Psoriasis is a common chronic inflammatory skin disease affecting individuals of all ages. Approximately 0.09–11.43% of the global population has psoriasis [1] and nearly one-third of psoriasis cases occur in children [2]. Recent research has focused on the epidemiology of psoriasis, particularly for management and treatment, yet studies specifically targeting children and adolescents remain scarce. To further investigate the burden of children and adolescent psoriasis and furnish a reference for enhancing pertinent public management systems, we used data from the Global Burden of Disease (GBD) 2021 to analyse the prevalence and incidence of psoriasis in children and adolescents (0–19 years) at the global, regional, and national levels. The WHO views psoriasis as a critical global health issue due to its substantial psychological and social effects on young people with limited treatment choices. Our study backs their call for age-specific epidemiological data for better policy-making [1].
Methods
The GBD employs an array of stringent methodologies, such as meticulous literature appraisals, analysis of healthcare facility records, and insurance billing information, coupled with exhaustive nationwide health assessments, to generate optimal projections regarding the worldwide disease burden. We obtained information from the Global Health Data Exchange and focused on the burden of psoriasis in individuals under 20 years of age at the global, regional, and national levels. These data were categorised into four age groups: under 5 years (0–4 years), 5–9, 10–14, and 15–19. Twenty-one regions, 204 countries and territories, and five sociodemographic index (SDI) regions were included in the analysis. The SDI classifies regions into high, high-middle, middle, low-middle, and low based on birth rates, education, and income, aiding health studies and policy formulation [3]. The measures used were the number, rate, and age-standardised rates of prevalence, incidence, and disability-adjusted life years (DALYs). We calculated and compared the age-standardised prevalence rate (per 100,000 people), age-standardised incidence rate (per 100,000 people), and age-standardised DALY rate (per 100,000 people) of psoriasis across various age groups, sexes, regions, and countries. Subsequently, we leveraged joinpoint regression analysis to compute the average annual percentage change (AAPC) to depict the trajectory of psoriasis between 1990 and 2021. Finally, the Bayesian Age-Period-Cohort (BAPC) model was used to predict the incidence and prevalence of psoriasis in children and adolescents. All statistical analyses were conducted using the Joinpoint Regression program (version 5.0.2) and R (version 4.4.1), and our forecast considered the GBD 2017 population projections.
Results
Globally, the prevalence, incidence, and DALYs of psoriasis in children and adolescents showed an increasing trend, and the upward trends in all three indicators were similar. Between 1990 and 2021, the age-standardised prevalence, incidence, and DALYs rate of psoriasis in this age group increased by 28%, 8.5%, and 9.6%, with AAPCs of 0.28%, 0.26%, and 0.29%, respectively (Table I, Supplementary Tables SI and SII). Notably, the increasing trend in the age-standardised prevalence and DALYs rates of children and adolescents were more evident than that of the overall population with psoriasis from 1990 to 2021 while the increasing trend of incidence was less significant than in the overall population with psoriasis (Supplementary Figure S1). Moreover, the proportion of DALYs attributed to psoriasis in relation to all causes has steadily increased over the last 32 years among children and adolescents (Supplementary Figure S2). Considering gender, the increasing trends in the prevalence, incidence and DALYs of psoriasis among young people were more rapid in males than in females (AAPC: 0.33% vs. 0.25%, 0.32% vs. 0.21%, 0.33% vs. 0.25%). However, the prevalence, incidence and DALYs of psoriasis in females in 1990 and 2021 were higher than in males (Table I, Supplementary Table SI and SII). From the perspective of age subgroup, the burden of psoriasis in each age category in those under 20 years demonstrated a clear increasing pattern. In general, age-standardised prevalence, DALYs, and incidence rates all increased with age, whereas the AAPCs for prevalence and DALYs decreased with age. The age-standardised prevalence rate of psoriasis increased the most rapidly in the 0–4 years group, from 102 per 100,000 people to 113 per 100,000 with an AAPC of 0.32%. In contrast, the age-standardised prevalence rate increased the slowest in the 15–19 years group, from 287 per 100,000 people to 310 per 100,000 with an AAPC of 0.25% (Table I). The most significant increases in age-standardised DALY and incidence rates associated with psoriasis were also observed among those aged 0–4 years with AAPCs of 0.44% and 0.43%. When considering SDI, between 1990 and 2021, the age-standardised prevalence, incidence, and DALY rates all increased with SDI in 1990 and 2021, whereas the highest prevalence, incidence, and DALYs were found in countries with a middle SDI. Furthermore, the age-standardised prevalence, incidence, and DALY rates of females were consistently higher than those of males, regardless of changes in SDI (Supplementary Figure S4). In these subgroups, there were no significant differences in the AAPCs of the three indicators between males and females (Supplementary Figure S5). Except in nations with a low-middle SDI, the increasing trend of psoriasis burden in this age group was consistently higher than that in all ages (Supplementary Figure S1 and S6).
