
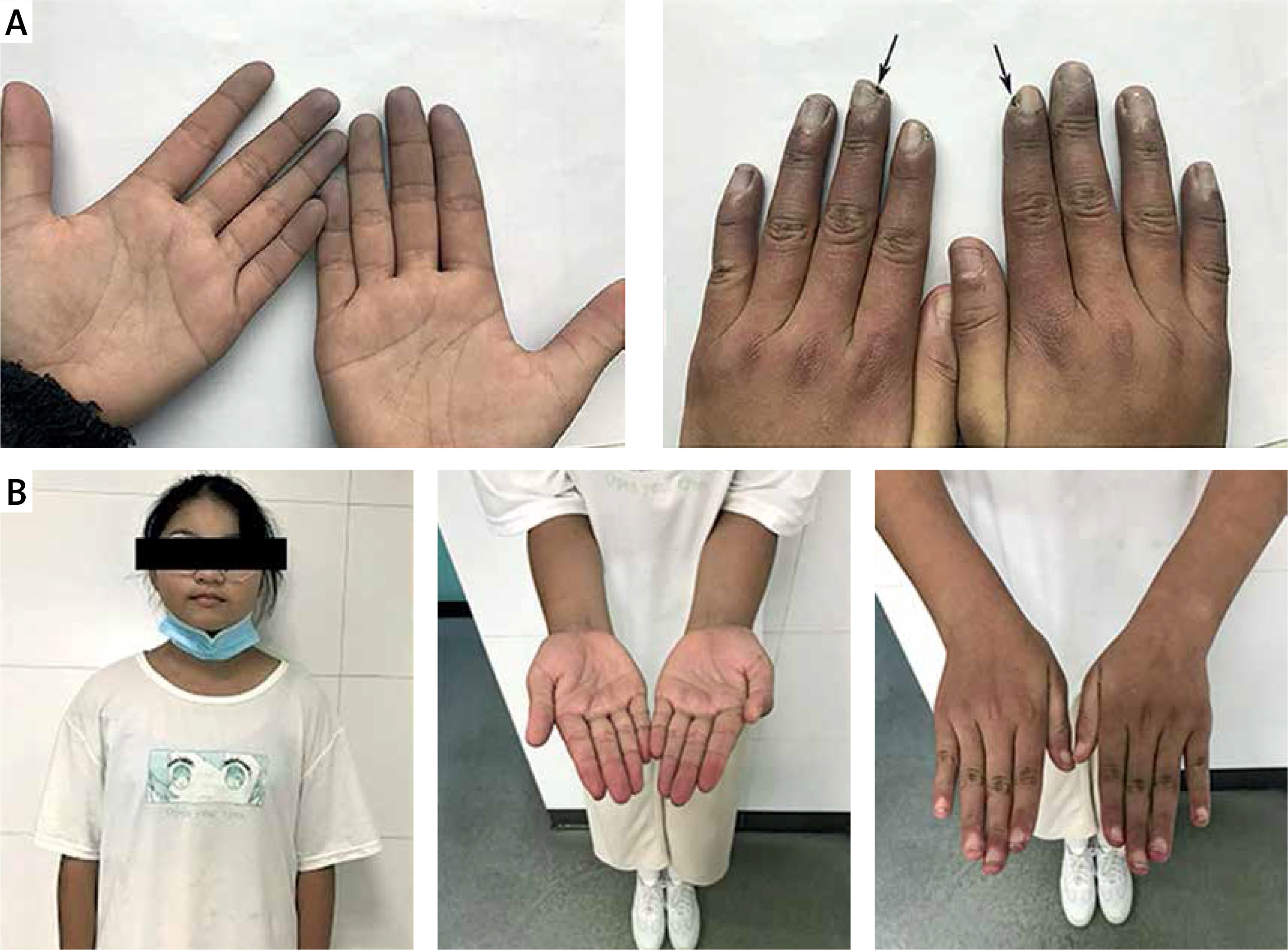
A 12-year-old girl presented to our paediatric department due to a 6-week history of Raynaud’s phenomenon (RP) with cold, swollen, and cyanotic fingers. She also complained pains and ulcers (arrows) in her fingers with morning stiffness of around 3 h (Figure 1 A). On physical examination, we found her blood pressure was 117/69 mm Hg, heart rate was 94 beats per minute, axillary temperature was 38.6°C, respiratory rate was 25 breaths per minute, and she had multiple enlarged bilateral cervical lymph nodes with a diameter of almost 4 cm. Laboratory studies found a normocytic anaemia (haemoglobin 104 g/l), with a normal red blood cell count of 4.16 × 1012/l, a white blood cell count of 8.67 × 109/l, and a platelet count of 394 × 109/l. Other chemistries showed elevated levels of alanine aminotransferase (59 U/l), aspartate aminotransferase (65 U/l), creatine kinase (415 U/l), and creatine kinase isoenzyme (374 U/l). The autoimmune and serologic workup came back positive for ANA at a titre of 1 : 3200, anti-U1-snRNP at a titre of 1 : 1600, HLA-B27 (77%), anti-Sm, and low complement C4 (0.07 g/l). Cardiac ultrasonography showed pulmonary hypertension with a pulmonary arterial pressure of 29 mm Hg. According to 2019 European League Against Rheumatism (EULAR)/American College of Rheumatology (ACR) criteria, our patient was diagnosed as having systemic lupus erythematosus (SLE) with a definitive score of 17, including fever (2 points), joint involvement (6 points), low C4 (3 points), and positive for anti-Sm (6 points). In addition, the SLEDAI-2K score was 7 points at the first visit. Treatments with prednisolone, naproxen, hydroxychloroquine, methotrexate, and nifedipine were initiated. Her fever, morning stiffness of fingers, and liver dysfunction resolved completely within 1 week. At a follow-up visit 4 months after discharge, RP significantly resolved, her finger ulcers had completely healed (Figure 1 B), and C4 had increased to 0.15 g/l.
