Introduction
In the era of the COVID-19 pandemic, the management of non-communicable diseases (NCDs) becomes challenging. The World Health Organization (WHO) reported significant disruptions in NCD-related services due to the virus spread. Dental care, rehabilitation and palliative care appeared to be the most affected domains as shown in a survey of 163 countries [1]. Nevertheless, the management of other NCDs such as hypertension (HTN), diabetes and cancer suffered similar disturbances [1]. National health systems around the world responded to this invisible threat by employing adjustments to the health care system including cancellations of elective procedures and outpatient visits. Part of the available resources was shifted to support the increased demand for inpatient care or to control viral transmission. On the other hand, patient attendance at hospitals showed a significant decline. The fear of potential contagion was identified as the main cause for this population behavior [2–5]. These changes in medical services along with the patients’ feeling of insecurity limited the global effort to control NCDs.
The HTN community experienced additional COVID-19-related stress and uncertainties. Hypertensive patients appeared to be more susceptible to the virus than normotensives ones and uncontrolled HTN was associated with worse disease outcomes [6–14]. Contradictory reports regarding renin-angiotensin system (RAS) blockers [15, 16] created additional confusion to the public, which according to a recently published survey among centers of excellence of the European Society of Hypertension (ESH) prompted part of the population to discontinue treatment [17]. Increased anxiety and treatment discontinuation can adversely affect blood pressure (BP) control, reflecting on the incidence of hypertensive urgencies (HTNu) and emergencies (HTNe). HTNu are usually defined as acute episodes of marked BP rise and differ from HTNe events as they are not related to evidence of new target organ damage and they are frequently asymptomatic [18, 19]. These episodes account for a large percentage of the total visits to the emergency department, being also linked to increased morbidity and mortality [18–23].
The aim of the present study was to investigate the population behavior regarding HTNu during the first wave of the COVID-19 pandemic.
Material and methods
This study is an observational, retrospective analysis of unscheduled visits for HTNu in the Emergency Cardiology Department (ECD) of a tertiary University General Hospital in the metropolitan area of Athens, Greece. Under normal circumstances, outpatient HTN care in this hospital has been provided by two HTN clinics and one center of excellence, accommodating more than 5000 scheduled visits per year. The study period was set to include the first wave of the COVID-19 pandemic and ranged between January 15th and July 14th, 2020. The findings were compared with the respective period of the previous year. The first confirmed COVID-19 case in Greece was reported on February 26th, 2020, whereas a complete lockdown was imposed on March 10th, 2020. During the study period, the hospital remained open to the public for general emergencies and it was not limited to COVID-19 infected patients. On the contrary, it was not dedicated to hospitalized confirmed COVID-19 cases. The study period was intentionally selected to start prior to the coronavirus spread in Greece and to include several months after the cancellation of the restrictive measures, which happened on May 4th, 2020. Population behavior towards hypertensive urgencies was evaluated upon the trends of unscheduled visits for uncontrolled hypertension during the aforementioned period which were compared with the ones of the previous year.
The study was carried out following standard ethics requirements according to the Helsinki Declaration with the permission of the hospital’s Bioethics Committee (ref number 3521, May 2020).
Data were retrieved from the ECD visitor’s registry. All unscheduled visits during the study period were extracted and discriminated by sex, age, reason for visit, initial diagnosis and outcome. The three different outcomes of interest were hospital admission, death in ECD and discharge. For the present study, all patients with HTNu or diagnosis of HTN on admission were analyzed separately. HTNu was defined according to the current European Society of Cardiology/European Society of Hypertension (2018 ESC/ESH) guidelines [20]. HTN diagnosis on admission refers to cases admitted to the hospital due to uncontrolled HTN, taking or not taking antihypertensive medication.
Statistical analysis
All categorical variables are shown as absolute and relative (%) frequencies, while the age variable is shown as mean ± standard deviation (SD). Visits are presented as counts. For the purposes of this analysis, the ratio of HTN diagnoses on admission was calculated as the number of patients with HTN diagnoses/total incidents per time period. Pearson’s χ2 and Student’s t-test statistics were used for simple bivariate comparisons, depending on the type of variable. Time-series analysis using Poisson function and linear trend modeling were conducted in order to evaluate the pattern of admissions and visits by time periods (weeks or half-month periods). To further investigate the pattern, other non-linear trends (parabolic and polynomial) were also tested. Cross-correlation analysis was also applied between the national COVID-19 confirmed cases and visits at the ECD from February 26th (the first confirmed case in Greece) to July 15th, 2020. All tested hypotheses were two-sided at a significance value of p < 0.05. All statistical analyses were performed using the Stata SE 16 software (STATA Corp Ltd., Texas, USA).