Table I
Age-standardised prevalence of psoriasis in young people and their AAPCs from 1990 to 2021 at the global and SDI levels
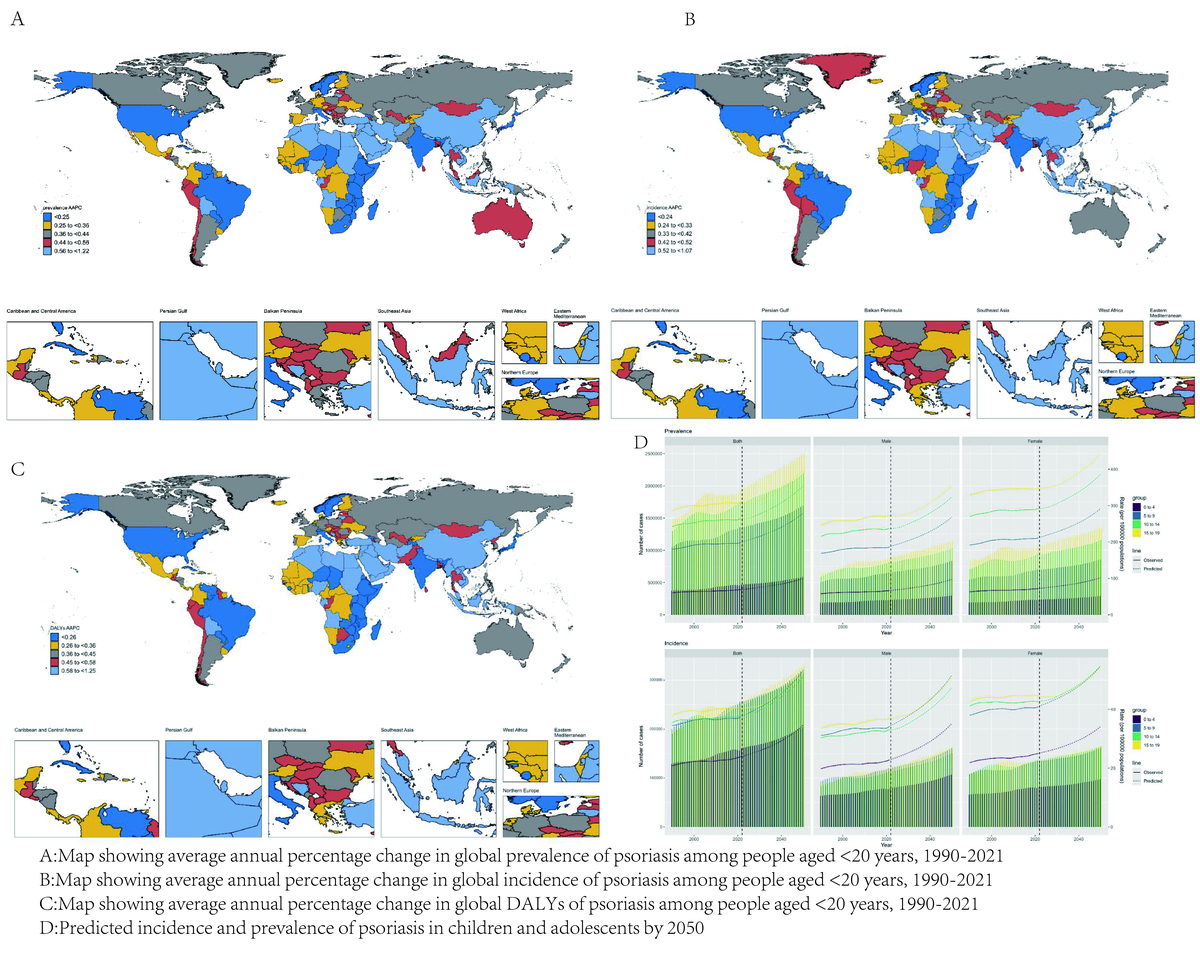
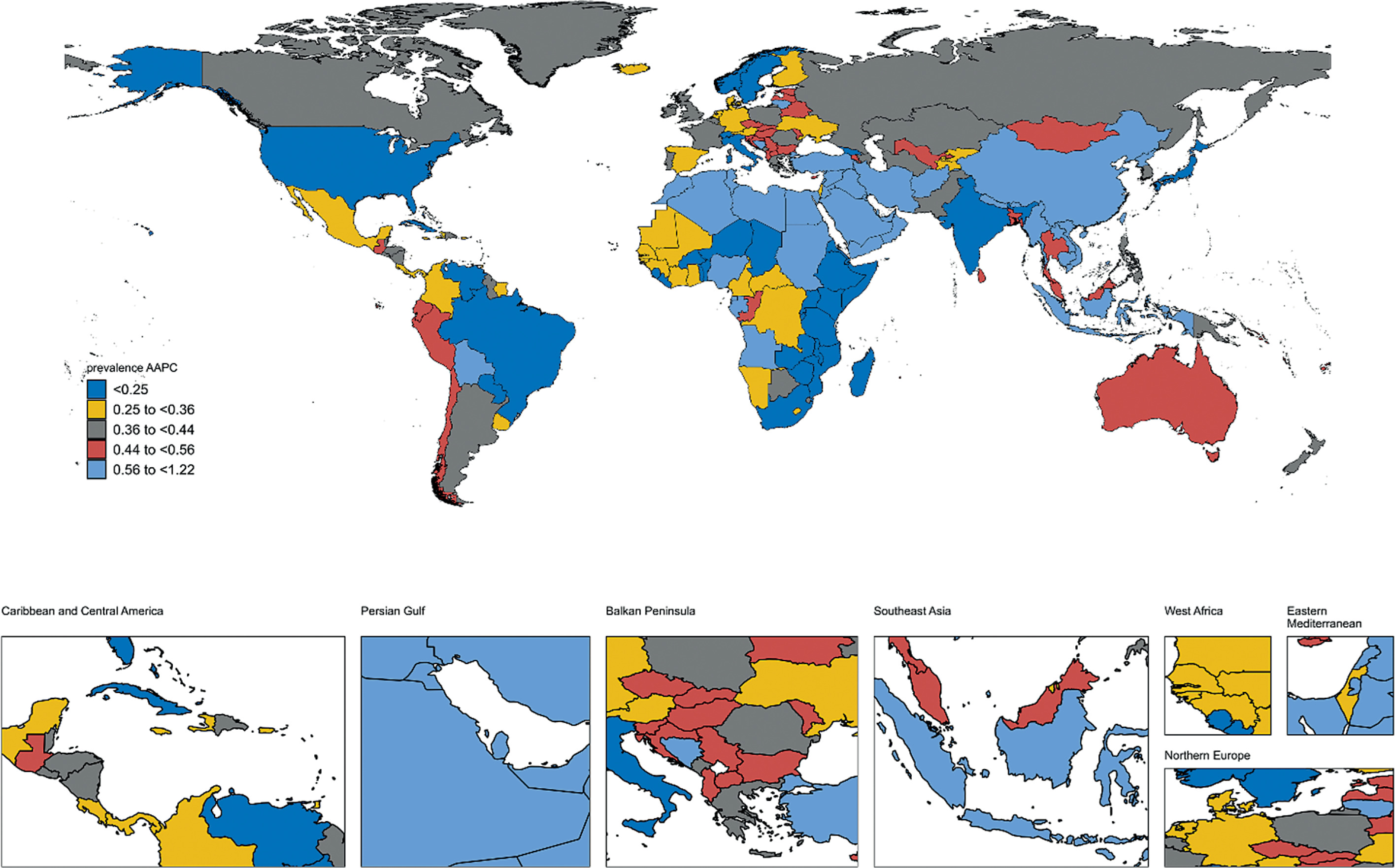
From the perspective of regions, the burden of psoriasis increased in almost all 21 regions. Only in high-income North America the prevalence and DALYs of psoriasis among children and adolescents showed statistically non-significant decreasing trends with AAPCs of –0.03% (95% CI: –0.1% to 0.04%) and –0.04% (95% CI: –0.1% to 0.02%). The increase in age-standardised prevalence, incidence, and DALY rates for children and adolescents with psoriasis was particularly evident in East Asia (AAPC of 0.89%, 0.86%, and 0.9%), followed by North Africa and the Middle East (AAPC of 0.76%, 0.73%, and 0.77%). At the national level, from 1990 to 2021, Equatorial Guinea saw the most significant trend in the growing burden of psoriasis among children and adolescents (AAPC for prevalence: 1.22%; AAPC for incidence: 1.07%; AAPC for DALYs: 1.25%), followed by Oman (AAPC for prevalence: 1.1%; AAPC for incidence: 1.01%; AAPC for DALYs: 1.13%), Sudan (AAPC for prevalence: 1.01%; AAPC for incidence: 0.94%; AAPC for DALYs: 1%) and Saudi Arabia (AAPC for prevalence: 1.01%; AAPC for incidence: 0.93%; AAPC for DALYs: 1.01%) (Supplementary Table SIII, SIV, Figure 1, and Supplementary Figures S7, S9, S10). In our prediction, according to Supplementary Figure S11 and Supplementary Table SV, we anticipate a rise in the global prevalence and incidence per 1,000 individuals, from 5,504 cases in 2022 to 6,982 by 2050 and from 921 cases in 2022 to 1,172 in 2050, respectively. Moreover, the age-standardised prevalence and incidence rates across all four age groups are also expected to show an upward trajectory. For more content, please refer to our supplementary documents.
