Introduction
Cerebral circulation disorders are one of the main causes of mortality and permanent disability. According to American data, when considered separately from other cardiovascular diseases, stroke ranks fifth among all causes of death, behind diseases of the heart, cancer, chronic lower respiratory tract disease, and unintentional injuries [1]. Cerebral small vessel disease (CSVD) refers to a group of pathological processes with various aetiologies, which affect the small arteries, arterioles, venules, and capillaries of the brain. The consequences of CSVD on the brain parenchyma can be detected in neuroimaging studies and consist mainly of lesions located in the subcortical structures such as lacunar infarcts, white matter lesions, large haemorrhages, and microbleeds. Clinical implications of CSVD are as follows: increased risk of ischaemic stroke, disability, and cognitive decline in the elderly. Because this constitutes an important and – as we can anticipate in connection with the aging of society – growing problem, attention should be directed to modifiable risk factors. The link between hypertension, obesity, hyperglycaemia, hyperlipidaemia, renal dysfunction, behavioural factors (smoking, sedentary lifestyle, unhealthy diet), and CSVD is recognised and documented [2, 3]. Another significant factor associated with stroke risk is obstructive sleep apnoea (OSA). Obstructive sleep apnoea is characterised as the occurrence of apnoeas or hypopnoeas during sleep. The polysomnography-determined Apnoea–Hypopnoea Index (AHI) defines the severity of the disease. Apnoea–Hypopnoea Index between 5–15/h indicates mild OSA, whereas 15–30/h points to moderate OSA and > 30/h to severe OSA. It is a common disorder affecting millions of people. Data from the Wisconsin Cohort Study estimate the overall prevalence of OSA at 33.9% in men and 17.4% in women between 30 and 70 years of age, while moderate to severe OSA (defined by AHI > 15/h) affects 13.0% of men and 5.6% of women [4]. Large analyses indicate that severe OSA is associated with a doubling of stroke risk, higher post-stroke mortality, and worse functional outcome [5, 6]. The aim of our study was to assess the prevalence and association between CSVD and OSA in Polish subjects taking part in the Prospective Urban Rural Epidemiology (PURE) study, which is a population cohort study of individuals from urban and rural communities from 21 countries.
Material and methods
The PURE study is a large prospective cohort study with the main objective of investigating the association between societal influences on human lifestyle, cardiovascular risk factors, and the rate of noncommunicable diseases [7]. PURE MIND (a sub-study of the PURE study) was designed to determine the risk factors and consequences of silent cerebrovascular disease detected on brain magnetic resonance imaging (MRI). Participants were interviewed using a standardised questionnaire, completed medical examination, and the STOP-BANG questionnaire, and they underwent brain MRI. Data included biometrics, cardiovascular disease risk factors, health history, use of medications, and body composition analysis. Ethical approval was acquired from the Local Ethical Committee. All participants signed an informed consent form.
Study population
Two hundred and seven subjects with no history of cerebrovascular disease were included in the study. They were participants of PURE MIND sub-study, who filled in the STOP-BANG questionnaire. A total of 176 patients (133 women and 43 men) scored 0–2 and were categorised as the control group. The remaining group of 31 who scored > 3 (11 women and 20 men) underwent full-night polysomnography and were diagnosed with OSA using the AASM Manual for the Scoring of Sleep and Associated Events, version 2.5. All patients had brain MRI. Body composition analysis was performed using a BC-554 IRONMAN® Body Composition Monitor (Tanita). The demographic characteristics of the study population are presented in Table I. Hypertension was defined as systolic blood pressure over 140 mm Hg or diastolic blood pressure over 90 mm Hg measured at the time of visit as well as treatment with antihypertensive drugs. Diabetes was defined either as treatment with antidiabetic drugs or fasting glucose over 7 mmol/l (126 mg/dl) (measured twice) or glucose over > 11.1 mmol/l (140 mg/dl) 2 h in oral glucose tolerance test. Hyperlipidaemia was diagnosed if serum total cholesterol level was over 12.2 mmol/l (220 mg/dl) or if the patient was undergoing treatment with antihyperlipidemic medications.
