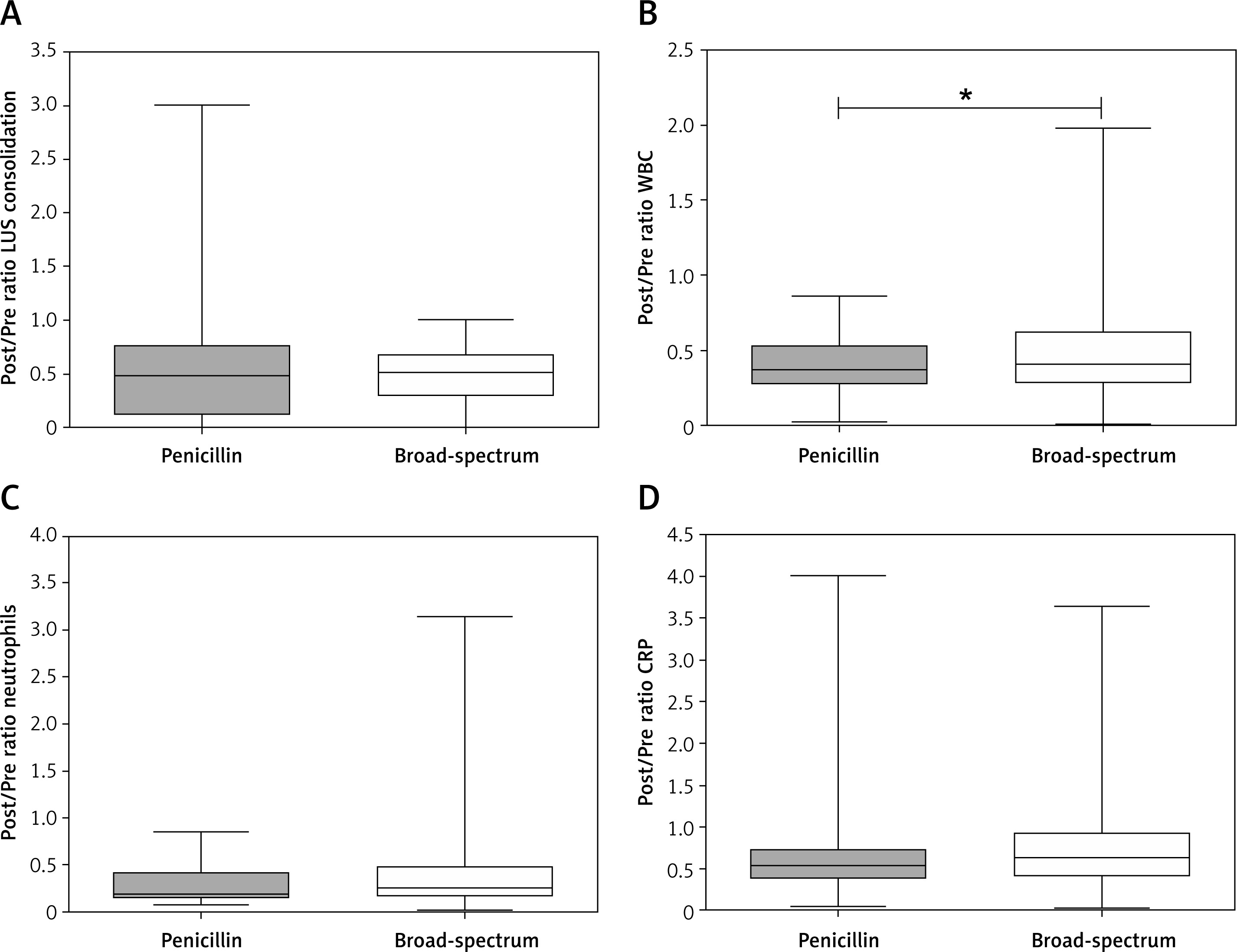
We observed no significant differences between the treatment groups regarding the effect of therapy on the size of the LUS-detected consolidation (p = 0.99), neutrophil count (p = 0.33) or CRP content (p = 0.06) and a marginally better effect of penicillin than broad-spectrum β-lactams on the decrease in WBC count (p = 0.05) (Figure 3).
Figure 3
Comparison of the effect of penicillin and broad-spectrum antibiotic treatment on the consolidation size and laboratory results in children with community-acquired pneumonia
Post/Pre ratio – follow-up value divided by baseline value at admission, CRP – C-reactive protein, WBC – white blood cell count, LUS – lung ultrasound-measured consolidation size, *significant difference.
Regarding the rate of complications, we observed 6 (6.9%) cases of large pleural effusion that emerged during the treatment in the penicillin group and 6 (12.2%) cases in the broad-spectrum group (p = 0.35). Only 4 (4.6%) patients were readmitted in the penicillin group and 2 (4.1%) in the broad-spectrum group (p = 0.86). In the penicillin treatment group, 2 (2.3%) patients needed a transfer to the ICU, compared with 1 (2.0%) patient in the broad-spectrum treatment group (p = 0.92). No other complications were observed. The median length of stay in both treatment groups was 2 days.
In addition, we analysed the effect of therapy, adjusting for sex and age, with a generalised linear model and still found an association of penicillin treatment with greater WBC count decline (p < 0.01) and a marginal association with neutrophil count decline (0.05). There was no association of treatment choice with CRP decline (p = 0.46) or regression of pneumonic consolidation detected with LUS (p = 0.86).