Results
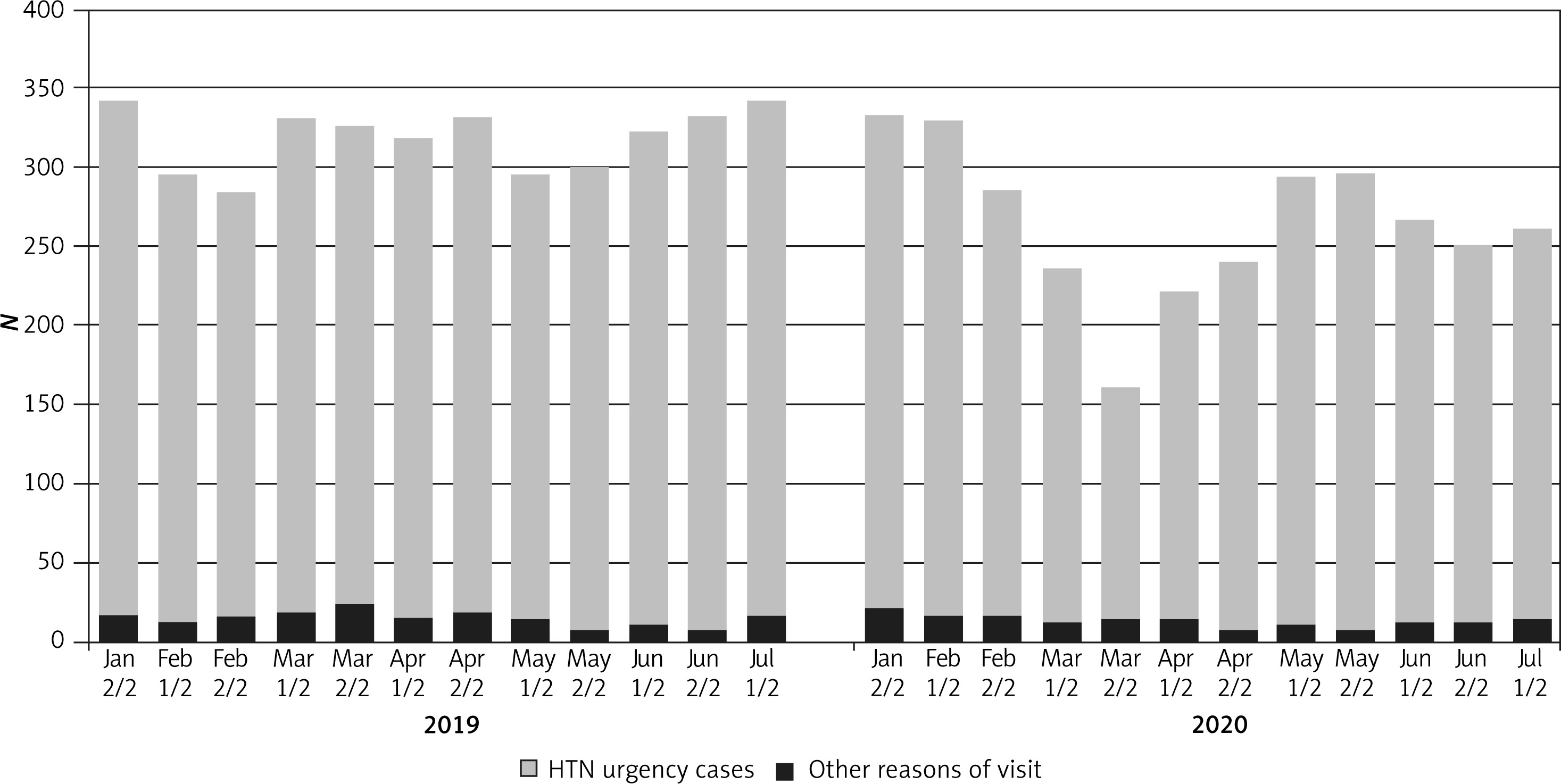
A total of 7,373 patients records were used for this study. The descriptive characteristics of the participants are shown in Table I. Admissions to the hospital for uncontrolled HTN and cases of HTNu during the first wave of the COVID-19 pandemic were compared with the respective events during the same period of the previous year. Overall distribution of gender and course was different between 2019 and 2020. A higher percentage of women (43.5%) visited the ECD during the first months of 2020 compared with 2019 (41.1%) (p = 0.035). The relative frequency of all-cause admissions during the period between January 15th and July 15th, 2020 was significantly higher than the corresponding frequency during the same period in 2019 (i.e., 47.4 vs. 43.8%, p = 0.007) (Figure 1). The overall mean age of admitted patients was 64.1 ±18.1 years and it was similar between patients admitted in 2020 and 2019 (p = 0.856). Moreover, there were no differences in the pattern of reason for visit to the ECD (HTNu vs. other) (Figure 2) or the final diagnosis (p = 0.397 and 0.612, respectively).
