Introduction
Pediatric acute lymphoblastic leukemia is the most common type of malignant tumor in children, accounting for more than 90% of all malignant tumors in children [1, 2]. Children may show a variety of clinical manifestations such as paleness, dizziness, fatigue, fever, bleeding, and superficial lymphadenopathy [3]. Whether children with acute lymphoblastic leukemia can be cured requires specific analysis of the specific condition. Clinically, childhood acute lymphoblastic leukemia is divided into a low-risk group, a middle-risk group and a high-risk group. For children in the low-risk group and medium-risk group, if they receive regular treatment, the therapeutic effect is very good, most children can be cured, and the cure rate exceeds 90%. However, for the children in the high-risk group, due to the high degree of malignancy, it is often difficult to achieve the clinical effect of general chemotherapy [4, 5]. Therefore, focusing on a new treatment method that stops the progression of leukemia is crucial [6].
Vindesine, which is an alkaloid extracted from Catharanthus roseus [7], is important in the treatment of several types of malignant tumors [8]. It has mild experimental neurotoxicity and the capacity to inhibit tubulin polymerization [9]. Studies have revealed the effectiveness of vindesine in treating pediatric acute lymphoblastic leukemia, chronic myelocytic leukemia, esophageal cancer, and non-Hodgkin’s lymphoma [10]. In contrast, leurocristine is clinically administered to treat acute leukemia and other malignant tumors [11] and is a potential serious neurotoxin [12]. Its mechanism of action has been well elucidated, and its anti-cancer activity and the possibility of its combination with other drugs have been well studied [13, 14]. According to a study, leurocristine may be administered to patients with leukopenia and thrombocytopenia [15–17].
Chemotherapy is the standard treatment for pediatric acute lymphoblastic leukemia, and a rational treatment plan can effectively improve the survival rate in children. In the present study, we used vindesine and leurocristine for chemotherapy and compared their clinical efficacy and their effects on serum interlekin 6 (IL-6) and tumour necrosis factor-α (TNF-α) expression levels and quality of life to provide references for the treatment of pediatric acute lymphoblastic leukemia.
Material and methods
General characteristics
A total of 94 patients with pediatric acute lymphoblastic leukemia were admitted to our hospital for treatment and were categorized into group A (treatment with vindesine, n = 48) and group B (treatment with leurocristine, n = 46). Group A comprised 25 males and 23 females aged 2–12 years (mean age, 5.3 ± 2.9 years). In group A, 23 patients were engaged in house decoration and 25 were not, 24 were exposed to radiation and 24 were not, and 16 lived near chemical factories and 32 did not. In group B, there were 27 males and 19 females aged 3–13 years (mean age, 6.4 ± 3.2 years), including 15, 19, and 11 patients with and 31, 27, and 35 without house decoration, exposure to radiation, and living near chemical factories, respectively. This study was approved by the ethics committee of Yinzhou People’s Hospital, and the guardians of the patients provided completed informed consent forms.
Inclusion and exclusion criteria
Patients who met the diagnostic criteria of pediatric acute lymphoblastic leukemia established by the World Health Organization [18], never received chemotherapy but could provide complete medical records, agreed to receive subsequent treatment at our hospital, and cooperated with the investigation and arrangement performed by our medical staff were included. Patients who had other concurrent tumors; cardiovascular, cerebral, vascular, and blood diseases; immune functional diseases, acute diseases, liver or kidney insufficiency, organ failure, and drug allergy were excluded.
Treatment methods
Both groups were treated in accordance with the Children’s Cancer and Leukaemia Group chemotherapy plan [19] and were administered different drugs during the inductive delay period and delay reinforcement period. Group A was treated with vindesine (Chengdu Shuxi Pharmaceutical Co., Ltd., product No. H20057028) intravenously at a dose of 3 mg/m2 once per week, and group B was treated with leurocristine (Shenzhen Wanle Pharmaceutical Co., Ltd., product No.: H44021772) intravenously at a dose of 1.5 mg/m2 once per week.
Observation indexes
The two groups were observed, and the medical expenses and length of hospital stay were recorded.
