
Although laryngeal zoster-related cough syncope is rare, it should also be considered in the differential diagnosis in working up a syncopal episode. Pregabalin is an analogue of the neurotransmitter γ-aminobutyric acid (GABA). It can reduce the depolarization and calcium influx of nerve terminals by binding and inhibiting the α2-σ subunit protein of voltage-dependent calcium channels, thereby inhibiting the release of excitatory neurotransmitters such as L-glutamate. The release of these excitatory neurotransmitters is associated with convulsions, pain, and anxiety. We found that pregabalin might be suggested as part of the treatment for its good tolerance, pharmacokinetics, and safety. This paper presents a rare case of a 51-year-old male who presented with cough syncope secondary to laryngeal herpes zoster. Short-term inhaled budesonide suspension stopped the syncope but not the coughs; however, the disturbing post-herpetic cough remained. Although many antitussives had been tried, the therapeutic effect was limited. Pregabalin was finally administered, with highly satisfactory results for cough relief without adverse effects. It provided new evidence that pregabalin use might be justified for the treatment of post-herpetic neurogenic cough.
A 51-year-old male was referred to our pulmonology department with non-productive cough for 14 days. During this time he had experienced 3 episodic losses of consciousness following bouts of cough, leading to emergency hospital visits. These events had precipitated his referral to our specialist cough clinic. His visual analogue scale (VAS) score was 9/10, where 0 is no cough and 10 is the worst possible cough. He had no concomitant symptoms of breathless, haemoptysis, wheeze, or fever. He also complained of hoarseness and progressive throat pain. He had never smoked. Medical review also noted no symptoms of dyspepsia or postnasal drip, and he had neither significant past medical history nor occupational exposure to chemical irritants.
His pulmonary investigations including chest computed tomography (CT) scan, pulmonary function tests, and endoscopic bronchoscopy showed no relevant changes. Overnight oximetry did not suggest obstructive sleep apnoea.
A detailed ear, nose, and throat examination with flexible trans-nasal laryngoscopy was done, which revealed numerous ulcers with purulent exudate on the left half of his supraglottic area, and the left lateral and posterior pharyngeal wall (Figure 1). The vocal fold was markedly oedematous, but vocal fold mobility was intact bilaterally. An empirical diagnosis of laryngeal zoster was made based on these examination findings.

However, laryngeal herpes zoster-related cough syncope is rare, so the patient was admitted for further syncopal (diagnostic) workup to exclude other underlying aetiologies for cough syncope.
The patient underwent an extensive cardiological investigation, including an ECG (electrocardiogram), ECHO (echocardiogram), 24-h Holter monitoring, and carotid artery ultrasound, which were all within normal limits. Further neurological investigations were undertaken with magnetic resonance imaging (MRI) of the brain and electroencephalogram (EEG), which were also unremarkable. Accordingly, all these investigations excluded cardiac and neurological causes. The most likely cause of cough syncope was laryngeal herpes zoster. Daily inhale budesonide suspension 8 mg twice was prescribed by the ear, nose, and throat team. Adjunctive high-dose administration of steroids remains controversial, but it decreases the risk of post-herpetic neuralgia, so the potential benefit should be weighed against their known deleterious effects, particularly in patients with diabetic or psychiatric comorbidities.