Table I
Descriptive statistics of the study population
Figure 1
Distribution of the outcomes after the visits of patients in the emergency department of a tertiary hospital in Athens, Greece, during January–July (in 2019 and 2020, respectively)
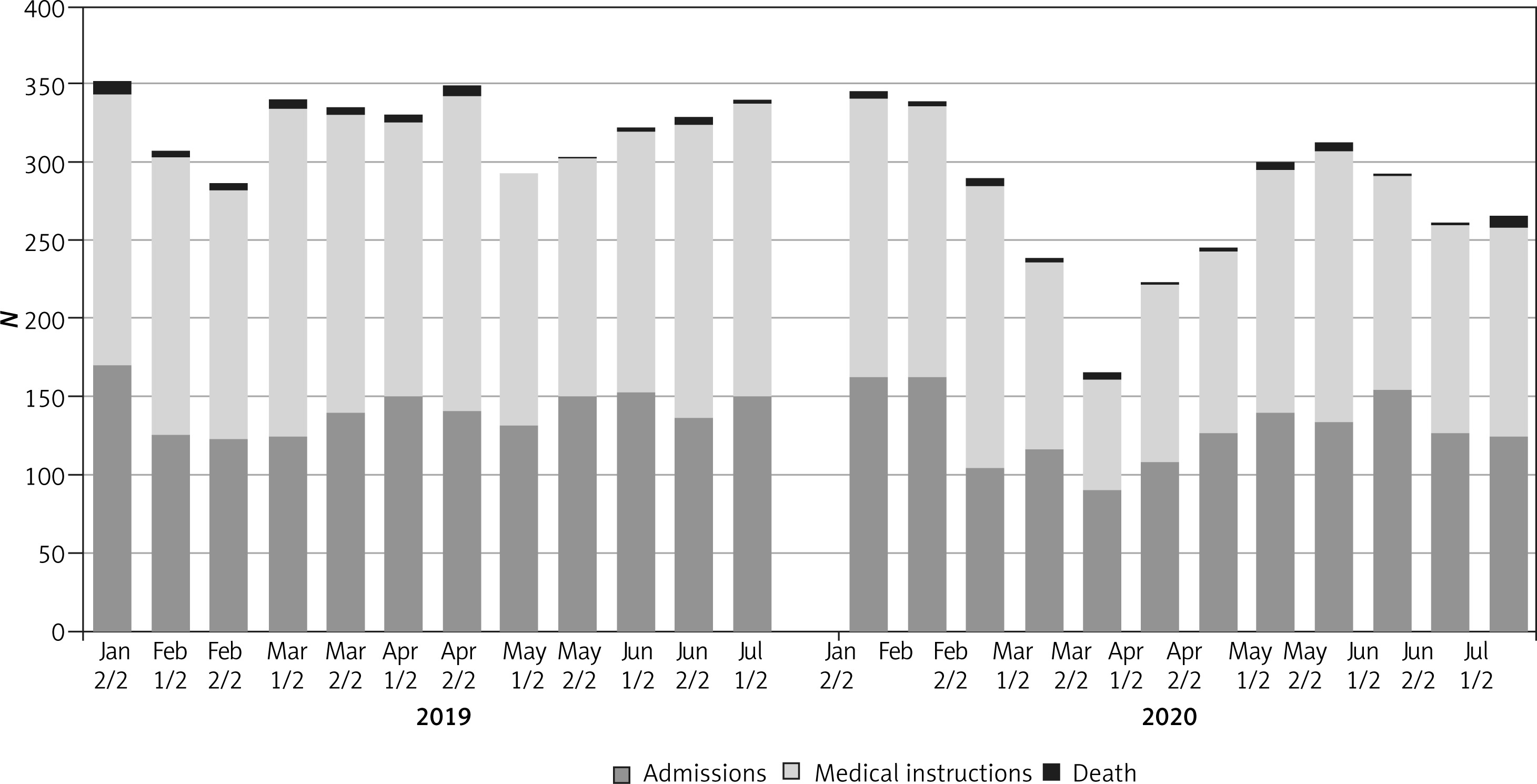
Figure 2
Distribution of the presenting reasons for visits in the emergency department of a tertiary hospital in Athens, Greece, during January–July (2019–2020)
HTN – hypertension.
