Current issue
Archive
Manuscripts accepted
About the Journal
Editorial office
Editorial board
Section Editors
Abstracting and indexing
Subscription
Contact
Ethical standards and procedures
Most read articles
Instructions for authors
Article Processing Charge (APC)
Regulations of paying article processing charge (APC)
PULMONOLOGY / CLINICAL RESEARCH
Intra-abdominal pressure for predicating extubation failure in mechanically ventilated patients: it does work
1
Department of Nursing, Changshu First People’s Hospital, Soochow, China
2
Department of Respiratory and Critical Care Medicine, the First Affiliated Hospital of Soochow University, Soochow, China
3
Department of Nursing, Dushu Lake Hospital Affiliated to Soochow University, Soochow, China
Submission date: 2021-07-27
Final revision date: 2021-08-30
Acceptance date: 2021-09-01
Online publication date: 2021-09-17
KEYWORDS
TOPICS
ABSTRACT
Introduction:
Reducing extubation failure is vital to the early recovery of pa- tients with mechanical ventilation (MV). We aimed to explore the predictive value of the change of intra-abdominal pressure (ΔIAP) before extubation for the extubation failure of MV patients.
Material and methods:
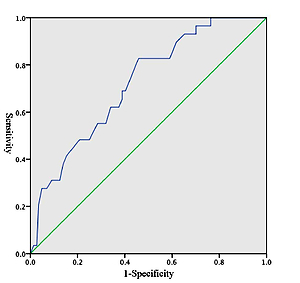
failure of MV patients. Material and methods: Patients undergoing MV for more than 24 h were selected. We used a urodynamic monitor to measure ΔIAP 30 min before extubation. The characteristics and prognosis of MV patients were analyzed. A receiver operating characteristic (ROC) curve was drawn to analyze the predictive value of ΔIAP for extubation failure.
Results:
A total of 173 MV patients were included. The risks of extubation failure increased with the decrease of ΔIAP. The risk of extubation failure in the ΔIAP ≤ 21 mm Hg group was 5.7 times that of the ΔIAP ≥ 38 mm Hg group (OR = 5.7, 95% CI: 1.5–22.0), the risk of extubation failure in the ΔIAP 22–37 mm Hg group was 3.8 times that of the ΔIAP ≥ 38 mm Hg group (OR = 3.8, 95% CI: 1.0–15.3). The area under the curve (AUC) predicted by ΔIAP for extubation failure was 0.721, the cutoff value was 31 mm Hg with 82.8% sensitivity and 48.6% specificity. There were no significant differences in the duration of MV, length of ICU stay, and death in ICU of the three groups of patients (all p > 0.05).
Conclusions:
The ΔIAP has good reference value for predicting extubation failure, which is negatively correlated with the risk of extubation failure in patients with MV. For MV patients with ΔIAP ≤ 31 mm Hg, they may have higher risk of extubation failure; early alert and interventions are highlighted for those patients.
Reducing extubation failure is vital to the early recovery of pa- tients with mechanical ventilation (MV). We aimed to explore the predictive value of the change of intra-abdominal pressure (ΔIAP) before extubation for the extubation failure of MV patients.
Material and methods:
failure of MV patients. Material and methods: Patients undergoing MV for more than 24 h were selected. We used a urodynamic monitor to measure ΔIAP 30 min before extubation. The characteristics and prognosis of MV patients were analyzed. A receiver operating characteristic (ROC) curve was drawn to analyze the predictive value of ΔIAP for extubation failure.
Results:
A total of 173 MV patients were included. The risks of extubation failure increased with the decrease of ΔIAP. The risk of extubation failure in the ΔIAP ≤ 21 mm Hg group was 5.7 times that of the ΔIAP ≥ 38 mm Hg group (OR = 5.7, 95% CI: 1.5–22.0), the risk of extubation failure in the ΔIAP 22–37 mm Hg group was 3.8 times that of the ΔIAP ≥ 38 mm Hg group (OR = 3.8, 95% CI: 1.0–15.3). The area under the curve (AUC) predicted by ΔIAP for extubation failure was 0.721, the cutoff value was 31 mm Hg with 82.8% sensitivity and 48.6% specificity. There were no significant differences in the duration of MV, length of ICU stay, and death in ICU of the three groups of patients (all p > 0.05).
Conclusions:
The ΔIAP has good reference value for predicting extubation failure, which is negatively correlated with the risk of extubation failure in patients with MV. For MV patients with ΔIAP ≤ 31 mm Hg, they may have higher risk of extubation failure; early alert and interventions are highlighted for those patients.