Table I
Characteristics of the studied population
Sleep apnoea evaluation
The STOP-BANG questionnaire was used as a screening tool for OSA. It includes eight dichotomous (yes/no) questions related to the clinical features of sleep apnoea (Snoring, Tiredness, Observed apnoea, high blood Pressure, BMI, Age, Neck circumference, and male Gender). The total score ranges from 0 to 8. Patients can be classified for their OSA risk based on their respective scores. It has been evaluated as a three-category variable (low risk (0–2), medium risk (3–4), high risk (5–8)) and validated in pre-operative and general populations [8–10]. The available data demonstrate that a STOP-Bang score < 2 excludes moderate and severe OSA with a probability of 95%; therefore, this was used in our study [11, 12]. The low OSA risk group was considered as control group. Other participants underwent full in-lab diagnostic night polysomnography (Embletta® MPR Sleep System with RemLogic software). All polysomnography studies were scored by a physician blinded to the results of MRI. Apnoea was defined as a cessation of airflow for at least 10 s. Hypopnoea was defined as an amplitude reduction of airflow that was associated with an oxygen desaturation of > 3% or an arousal. Obstructive sleep apnoea was defined by AHI > 5/h. Patients with AHI 5–15/h were diagnosed with mild OSA, AHI 15–30/h – moderate OSA, and AHI > 15/h – severe OSA.
Brain magnetic resonance imaging evaluation
All patients underwent MR of the brain. The data were acquired using a 1.5 T MR (GE) scanner and 16-channel HNS coil. Imaging protocol consisted of T1, T2, FLAIR, and SWI images. The presence of ischaemic stroke, changes in white matter with high signal on T2-weighted and FLAIR images (WMHs – white matter hyperintensities), and micro- or macrobleeds were assessed by trained radiologists. Because no stroke was found and the amount of micro- and macrobleeds was statistically insignificant, only WMHs were taken for further analysis. The severity of WHMs in periventricular and subcortical areas was evaluated using the Fazekas scale [13]. This scoring system includes four grades depending on the size and confluence of lesions: grade 0 – absent, grade 1 – punctate, grade 2 – early confluent, grade 3 – confluent.
Statistical analysis
All statistical analyses were performed using R for windows statistical software (version 3.6.1). The results were expressed as the mean ± standard deviation. Mann-Whitney test and Kruskal-Wallis test were used to compare continuous variables when appropriate. Fisher exact test was performed for qualitative variables. Correlation between continuous variables was assessed using Spearman correlation coefficient. A p-value less than 0.05 was considered statistically significant.
Results
Among 31 OSA subjects 13 (4 women and 9 men) had severe OSA, 9 (4 women and 5 men) were diagnosed with moderate OSA, and the other 9 (3 women and 6 men) had mild OSA. Mean AHI in female and male groups was similar (32.26 ±25.78 vs. 32.70 ±24.50, p = 0.9). Results of PSG are listed in Table II. Magnetic resonance imaging showed WMHs in periventricular area in 10 (32.25%) subjects in the OSA group and 19 (10.79%) subjects in the control group, and the difference was statistically significant (p = 0.00382). The prevalence of subcortical lesions was also higher in OSA patients (n = 13; 41.94%) than in the control group (n = 29; 16.48%; p = 0.00580) No major ischaemic strokes, lacunar strokes, or microbleeds were revealed. In univariate analyses we used the prevalence of WMHs as a dependent variable and assessed the impact of the following independent variables: age, gender, BMI, WHR, smoking, hypertension, hyperglycaemia, hyperlipidaemia, use of aspirin, body muscle mass, body water, and body fat. Among these independent variables only age (p = 0.002 or p = 0.01) was a predictor of the prevalence of periventricular WMHs in patients with OSA and control subjects. For subcortical WMHs age (both in the OSA and control group; p = 0.0002 or p = 0.04) and WHR (only in OSA group p = 0.03) were significant predictors. On the other hand, we used AHI as a dependent variable in the OSA group and evaluated the impact of the same independent variables and WMHs, but no significant predictor was identified in this group.