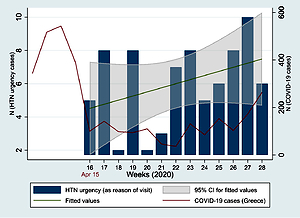
The number of patient visits at the ECD with HTNu demonstrated a U-shaped pattern during the first months of 2020 (p = 0.001) (Figure 3), following a quadratic non-linear trend. This pattern was not observed during the similar period of 2019 (p = 0.707). More specifically, there was a significant reduction in cases from January 15th to April 15th, 2020, when the COVID-19 cases increased in Greece (p for linear trend = 0.045, Figure 3).
Figure 3
Hypertension (HTN) urgency (as reason of visit) cases trend by half-month periods in 2019 and 2020. COVID-19 cases in Greece are also shown with the red line in the 2020 graph
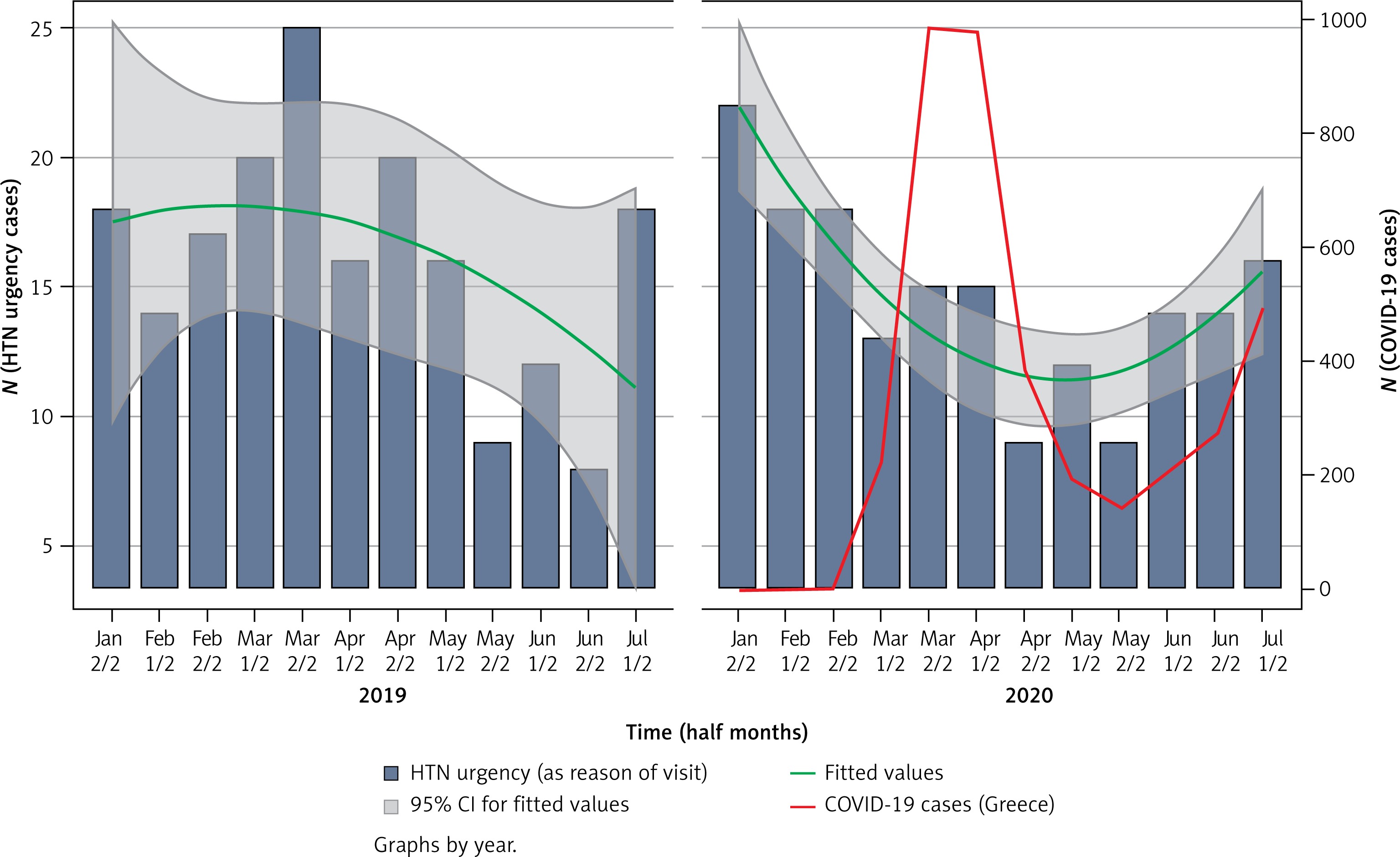
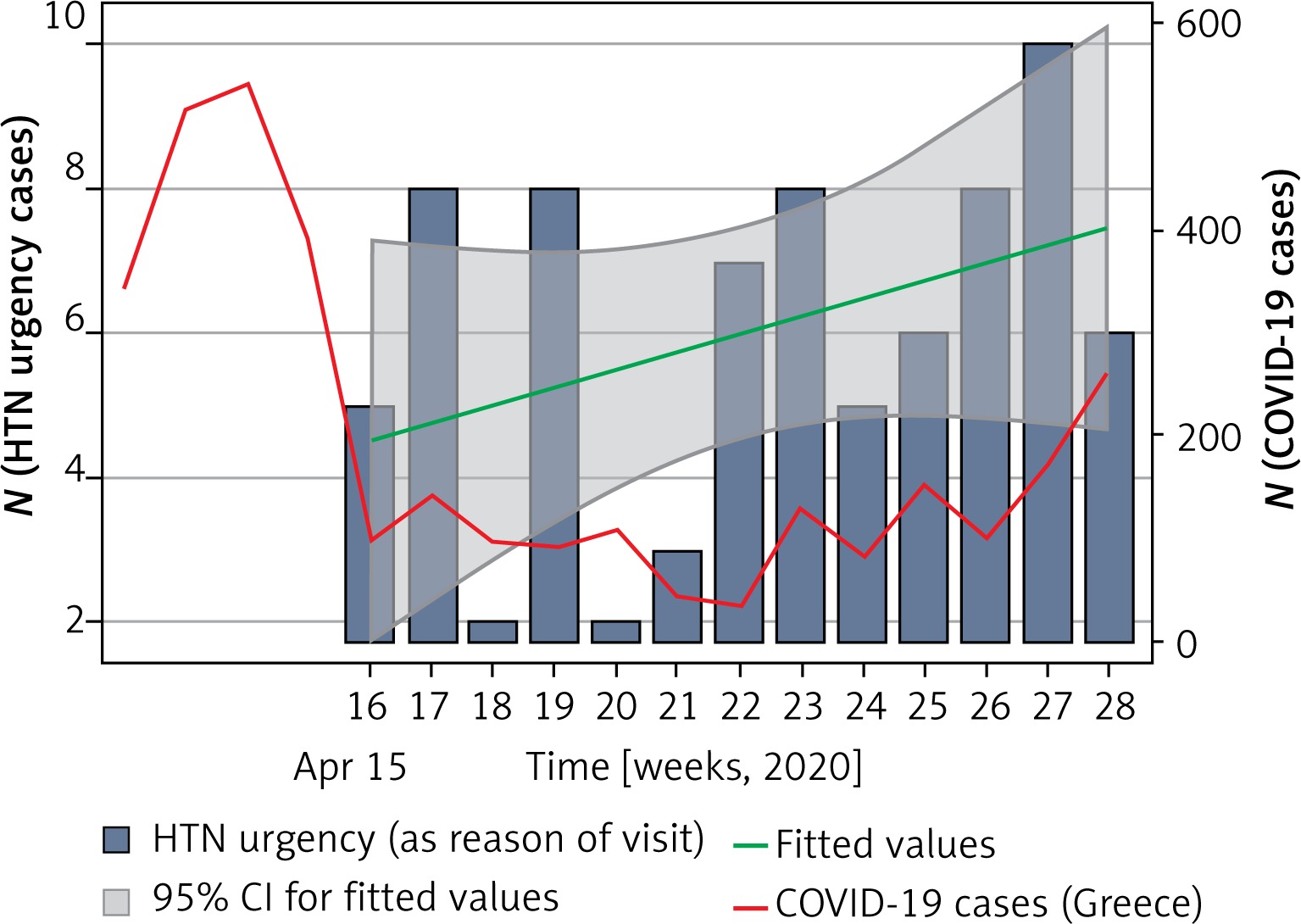
In contrast, a significant increase was reported from April 15th to July 15th, 2020, when the national COVID-19 cases decreased and remained low for a period of time (p for linear trend = 0.030) (Figure 4). Such trends did not appear during the same time periods of 2019 (p = 0.480 and 0.514, respectively).
Figure 4
Linear increasing trend of hypertension (HTN) urgency cases (as reason of visit) and COVID-19 cases in Greece by week time periods in 2020, after the reduction of the COVID-19 cases
In cross-correlation analysis a significant inverse association was observed between the number of confirmed national COVID-19 cases and the HTN related admissions to our hospital, i.e., as the number of COVID-19 cases declined, the number of admissions increased (r = –0.64, lag 7 days, p = 0.009). The same type of inverse