For determination of serum IL-6 and TNF-α concentrations, 5 ml of blood was drawn 1 day before and 24 h after administration in a fasting condition, centrifuged for 10 min at 1500 r/min, and placed in a refrigerator at –70°C until use. Serum concentrations were measured by ELISA following the manufacturer’s instructions for IL-6 (Wuhan Elabscience Biotechnology Co., Ltd., product No.: E-EL-H0102c) and TNF-α (Wuhan Elabscience Biotechnology Co., Ltd., product No.: E-EL-H0109c). Standard, sample, and blank control wells (without sample and ELISA reagent) were set up. Approximately 50 µl of standard product was added to the standard wells and 40 µl of sample diluent into the sample wells, followed by 10 µl of sample (finally diluted five times). The wells were sealed and incubated at 37°C for 30 min; the liquid in each well was discarded, and the wells were dried by patting and were repeatedly rinsed five times. Next, 50 µl of ELISA reagent was added to all wells except the blank wells, and the wells were sealed and incubated at 37°C for 30 min, and then 50 µl of developer A and 50 µl of developer B were added to each well, mixed, and reacted at 37°C for 10 min. Finally, 50 µl of stop buffer was added to each well to stop the reaction. To calculate the IL-6 and TNF-α concentrations, the optical density of each well was measured at 450 nm using a BioTek automated ELISA instrument (Beijing Anmaige Trading Co., Ltd., China).
Clinical efficacy: Disappearance of all clinical symptoms and recovery of vital signs to the normal levels indicated complete remission; in complete remission, no leukemia cells were found in the peripheral blood and the patients managed to live a normal life. No improvement in the clinical symptoms and vital signs indicated partial remission. Improvement in the clinical symptoms and vital signs indicated that the patient was stable. No significant changes in the clinical symptoms and vital signs indicated progression.
Adverse reactions (thrombocytopenia, anemia, peripheral neurotoxic reaction, infection, nausea, and vomiting) after treatment were observed and recorded.
Patients’ quality of life before and after treatment was observed and scored according to the KPS scoring criteria, which defined the independent grade as a score of > 80, at which patients can eat and dress themselves independently; the semi-dependent grade as a score of 50–70, at which patients require assistance for daily activities such as eating and dressing; and the dependent grade as a score of < 50, at which patients always require assistance from others in daily life. A higher score indicates better physical conditions.
Follow-up
The 94 patients were followed up by calls or visits once every 3 months for 5 years. The overall survival (OS) is the period from the first postoperative day until the last follow-up or up to the patients’ death.
Statistical analysis
Statistical analysis was performed using SPSS version 22.0 (IBM Corp., USA). In the case of nominal data expressed as [n (%)], comparison studies were conducted using the χ2 test for intergroup comparisons. In the case of numerical data expressed as
Results
General characteristics
No significant difference was observed between the two groups in gender, age, abnormal child-bearing history, gestational age, delivery mode, child-bearing ages of the mother and father, engagement in house decoration, exposure to radiation, living near chemical factories, frequent infection, use of antifebriles, and family history of tumors (p > 0.05, Table I).
Table I
Comparison of general clinical materials between the two groups [n (%)], (x ± SD)
Comparison of basic conditions after treatment between the groups
Patients in group A reported lower medical expenses and shorter length of hospital stay than those in group B (p < 0.05, Table II).
Comparison of inflammatory factor levels before and after treatment between the groups
There was no significant difference in IL-6 and TNF-α expression before treatment (p > 0.05), and both groups experienced a considerable decrease after treatment (p < 0.05), with group A demonstrating much lower results than group B (p < 0.05, Table III).
Table III
Comparison of levels of inflammatory factors before and after treatment between the two groups (x ± SD)
Comparison of clinical efficacy after treatment between the groups
After treatment, group A had 35 complete remission cases (72.92%), 10 partial remission cases (20.83%), 1 stable case (2.08%), and 2 progress cases (4.17%), with a total effective rate of 93.75%. Group B had 25 complete remission cases (54.35%), 15 partial remission cases (32.61%), 3 stable cases (6.52%), and 3 progression cases (6.52%), with a total effective rate of 86.96% (p > 0.05, Table IV).