Table II
Polysomnography results
Discussion
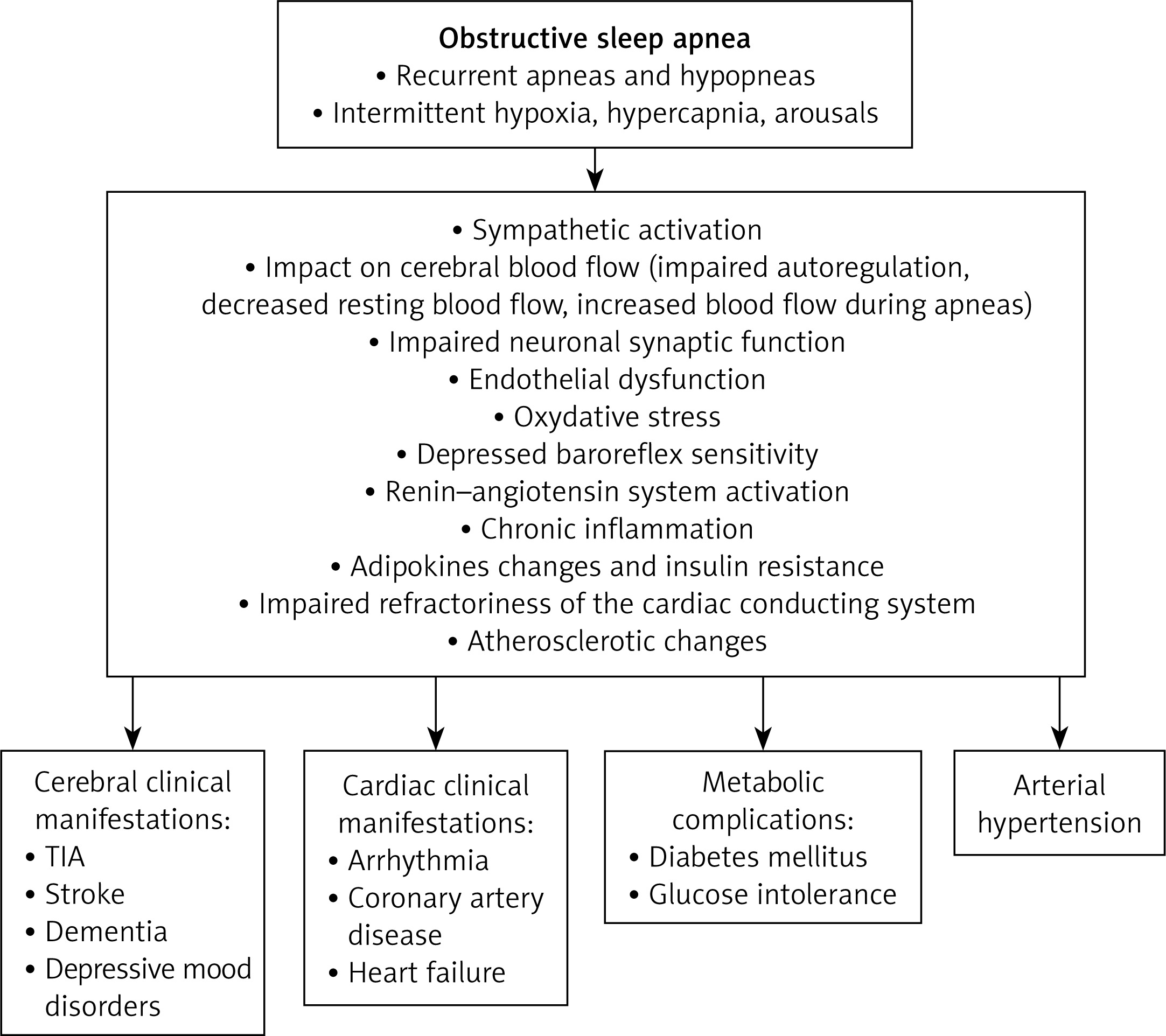
Aging and neurodegenerative disorders are a growing problem. White matter hyperintensities along with perivascular space widening, brain atrophy, and lacunar infarctions are neuroradiological manifestations of CVSD and are histopathologically correlated with axonal loss, focal myelinolysis, reactive astrocytosis, and vessel wall hyalinosis. Clinical implications include increased risk of stroke, cognitive dysfunction, dementia, gait instability, and depression [14, 15]. Typically, changes increase with the aging process; however, their onset and progression can be exacerbated by comorbidities. The prevalence of CSVD in neuroimaging studies ranges from 5% to 62% [16], depending on the studied population and research methodology. In most papers this incidence was estimated at 10–20%. Higher values are observed in patients with previous stroke or transient ischaemic attack (TIA). The strongest factor influencing the occurrence is age, with an annual incidence of between 2% and 4%. In the Rotterdam Scan Study, the prevalence of silent brain infarcts increased from 8% in subjects 60 to 64 years old, 13% in 65 to 69 years old, to more than 20% in the 70 to 79-year-olds and 35% in those older than 80 years [17]. As well as age, other significant risk factors that have a strong association with CSVD are hypertension, hyperlipidaemia, smoking, male sex, and intra- and extracranial large artery atherosclerotic disease [18–20]. The effects of other recognised cardiovascular factors such as diabetes mellitus, tobacco use, alcohol consumption, obesity, or atrial fibrillation, although possibly important, have not been clearly demonstrated. One of the suggested factors contributing to the onset and severity of CSVD is OSA. Pathophysiological changes that occur during periods of apnoea and hypopnoea affect the vascular endothelium and flow in the cerebral vessels both at night and during wakefulness [21]. Oxidative stress, inflammatory response, activation of the sympathetic nervous system, and disturbed blood flow autoregulation interfere with normal blood flow in the cerebral macro- and microvessels. Numerous studies have demonstrated that patients with moderate and severe OSA have a