association was evident between the number of COVID-19 cases and the number of total visits both during the increase (from Feb 26th to April 2nd, 2020) and during the decrease (April 3rd to July 15th, 2020) of COVID-19 cases in Greece (r = –0.677, p = 0.031 and r = –0.789, p = 0.001, respectively). There was also a significant positive correlation between the number of national COVID-19 cases and the percentage of HTN as diagnosis on admission among the number of total incidents during the start of the pandemic in Greece (from Feb 26th to April 2nd, 2020) (r = 0.82, lag 7 days, p = 0.045).
Discussion
The main finding of the present study is the significant reduction in the absolute number of visiting patients presenting with HTNu after the spread of SARS-CoV-2 in Greece. This trend appeared to reverse later, when the pandemic in the country started to decrease (Figure 3). This U-shaped pattern of HTNu followed a similar trend to all-cause attendance in the ECD during the pandemic expansion (Figure 2). In contrast, HTNu cases in 2019 showed a continuous declining trend inversely related to the environmental temperature increase, which could reflect the principle of seasonal BP variability [24].
The phenomenon of a reduced visit rate to the emergency department for cardiovascular causes has already been discussed by our team during the first months of the COVID-19 pandemic [2], as well as by other investigators [25, 26]. In accordance, visits for specific cardiovascular emergencies, such as acute stroke or myocardial infarction (MI), have similarly decreased during the virus spread [3–5, 27–29]. Most of the authors attribute this trend to the fear of potential contagion, leading patients suffering from relevant events not to report to the emergency department. Additionally, the imposed restrictive measures on transportation, the local or national lockdowns and the regional campaigns promoting self-isolation have been suggested to increase the levels of stress and prevent part of the population from visiting the emergency department. The latter is further supported in our study by the increased relative frequency of all-cause admissions during the study period. It can be speculated that patients with less severe events avoided contacting the emergency department, whereas those patients visiting the emergency room were more likely to be admitted. The later increase in HTNu cases could represent hypertensive events that were neglected during the restrictive period, and the patients were not transferred to the emergency department. Interestingly, the number of HTNu visits started to increase before the cancellation of the lockdown measures, which happened on the 4th of May in Greece (Figure 4). The U-shaped curve appeared when the epidemic curve of new COVID-19 cases started to flatten. The ascending part of the U-shaped curve was observed only when the daily cases of COVID-19 stabilized to a low level, whereas the restrictive measures were still valid, suggesting that the sudden and violent spread of the virus had a more profound impact on stressing the public than the restrictive measures themselves.