Table IV
Comparison of total effective rate after treatment between the two groups [n (%)]
Comparison of adverse reactions after treatment between the groups
Group A had a total incidence of adverse reactions of 8.33% based on one thrombocytopenia case (2.08%), one anemia case (2.08%), one peripheral neurotoxic reaction case (2.08%), no infection case (0%), and one nausea and vomiting case (2.08%); in group B, there were two thrombocytopenia cases (4.35%), two anemia cases (4.35%), three peripheral neurotoxic reaction cases (6.52%), two infection cases (4.35%), and three nausea and vomiting cases (6.52%), resulting in a total incidence of adverse reactions of 26.09% (p < 0.05, Table V).
Table V
Comparison of adverse reactions after treatment between the two groups [n (%)]
Comparison of Karnofsky Performance Scale scores before and after treatment between the groups
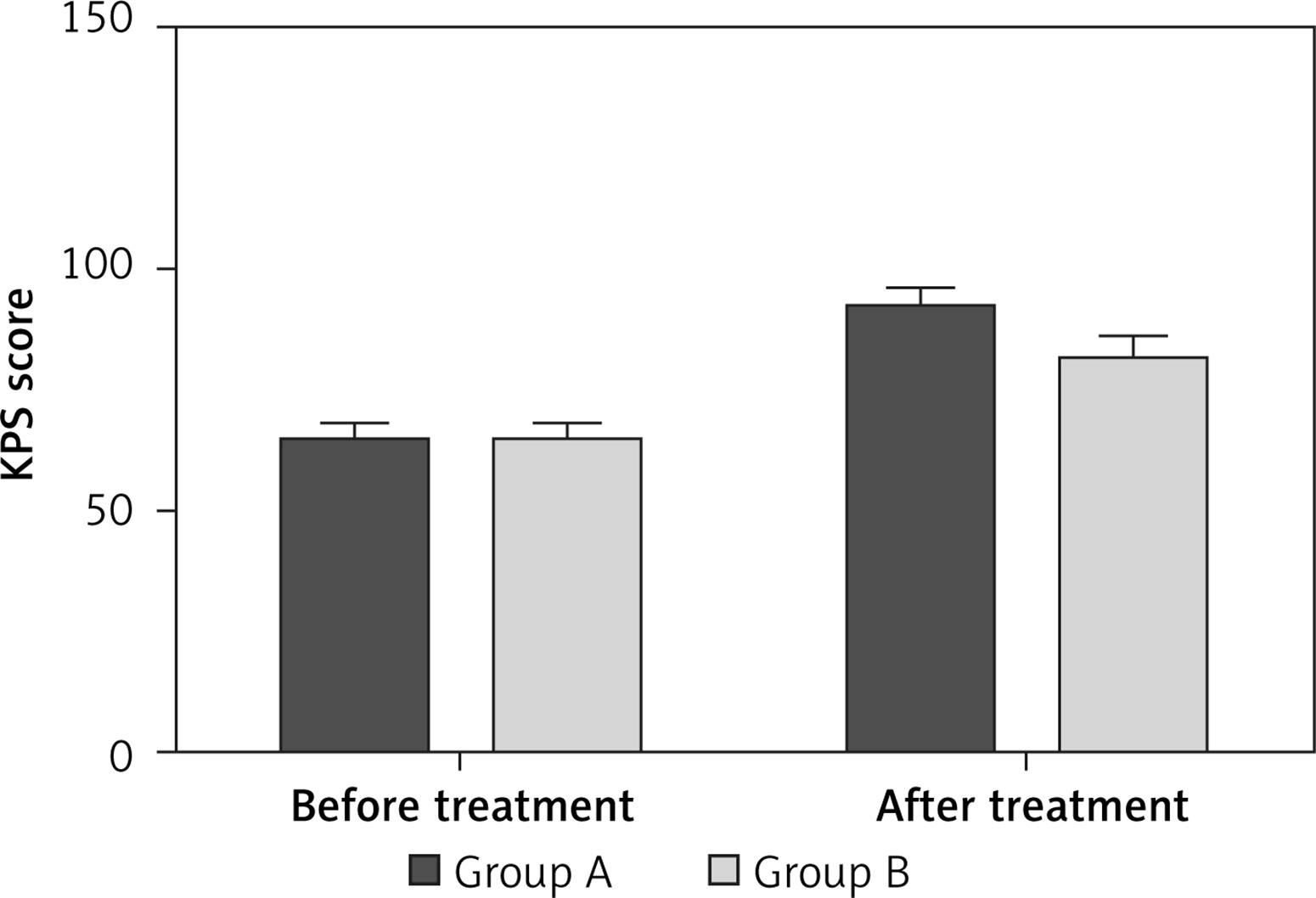
There was no significant difference in the quality of life before treatment (p > 0.05), and both groups showed improvements with treatment (p < 0.05), with group A having higher KPS scores than group B (p < 0.05, Figure 1).