Figure 1
A – Raynaud’s phenomenon. Arrows represent the ulceration of fingers. B – At a follow-up visit 4 months after discharge, Raynaud’s phenomenon had significantly resolved, and her finger ulcers had completely healed
The 2019 EULAR/ACR classification criteria for SLE include positive ANA at least once as an obligatory entry criterion, followed by additive weighted criteria grouped in 7 clinical and 3 immunological domains and weighted from 2 to 10. Patients accumulating ≥ 10 points are classified [1]. In this report, our patient had a EULAR/ACR total score of 17; thus, the diagnosis of SLE could be established. In addition, the SLE Disease Activity Index 2000 (SLEDAI 2K) score was 7 at the first visit, including arthritis (4 points), low complement (2 points), and fever (1 point). According to the 2019 update of the EULAR recommendations for the management of SLE, our patient had moderate disease activity [2].
RP is a nonspecific cutaneous lesion that appears in 10% of paediatrics with SLE initially [3]. The presence of RP would suggest a less severe disease. Glomerulonephritis, serositis, and haemolytic anaemia occurred in 35.5%, 14.2%, and 4.5% of SLE patients with RP, respectively. In addition, the presence of anti-U1-RNP antibodies in patients fulfilling SLE criteria (but not the mixed connective tissue disease, MCTD) is found to be associated with manifestations such as RP, musculoskeletal, lung impairment, or nail fold capillaroscopy changes, which are frequently encountered in MCTD patients but rarely described in the lupus population [4]. Apart from the basic treatment for SLE, calcium channel blockers are currently the most prescribed and studied medications for Raynaud’s attacks, with a mean reduction of 35% in the severity of RP attacks over 2 weeks [5]. In this situation, we speculate that the long-term outcomes of our patient are prone to be relatively satisfactory.