Another explanatory approach could link the duration of the stressful stimulus (i.e., the COVID-19 threat) with the late increasing trend of the absolute number of HTNu cases. Accumulated stress could result in higher BP levels. The stressful condition of a HTNu or HTNe could overcome the weakened, over time, fear of contagion and lead more patients to seek medical advice, explaining the increasing HTN-related admissions during the ascending part of the U-shaped curve. This hypothesis is further strengthened by evidence that highlights the significant impact of the pandemic on mental health. Increased levels of anxiety, prevalence of depression, stress and insomnia have been attributed to the virus spread, which appeared to affect all the population. The largest impact was documented on infected patients and their relatives, followed by health workers and patients with chronic illnesses. Nevertheless, the general public has been affected too [30, 31]. Female gender, social isolation, low socio-economic status and the presence of chronic diseases, known to be related to a higher risk of severe COVID-19 infection, have all been presented as risk factors predisposing to increased levels of anxiety and depression related to the pandemic [30]. Interestingly, our results demonstrated women to have a higher rate of all-cause visits during the study period in 2020 compared with the previous year. This could be related to the aforementioned impact on mental health; however, our study does not include the necessary data to support it.
Based on retrospective epidemiological data, HTN was presented as a risk factor for increased susceptibility to COVID-19, increased disease severity and unfavorable outcomes [6–14]. Undoubtedly, this information made hypertensive patients feel vulnerable. In the meantime, the recognition of angiotensin-converting enzyme 2 (ACE2) as the facilitator of SARS-CoV-2 entry in humans [32, 33] raised significant concerns about the appropriateness of RAS blocker usage [15]. Theoretically, RAS blocker-induced ACE2 upregulation could predispose to an increased likelihood for or severity of a coronavirus infection. An opposing theory suggested that RAS inhibition could ameliorate the inflammatory cascade [16]. Consequently, both health workers and the public were confused about HTN treatment due to its potential effect on COVID-19 transmission and severity [34]. The first hypothesis prompted some of its supporters to advise against the initiation or continuation of this drug category during the pandemic [17, 35–37]. This practice was challenged in the light of insufficient evidence [34, 38–43]. Several scientific societies recommended against it, extenuating the preceding confusion regarding this cornerstone treatment which extends beyond HTN. Subsequent observational data suggested that HTN could not independently predict disease severity [41, 44–46] and also that RAS blocker usage could not influence the propensity to coronavirus or worse outcomes [15, 44, 47–50]. In contrast, HTN control with RAS inhibition in the COVID-19 cases may favor the prognosis [42, 51–55]. However, it is possible that a part of the hypertensive population discontinued such medications in the fear of possible complications. This would have also led to the observed early increased rate of HTN admissions and the late increase in HTNu visits.
In Greece, the Hellenic Society of Cardiology initiated a national awareness campaign to promote cardiovascular prevention and treatment policies in the COVID-19 era, initiated in mid-March 2020. In our study results, the HTNu cases started to increase 1 month after the implementation of the campaign. It is highly likely that this campaign itself may have affected people’s perspective in relation to HTN management. In combination with the virus spread interception, this may have also contributed to the ascending part of the U-shaped curve of our results. Similar findings were reported regarding stroke admission rates in the Greater Manchester and East Cheshire area [56]. Although stroke admission rates were reported to decline during the first wave of the pandemic [56–62], Gittins et al. demonstrated that this reduction was partially reversed after the imposition of a stroke awareness campaign [56].
However, untreated HTNu can progress to HTNe conditions. Unattended, severe HTNu patients could later suffer from an acute stroke. Hypothetically, in such events, these patients would be transferred to stroke-dedicated centers, bypassing the ECD, explaining part of the “missing” HTNu visits in our results. On the other hand, the later increase in stroke admission rate in the Gittins et al. study [55] could reflect untreated HTNu cases, leading to a stroke. Additionally, atrial fibrillation (AF) is a well-known cause of stroke, and uncontrolled HTN increases its incidence. Regional lockdowns have been associated with a reduced incidence of AF diagnosis, raising concerns about the detrimental implications of unattended cases [63]. On a theoretical basis, unattended HTNu cases could impact on more AF events and subsequently increased stroke incidence. Nevertheless, COVID-19 could have also influenced the stroke admission rates as the disease per se has been associated with increased stroke incidence [64–66].