REFERENCES (41)
1.
Almeida CM, Lopes AJ, Guimaraes FS. Cough peak flow to predict the extubation outcome: Comparison between three cough stimulation methods. Can J Respir Ther 2020; 56: 58-64.
2.
Duan J, Zhou L, Xiao M, Liu J, Yang X. Semiquantitative cough strength score for predicting reintubation after planned extubation. Am J Crit Care 2015; 24: e86-90.
3.
Menon N, Joffe AM, Deem S, et al. Occurrence and complications of tracheal reintubation in critically ill adults. Respir Care 2012; 57: 1555-63.
4.
Lai CC, Chen CM, Chiang SR, et al. Establishing predictors for successfully planned endotracheal extubation. Medicine 2016; 95: e4852.
5.
Deschamps J, Andersen SK, Webber J, et al. Brain natriuretic peptide to predict successful liberation from mechanical ventilation in critically ill patients: a systematic review and meta-analysis. Crit Care 2020; 24: 213.
6.
Savla P, Toor H, Podkovik S, et al. A reassessment of weaning parameters in patients with spontaneous intracerebral hemorrhage. Cureus 2021; 13: e12539.
7.
Baptistella AR, Mantelli LM, Matte L, et al. Prediction of extubation outcome in mechanically ventilated patients: development and validation of the Extubation Predictive Score (ExPreS). PLoS One 2021; 16: e0248868.
8.
Lombardi FS, Cotoia A, Petta R, Schultz M, Cinnella G, Horn J. Prediction of extubation failure in intensive care unit: systematic review of parameters investigated. Minerva Anestesiol 2019; 85: 298-307.
9.
Miu T, Joffe AM, Yanez ND, et al. Predictors of reintubation in critically ill patients. Respir Care 2014; 59: 178-85.
10.
Thille AW, Richard JC, Brochard L. The decision to extubate in the intensive care unit. Am J Respir Crit Care Med 2013; 187: 1294-302.
11.
Nguyen AP, Schmidt UH. The strong cough: is it a signpost on the road to extubation or just a dead end? Respir Care 2017; 62: 1611-2.
12.
Duan J, Liu J, Xiao M, Yang X, Wu J, Zhou L. Voluntary is better than involuntary cough peak flow for predicting re-intubation after scheduled extubation in cooperative subjects. Respir Care 2014; 59: 1643-51.
13.
Gobert F, Yonis H, Tapponnier R, et al. Predicting extubation outcome by cough peak flow measured using a built-in ventilator flow meter. Respir Care 2017; 62: 1505-19.
14.
Su WL, Chen YH, Chen CW, et al. Involuntary cough strength and extubation outcomes for patients in an ICU. Chest 2010; 137: 777-82.
15.
Chittawattanarat K, Kantha K, Tepsuwan T. Central Venous oxygen saturation is not a predictor of extubation success after simple weaning from mechanical ventilation in post-cardiac surgical patients. J Med Assoc Thai 2016; 99 Suppl 6: S145-52.
16.
Abedini M, Froutan R, Bagheri Moghaddam A, Mazloum SR. Comparison of “cough peak expiratory flow measurement” and “cough strength measurement using the white card test” in extubation success: a randomized controlled trial. J Res Med Sci 2020; 25: 52.
17.
Thille AW, Boissier F, Muller M, et al. Role of ICU-acquired weakness on extubation outcome among patients at high risk of reintubation. Crit Care 2020; 24: 86.
18.
Shi ZH, Jonkman A, de Vries H, et al. Expiratory muscle dysfunction in critically ill patients: towards improved understanding. Intensive Care Med 2019; 45: 1061-71.
19.
Boles JM, Bion J, Connors A, et al. Weaning from mechanical ventilation. Eur Respir J 2007; 29: 1033-56.
20.
Bien MY, Shui Lin Y, Shih CH, et al. Comparisons of predictive performance of breathing pattern variability measured during T-piece, automatic tube compensation, and pressure support ventilation for weaning intensive care unit patients from mechanical ventilation. Crit Care Med 2011; 39: 2253-62.
21.
Xiao M, Duan J. Weaning attempts, cough strength and albumin are independent risk factors of reintubation in medical patients. Clin Respir J 2018; 12: 1240-6.
22.
Baptistella AR, Sarmento FJ, da Silva KR, et al. Predictive factors of weaning from mechanical ventilation and extubation outcome: a systematic review. J Crit Care 2018; 48: 56-62.