Figure 1
Comparison of Karnofsky Performance Scale (KPS) scores before and after treatment between the two groups. There was no significant difference in quality of life before treatment (p > 0.05), and both groups showed improvements with treatment (p < 0.05), with group A having higher KPS scores than group B (p < 0.05)
* < 0.05 as compared with group B after treatment.
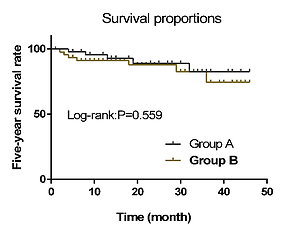
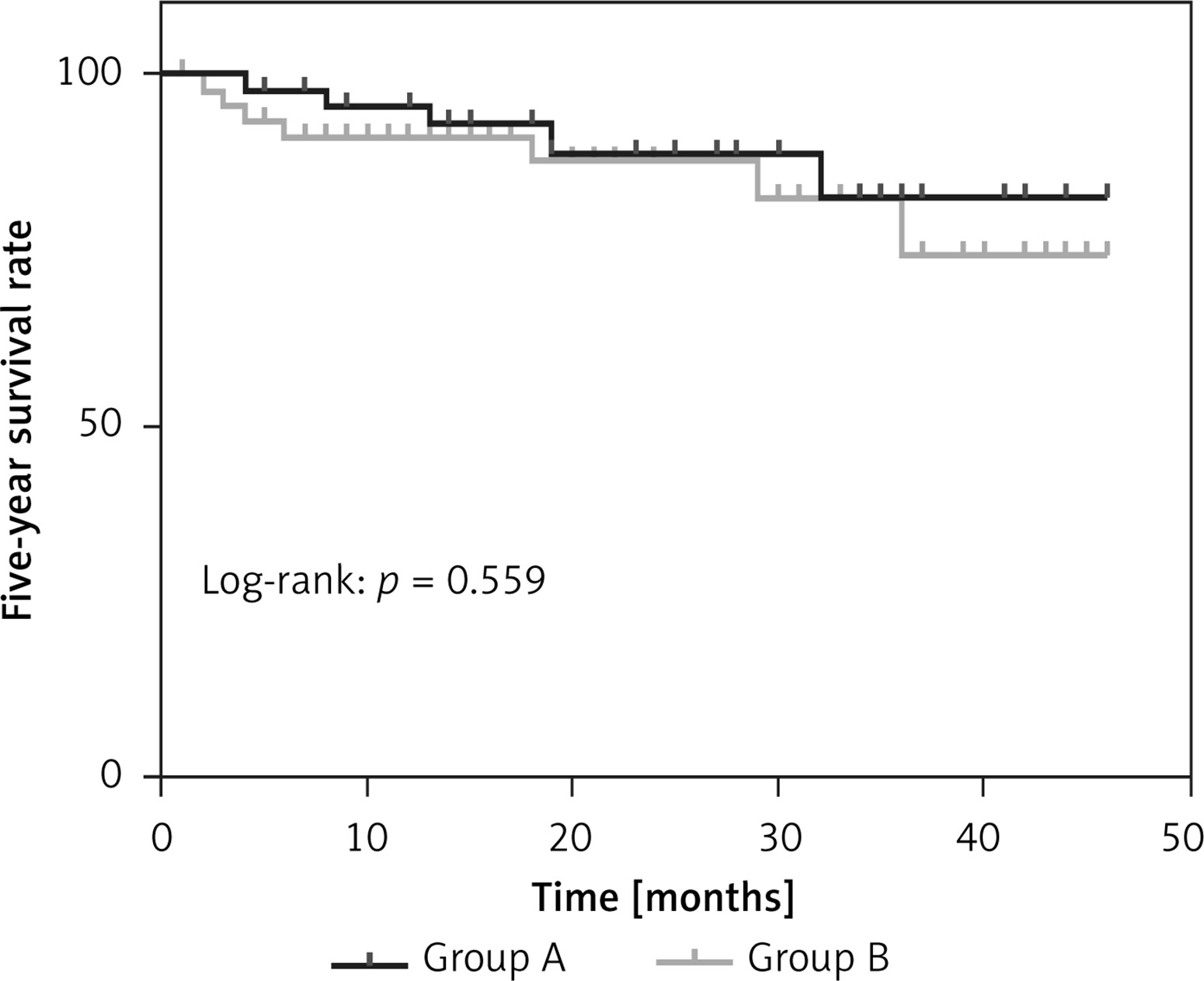
Five-year overall survival
According to follow-up results, the 5-year OS was 89.58% (5/43) in group A and 82.61% (8/38) in group B (p > 0.05, Figure 2).
Discussion
As a frequently occurring pediatric cancer [20–23], acute lymphoblastic leukemia may be caused by genetic factors, virus infection, and immunologic deficiency [24, 25]. In most cases, combined chemotherapy is provided to destroy the leukemia cells in the patients [26] to achieve a higher 5-year event-free survival (EFS) [27]. However, the treatment also leads to increased toxic effects. Thus, to further eliminate the adverse effects in children, innovative methods are required [28].
In the present study, vindesine and leurocristine, both general drugs used in acute leukemia treatment, were used to treat patients with pediatric acute lymphoblastic leukemia, and significant improvements in their conditions were observed. Vindesine showed a higher vitality in the malignant tumors in the blood system and played an important role in the treatment of acute lymphoblastic leukemia, particularly in children [29, 30]. Leurocristine is a cytotoxic alkaloid with extensive anti-tumor activity, and its efficacy depends on its concentration and continuous exposure [31]. Our results revealed no significant difference between the two groups in terms of treatment efficacy and 5-year OS, but group A had lower medical expenses and a shorter length of hospital stay than group B, indicating that vindesine has advantages in terms of medical