Outpatient HTN care faced profound disturbance due to the restricting measures and social distancing. The ESH reported a significant decline to the number of hypertensive patients evaluated or treated in excellence centers, reaching the percentage of 90% during the complete lockdown period [17]. The same disruption occurring simultaneously with the lockdown in Greece may have also influenced the increase in HTNu visits after April 15th, 2020. Our hospital covers a large urban area in which HTN management is being practiced in outpatient clinics, either public or private. The government offered the opportunity of renewing prescriptions for chronic illnesses, including antihypertensive medications via virtual (over the phone) consultations. However, the available infrastructure and personnel were not adequate to accommodate all needs, and telemedicine, although helpful [67], was not technically feasible in most cases. The pandemic presented a big challenge for both the public and health care professionals and took a considerable length of time to adopt. Consequently, from our experience, there was a significant disturbance in HTN management which in any case mandates the presence of an integral, dedicated and focused health care system. This would have also contributed to the increased relative frequency of HTNu cases during all the studied period compared with 2019.
A rather interesting finding was that the ratio of attendance for HTNu/all visits in the period with the least total attendance (last 2 weeks of March 2020, Figure 2) was actually increased and was significantly higher than the corresponding ratio for 2019. We could suggest that this result may reflect an actual increase in BP levels, leading to proportionally more frequent events of HTNu. A similar trend in BP values was described after disasters such as the 2011 earthquake in Japan and has been labeled as “disaster HTN” [68–71]. Although our study sample could not be considered sufficient to conclude whether a “disaster HTN” effect was present in the global threat of COVID-19, this theory could explain the early increase in the relative frequency of HTN diagnosis.
We acknowledge that comparing more than one of the preceding years with the studied period would offer added value to our results. Another limitation of our study is that our data do not include the necessary information to present the trends of HTNe cases during the studied period as many of these cases may have been registered under other diagnoses, such as MI or acute heart failure. In the same line, our ECD does not receive stroke referrals, which account for a remarkable percentage of HTNe cases. Moreover, part of the reduction in HTNu cases could represent patients who selected an alternative health care provider. However, our hospital was not dedicated to hospitalized COVID-19 cases and it was considered to be among the safe ones during the studied period. On the other hand, the number of HTN diagnoses on admission could reflect the incidence of HTN emergencies. The acceptance of such an assumption would indicate that HTN emergencies were probably increased during the studied period but we cannot support it adequately.
To the best of our knowledge, the present study is the first to evaluate the impact of COVID-19 on the incidence of HTNu in an emergency department. Our results highlight the profound difference in population behavior towards HTNu during the first wave of the pandemic which seems to be severely affected by the coronavirus spread and to a lesser extent by the implementation of restrictive measures. The observed relative increase of hypertension related admissions raises concerns that overall hypertension control was significantly affected during the studied period.
Taking into consideration the anticipated subsequent phases of the pandemic and based on our observations, we could suggest several measures to avoid similar disturbance in hypertension care. Hypertension clinics’ regular operation needs to be restored with all the necessary protective measures available. Telemedicine applications together with over the phone consultations on a daily basis including out of hours service could provide reliable help to hypertensive subjects who prefer to avoid direct visits. Informative campaigns about the prompt screening, monitoring and hypertension treatment are of high value in order to keep the public alert about the potential dangers of neglecting uncontrolled blood pressure levels.
In conclusion, HTNu in absolute numbers followed a U-shaped curve, similar to other cardiovascular conditions, during the first wave of the COVID-19 pandemic, in terms of ECD attendance in a tertiary General Hospital in Athens, Greece. Stress in combination with the disrupted HTN outpatient care system and the impact of the national campaign to clarify potential misconceptions about HTN management seem to be the main contributors of these findings. Uncontrolled HTN can provoke a domino effect in cardiovascular mortality and morbidity, increasing the incidence of disabling events such as stroke or MI. Furthermore, untreated HTN is linked to unfavorable COVID-19 outcomes. A well-structured system for outpatient HTN management is of great value, which, in the context of the continuously growing pandemic, needs to integrate urgently with applications of telemedicine to offer a safe follow-up in the patients’ safe environment.