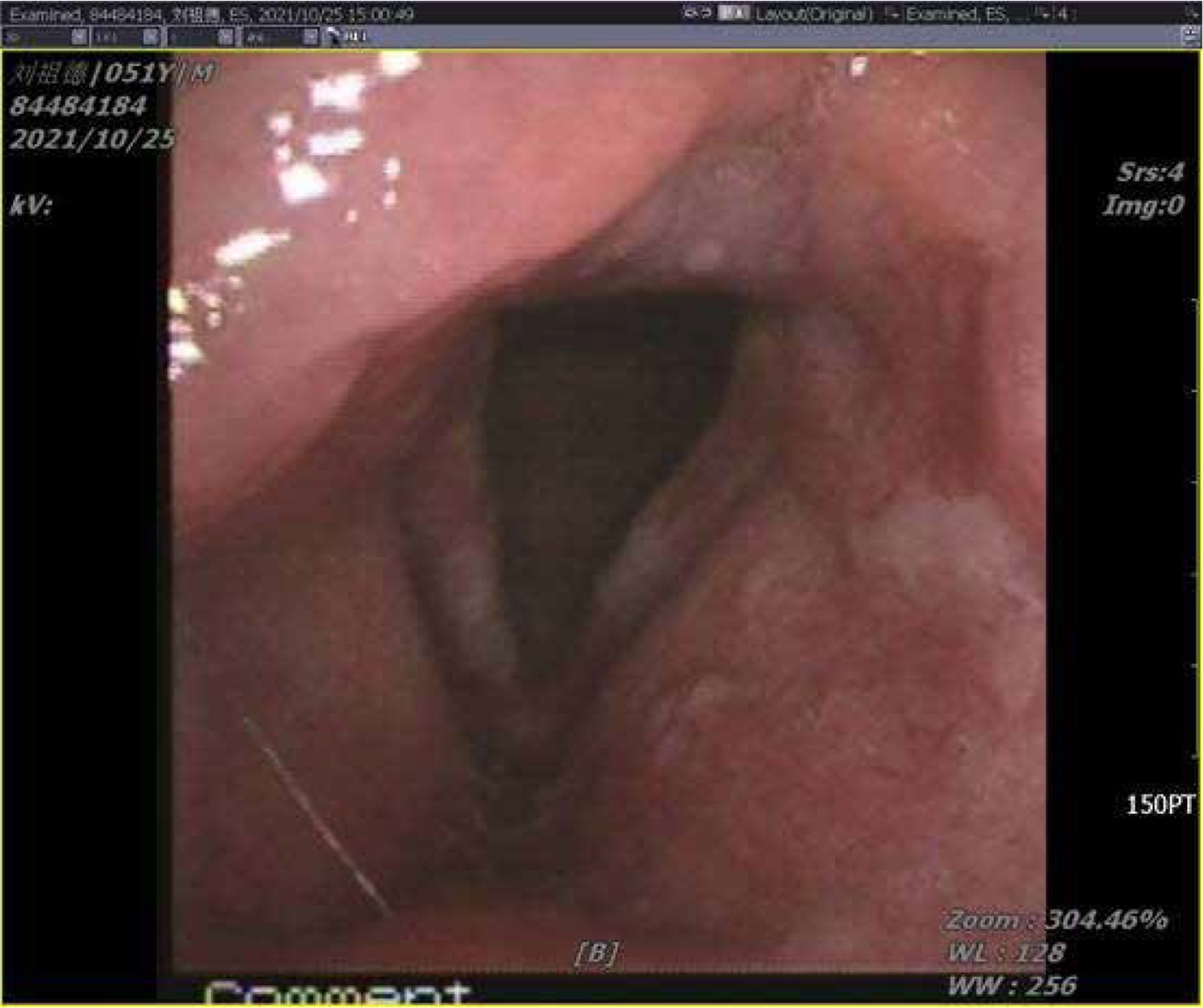
However, antivirals were not suggested because they were not funded for the treatment of herpes zoster beyond 72 h of symptom onset. A week later, his hoarseness and left-sided throat pain had largely resolved. Flexible laryngoscopy showed complete resolution of the ulcers, with some areas of patchy erythema but complete re-mucolisation. Vocal fold oedema was also greatly reduced. He had no recurrence of cough-related syncopal episodes. Unfortunately, it only showed only slight reduction in the severity and frequency of cough, with his VAS score decreasing from 9/10 to 5/10, i.e. he was still experiencing chronic cough (Figure 2).
Figure 2
One week after laryngeal herpes zoster treatment, review the laryngoscopy pictures (2021-10-25)
Subsequently, our patient was given several trials of anticough medications including codeine, dextromethorphan, montelukast, and oral antihistamines (chlorpheniramine), but the effects of these therapies were rather disappointing in alleviating his cough. Finally, the patient was treated with pregabalin at 75 mg twice per day. Surprisingly, after starting it, he reported that the cough was cured. After discharge, the perfect effect was still obtained during drug reduction for one month. Even after drug withdrawal, the patient did not feel cough after 1-year follow-up. It is worth mentioning that he experienced no adverse effects throughout the whole treatment period (Figure 3).

We present a rare case of a 51-year-old male who presented with cough syncope secondary to laryngeal herpes zoster. Short-term inhaled budesonide suspension stopped the syncopal episodes entirely, but the disturbing post-herpetic cough remained. Although many other antitussive drugs had been given, their therapeutic effect was limited. Pregabalin was finally administered, which gave highly satisfactory results for cough relief without adverse effects.
In Herpes zoster, the most typical clinical presentation is vesicular eruption in the skin of the affected dermatome. Neurogenic sequelae, particularly pain, is another frequent clinical presentation [1]. However, as a special kind of herps zoster, laryngeal zosters are characterized by special mucosal manifestations, suggesting a vagal origin of the eruption. Hoarseness, odynophagia, and dysphagia were the predominant clinical symptoms in laryngeal zoster [2, 3]. Respiratory complaints are rarely reported in laryngeal zoster, and cough syncope is even rarer [4].
This study was approved by the Ethics Committee of the 900th Hospital of Joint Logistics Support Forth.
We describe a case of laryngeal zoster with characteristic presentation, which developed a cough, and cough-related syncope, as a post-herpetic sequela. To our knowledge, our report is the first to record laryngeal zoster presenting with symptoms of cough syncope.