Figure 1
Map showing average annual percentage change in global prevalence of psoriasis among people aged < 20 years, 1990–2021
Generally, the burden of psoriasis among this demographic continuously increased; however, it varied across regions and countries. The rising incidence and prevalence, consistent with WHO’s observed global trends [1], may attribute to the increased detection rate of psoriasis in children and adolescents as paediatric psoriasis has received increasing attention, and diagnostic methods for this condition have improved with the use of biopsy and dermoscopy [4]. This DALY increase may be attributed to the difficulty of treating children with psoriasis. Drug options for children remain limited, and guidelines for the systemic treatment of psoriasis in children and adolescents are still lacking [5]. Previous studies have linked regions with greater societal privileges and wealthier inhabitants to a higher burden of psoriasis. In contrast, communities with more modest financial resources have demonstrated a lower burden of this condition [6, 7]. This is consistent with our results; however, we found that an increase in the burden of psoriasis in nations with middle and high-middle SDI was particularly prominent. This phenomenon requires further research and meticulous analysis. Many studies have delved into the disparities that exist between the sexes. In the entire population, it is commonly believed that the incidence of psoriasis among females is higher than in males, but several studies support the opposite conclusion [8, 9]. In our study, we found that among children and adolescents, the burden of psoriasis in females was much more serious than that in males, whereas the increasing trend was higher in males than in females. The causes behind these disparities remain elusive. Only 19% of countries