23.
De Jong A, Verzilli D, Sebbane M, et al. Medical versus surgical ICU obese patient outcome: a propensity-matched analysis to resolve clinical trial controversies. Crit Care Med 2018; 46: e294-301.
24.
Nemecek R, Nemecek E, Glaser C, Wallner T, Ratzinger F, Hollinsky C. Impact of two extubation techniques on the intra-abdominal pressure: a preliminary study. Hernia 2015; 19: 307-11.
25.
Goncalves EC, Silva EC, Basile Filho A, Auxiliadora-Martins M, Nicolini EA, Gastaldi AC. Low pressure support changes the rapid shallow breathing index (RSBI) in critically ill patients on mechanical ventilation. Rev Bras Fisioter 2012; 16: 368-74.
26.
Spadaro S, Grasso S, Mauri T, et al. Can diaphragmatic ultrasonography performed during the T-tube trial predict weaning failure? The role of diaphragmatic rapid shallow breathing index. Crit Care 2016; 20: 305.
27.
Wilson A, Longhi J, Goldman C, McNatt S. Intra-abdominal pressure and the morbidly obese patients: the effect of body mass index. J Trauma 2010; 69: 78-83.
28.
Smina M, Salam A, Khamiees M, Gada P, Amoateng-Adjepong Y, Manthous CA. Cough peak flows and extubation outcomes. Chest 2003; 124: 262-8.
29.
Abbas A, Embarak S, Walaa M, Lutfy SM. Role of diaphragmatic rapid shallow breathing index in predicting weaning outcome in patients with acute exacerbation of COPD. Int J Chron Obstruct Pulmon Dis 2018; 13: 1655-61.
30.
Goncalves EC, Lago AF, Silva EC, de Almeida MB, Basile-Filho A, Gastaldi AC. How mechanical ventilation measurement, cutoff and duration affect rapid shallow breathing index accuracy: a randomized trial. J Clin Med Res 2017; 9: 289-96.
31.
Woo HY, Oh SY, Lee H, Ryu HG. Evaluation of the association between decreased skeletal muscle mass and extubation failure after long-term mechanical ventilation. Clin Nutr 2020; 39: 2764-70.
32.
Winck JC, LeBlanc C, Soto JL, Plano F. The value of cough peak flow measurements in the assessment of extubation or decannulation readiness. Rev Port Pneumol 2015; 21: 94-8.
33.
Iyer D, Hunt L, Frost SA, Aneman A. Daily intra-abdominal pressure, sequential organ failure score and fluid balance predict duration of mechanical ventilation. Acta Anaesthesiol Scand 2018; 62: 1421-7.
34.
Gaidukov KM, Raibuzhis EN, Hussain A, et al. Effect of intra-abdominal pressure on respiratory function in patients undergoing ventral hernia repair. World J Crit Care Med 2013; 2: 9-16.
35.
Swingwood E, Stilma W, Tume L, et al. The use of mechanical insufflation-exsufflation in invasively ventilated critically ill adults: a scoping review protocol. Syst Rev 2020; 9: 287.
36.
Kaur R, Dass B, Ejaz AA, Singh A. Chest physiotherapy in acute muco-obstructive lung disease. Cureus 2020; 12: e7056.
37.
Liu X, Li Y, He W, Xu Y, Sang L. The application of fibrobronchoscopy in extubation for patients suffering from acute exacerbation of chronic obstructive pulmonary disease with low cough peak expiratory flow. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue 2014; 26: 855-9.
38.
Yildirim ZB, Uzunkoy A, Cigdem A, Ganidagli S, Ozgonul A. Changes in cuff pressure of endotracheal tube during laparoscopic and open abdominal surgery. Surg Endosc 2012; 26: 398-401.
39.
Veyckemans F. Tracheal extubation in children: planning, technique, and complications. Paediatr Anaesth 2020; 30: 331-8.
40.
Norisue Y, Kataoka J, Homma Y, et al. Increase in intra-abdominal pressure during airway suctioning-induced cough after a successful spontaneous breathing trial is associated with extubation outcome. Ann Intensive Care 2018; 8: 61.
41.
Rose L, Adhikari NK, Leasa D, Fergusson DA, McKim D. Cough augmentation techniques for extubation or weaning critically ill patients from mechanical ventilation. Cochrane Database Syst Rev 2017; 1: CD011833.
Share
RELATED ARTICLE
| eISSN: | 1896-9151 |
| ISSN: | 1734-1922 |
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.