expenses, length of hospital stay, and safety. Previous studies have indicated that the quality of life can be used as a major marker for the clinical treatment of acute lymphoblastic leukemia [32]. In this study, group A had a better quality of life than group B, proving vindesine’s contribution to an improved quality of life after treatment compared with leurocristine.
Interleukin 6 has demonstrated extensive bioactivity in immunomodulation, tumorigenesis, hematopoiesis, and inflammation [33–35], while TNF-α plays a possible role in B cell chronic lymphocytic leukemia [36–38]. The diagnostic value of these proinflammatory factors [39] in pediatric acute lymphoblastic leukemia has been proven in previous studies [40], and their expression in the serum of patients with leukemia often increases abnormally. The serum IL-6 and TNF-α expression in the two groups showed a sharp reduction after treatment, which was more significant in group A than in group B. Although this study has demonstrated the superior performance of vindesine in reducing the incidence of adverse reactions, length of hospital stay, medical expenses, and serum IL-6 and TNF-α expression and improving the quality of life after treatment, it has limitations and fails to present the specific mechanisms of vindesine and leurocristine that affect the serum IL-6 and TNF-α expression levels. Thus, further studies are required to verify the mechanisms of IL-6 and TNF-α in pediatric acute lymphoblastic leukemia, and basic experiments with larger sample sizes should be conducted to validate our results.
In conclusion, although vindesine and leurocristine showed no significant difference in terms of efficacy and 5-year OS, the vindesine group (group A) demonstrated fewer adverse reactions, shorter length of hospital stay, lower medical expenses, and better quality of life than the leurocristine group (group B), which is possibly related to the reduced serum IL-6 and TNF-α expression.