report psoriasis epidemiology, with most data from the US and Europe focusing on adults [10]. Research from these countries shows varying results in children, likely due to differences in reporting and criteria. Higher latitudes may have a higher prevalence [11]. Our findings indicate that psoriasis in children is primarily in high-income North America, Andean Latin America, and Western Europe, aligning with previous studies. However, the rising burden in East Asia, North Africa, and the Middle East suggests a need for targeted prevention and management efforts in these regions. Increased future prevalence highlights the need for more attention to paediatric cases.
Our research has limitations: the GBD 2021 data, based on a statistical model, may not reflect reality; no mortality data for psoriasis were available, limiting analysis to prevalence and incidence; and paediatric severity and comorbidities were unexamined. The data also exhibit a temporal lag. Confirmatory studies with robust methodologies are necessary.
In conclusion, from 1990 to 2021, the burden of psoriasis among children and adolescents increased. Future trends suggest continued escalation of this burden, underscoring the urgent need for age-specific management strategies as advocated in the WHO Global Report on Psoriasis [1]. These findings call for targeted interventions prioritizing early diagnosis and equitable treatment access.
Data sharing statement
The data used for analyses are publicly available at https://ghdx.healthdata.org/gbd-results-tool. All data will be made available on request to the corresponding author. Proposals will be reviewed and approved by the sponsor, investigator, and collaborators based on scientific merit. After approval of a proposal, data will be shared through a secure online platform after the signing of a data access agreement.