higher prevalence of CSVD than controls or subjects with mild OSA [22–26]. A recently published meta-analysis and systematic reviews confirm that moderate to severe sleep apnoea is independently related to WMH and silent brain infarcts, which strongly suggests that OSA may contribute to the pathogenesis of CSVD [27, 28]. In the present study the score of WMHs both in periventricular and subcortical areas was significantly higher in patients with OSA than in the control group. Our analysis indicated age as the strongest risk factor for WMHs, consistent with previous findings. Major strengths of our study include the population representative group [29], recruitment strategies to mitigate bias, and no previous studies on the population in this region. There are, however, some limitations of our study: the small sample size, the lack of exclusion of OSA on the basis of polysomnography, age differences, and gender asymmetry favouring men in the OSA group and women in the control group, which limits the external validity of the results. In future research the comparison with a control group of similar age, sex, and comorbidities could determine the relationship between OSA and CSVD more clearly. Some data suggest that effective hypertension control can prevent or halt WMH progression [30–32]. Although it remains unproven whether continuous positive pressure treatment (CPAP) also has such an effect, some reports indicate that CPAP may positively alter brain microstructure and perfusion patterns [33]. The study of Castronovo et al. showed that the structural brain abnormalities observed in white matter regions susceptible to hypoxemia can improve with CPAP treatment in three months. The effect was more pronounced after 12 months of positive pressure treatment [34]. In another study assessing not only resonance image but also cognitive function tests, significant improvement in the verbal episodic memory test was seen after just 1 month of using CPAP [35]. Further investigations evaluating the long-term effect of OSA treatment on brain microarchitecture on large groups of patients are needed.
In conclusion, the significantly higher incidence of WMHs in the OSA group suggests that patients with OSA may be at increased risk of neurodegenerative complications (Figure 1).