Discussion
In our prospective study, we found that treatment of CAP in children with narrow-spectrum intravenous penicillin is as least as successful as treatment with broad-spectrum β-lactam antibiotics.
We found that the median interval of 5 h from the administration of antibiotic therapy to permanent defervescence in the penicillin G treatment group was comparable to the 8-hour interval in the group of patients treated with broad-spectrum antibiotics. The effects of both treatment regimens on the laboratory results, regression of consolidations (measured with LUS) and the rate of complications were comparable. We observed a marginally significantly greater decrease in WBC count when patients were treated with penicillin. Amarilyo et al. compared the effect of parenteral penicillin G and cefuroxime for the treatment of CAP in Israeli children older than 10 years ago and found that treatment with cefuroxime was not superior. The median time to defervescence in their study was over 24 h, which is much longer than that in our study. The magnitude of the effect of treatment on WBC count and CRP was similar to our results. However, the mean time interval between the initial and follow-up laboratory results was approximately 3 days, which is a day longer than in our study [15]. According to the inclusion criteria and the initial laboratory results at admission, our patients were of similar severity. The better effect of therapy observed in our study can therefore be explained by the very high susceptibility of S. pneumoniae to β-lactam antibiotics in Slovenia [12]. The second explanation for the much shorter duration of fever in our study is the very strict criteria we used for the diagnosis of bacterial CAP, only after performing microbiological investigations to exclude viral and atypical bacterial CAP.
A large retrospective study performed by Williams et al. in the United States compared the effect of treatment of bacterial CAP in children with narrow-spectrum antibiotics (penicillin or ampicillin) and third-generation cephalosporins administered intravenously. They observed no association of treatment choice with hospital length of stay or the rate of complications. The direct comparison of that study with our results is limited, as the main outcomes in our study were different. The other main difference is that the majority (64%) of our patients were treated with narrow-spectrum antibiotics, compared to only 10.3% of patients included by Williams et al. [16].
A study performed by Queen et al. in the United States also compared the effect of CAP treatment in children with broad- and narrow-spectrum antibiotics. However, they considered the combination of amoxicillin and clavulanic acid as well as the combination of macrolide and aminopenicillin as a narrow-spectrum drug regime. Nevertheless, the mean time to defervescence in the study performed by Queen et al. was 6.1 h in the narrow-spectrum group and 9.1 h in the group of patients treated with broad-spectrum antibiotics, which is very similar to our results [17].
In both of the above-mentioned studies performed in the United States [16, 17], the treatment of CAP with narrow-spectrum antibiotics was much less frequently applied than broad-spectrum drug therapy. This situation is in contrast with the 2011 Paediatric Infectious Diseases Society/Infectious Diseases Society of America (PIDS/IDSA) guidelines for the management of children with CAP in which narrow-spectrum antimicrobial therapy is recommended for most hospitalised children [8].
One of the main outcomes of our study was the change in the size of LUS-detected consolidations, which was not used before for the purpose of evaluating treatment effects. Unlike CXR, LUS is an excellent tool for the early follow-up of CAP in children. LUS has already been established as a preferred method for the detection of pleural effusion and a sensitive tool for the detection of CAP in children [23, 28]. Moreover, several studies have shown that LUS findings parallel the clinical course of pneumonia, and the regression of pneumonic consolidations can already be observed after a few days of treatment [25, 26]. Buonsenso et al. have shown the potential usefulness of LUS in monitoring the response to antibiotic therapy in very small sample of children with CAP [30].
Broad-spectrum antibiotics are often prescribed in the emergency department and are then continued in the inpatient setting [3]. Therefore, one of the main reasons that the majority of our patients were treated with narrow-spectrum antibiotics could be the exclusion of all patients treated with antibiotics before admission.
CRP level and WBC count decrease are probably less useful as measures of the antibiotic efficacy in the adult population as pre-treatment values were found much lower (compared to children) with a median CRP level of 68.3 mg/dl and a median WBC count of 11.1 × 109/l in adults with gram-positive bacterial pneumonia [31].
Our study has several limitations. There is no “gold standard” for the diagnosis of bacterial CAP in children. Blood culture is positive in less than 10% of children with uncomplicated bacterial CAP [32]. Sputum is seldom obtained from preschool children, and the results are not specific [33]. Although we used additional criteria for the diagnosis of bacterial CAP (Figure 2) very similar to those recently suggested by Bhuiyan et al. [22], we probably still excluded some children with bacterial CAP in whom we detected respiratory viruses and atypical bacteria. It is well known that the isolation of viruses or atypical bacteria from the upper airways is not direct proof of lower respiratory tract infection because prolonged viral shedding or asymptomatic colonisation is common in children [34]. Although our study was prospective, the patients were not randomly assigned to either treatment group. This potential selection bias stems from the clinical settings of the study and the preference of physicians (who were on duty at admittance) for narrow- or broad-spectrum antibiotics. However, using the propensity score, we found that both groups were matched before the treatment, and no patients needed to be excluded from the study.
In conclusion, we have shown that the treatment of CAP in children with penicillin G is at least as successful as treatment with broad-spectrum β-lactam antibiotics. Such results are even more important in the present era of the increasing resistance of bacteria to antibiotics. The translation of microbiological results into clinical practice is not always straightforward. However, the results of our study should encourage us to adhere to the guidelines that promote the use of narrow-spectrum antibiotics. Such clinical practice minimises the impact of antibiotic use on the emerging problem of bacterial resistance and the collateral damage effect on the microbiota [14].