Cough-associated syncope may constitute a clinical challenge given the multitude of potential pathophysiological mechanisms and different aetiologies [5]. Now that it is relatively uncommon for patients with laryngeal zoster to present with respiratory complaints, especially cough syncope, it is essential to further screen for many potential aetiologies underlying cough and cough syncope. Hence, in this case, a careful history and systematic evaluation were proposed. Since other differential pathologies and possible provoking factors had been eliminated in the central nervous system, respiratory or cardiovascular systems, cough, and cough syncope were attributed to laryngeal zoster, i.e. they were both regarded as sequelae of laryngeal zoster.
The exact cough-related cough syncope pathophysiology remains uncertain and debated. Various pathophysiological mechanisms have been proposed, such as compression of the midbrain ascending reticular system or vascular complication [6]. Among them, the haemodynamic mechanism seems to be the most convincing [7].
As for post-herpetic cough, there are several proposed pathophysiology mechanisms to explain this phenomenon. In this case, the special distribution of the mucocutaneous lesions from the supraglottic area to the level of the vocal folds conformed to the anatomical distribution of the internal branch of the superior laryngeal nerve (SLN) [8, 9]. It represented the reactivation of varicella zoster virus (VZV) dormant in this area innervated by the vagus nerve, which could result in damage and/or inflammation along the SLN [10].
As we know, the internal branch of the SLN is not only the sensory innervation of the larynx, but also the main primary afferent of the cough reflex. Therefore, the herpetic injury to the SLN could directly give rise to peripheral cough reflex hypersensitivity. Furthermore, some mediators, such as bradykinin, released from the local inflammation of SLN, could stimulate unmyelinated C-fibres, known as a type of peripheral cough receptor and part of the afferent arc of the cough reflex. In other words, these irritants can further enhance the cough excitability.
Another proposed mechanism is related to inappropriate re-synapsing. VZV SLN infection of the internal branch may induce laryngeal hypersensitivity. Meanwhile, its second-order neuron could be rewired in the cough reflex arc to accommodate the axon of an inappropriate primary afferent as a result of deprivation of its original primary afferent due to the damage to the SLN. Accordingly, activities that involve laryngeal function such as talking, laughing, and positional changes could become new inappropriate primary afferents and form a connection with the cough reflex, causing the cough to be evoked erroneously [11].
To sum up, in laryngeal zoster, herpetic infection may damage the vagus nerve, cause hypersensitivity and/or inappropriate re-synapsing of the peripheral cough reflex, and lead to neurogenic cough, and even cough-related syncope.
Similarly to Ling et al. [4], we suggest that the post-herpetic neurogenic cough is a neuropathic disorder, analogous to the post-herpetic neuralgia (PHN) of dermatomal shingles.
In terms of treatment management of cough, syncope should be tailored to individual provoking factors and then to treating the cough [12]. As far as this case is concerned, laryngeal zoster-related cough syncope was the main clinical diagnosis of exclusion when complete workup for other causes of syncope was negative. Short-term inhaled budesonide suspension, as an aetiological treatment, effectively relieved symptoms in the larynx and stopped syncopal episodes entirely, but the coughing persisted, disturbing chronic cough. Although many antitussives had been tried, the therapeutic effect was limited.
Based on this mechanism, as mentioned above, neurogenic medication for postherpetic neuralgia (PHN) could be a new treatment option [13–15]. Some previous studies have shown that gabapentin is effective as a neuromodulator for chronic cough [16–18]. However, due to drug tolerance and serious side effects, its administration was restricted [19]. As part of the new generation of anti-neuropathic pain drugs, pregabalin is regarded as a substitute for gabapentin given its lower dose, better tolerance, and fewer side effects [19, 20].
However, there is no evidence to support the use of pregabalin in acute neuropathic pain scenarios. In the management of chronic neuropathic pain conditions, pregabalin was effective at high doses of 300 mg, 450 mg, and 600 mg daily. In chronic refractory cough, Pregabalin at 150 mg daily could lead to beneficial effects for cough relief. It provided new evidence that pregabalin had a good clinical application in the treatment of chronic cough.
However, given the limited number of clinical studies and fewer data, the optimal dose, the duration of treatment, and the safety of long-term use are still not well understood. Also, whether its administration affects varicella healing on the long with eventual hastened reinfection rate is still unknown. Its therapeutic potential is worthy of in-depth investigation.
In conclusion, this report provided a rare case of laryngeal zoster with characteristic mucosal signs, which developed cough, and even cough-related syncope, as a post-herpetic sequela. Although laryngeal zoster-related cough syncope is rare, it should also be considered in the differential diagnosis in working up a syncopal episode. Given the above proposed mechanisms, there are some similar neuronal pathways in PHN and laryngeal zoster-related cough.