Introduction
Today, as the degree of trust between doctors and patients continues to decline, the tense doctor-patient relationship (DPR) is becoming an industry-wide problem. In 2018, the China Medical Association survey showed that there were 90,000 medical disputes in China in 2016, in which over 50% of medical staff were subjected to verbal violence and 15% of the medical staff suffered physically injury [1]. As an industry in frequent contact with sick patients, doctors require a strong sense of responsibility and cognitive and emotional abilities [2]. Under the influence of a tense DPR, doctors are prone to develop a sense of identity and alertness, increase psychological pressure and subjectively create poor cognition of DPR tensity. Moreover, doctors have to face heavy workloads, such as night shifts, surgery, writing medical records and so on. Various pressures cause doctors to be prone to occupational burnout [2, 3–6].
Conversely, doctors with occupational burnout are prone to poor communication and more frictions with patients due to the decline of their enthusiasm for work, emotional control and communication expectations, which may further aggravate doctors’ poor cognition of DPR tensity [7]. Such a vicious circle will inevitably bring about enormous social problems and intensify the conflict between doctors and patients.
So we consider that there may be a causal relationship between the degree of occupational burnout and cognition of DPR tensity in doctors. However, it is unsubstantiated, because there is no study on the correlation between them at present. Therefore, this study quantifies the degree of doctors’ occupational burnout in a general hospital, evaluates respectively the cognitions of DPR tensity in doctors and patients, analyzes their correlations and proposes some targeted intervention measures.
Material and methods
Study population
300 clinical doctors were selected randomly as study objects from a general hospital in China. We issued 300 questionnaires and got back 281 copies of them, among which there were 265 valid copies. The effective rate was 94.3%. The baseline information of doctors included age, sex, educational background and professional title. The inpatients for whom the above-mentioned doctors were responsible (3 per doctor) were randomly selected as patient survey objects. A total of 795 questionnaires were handed in person to patients by our researchers, and recovered by us on site after patients completed the questionnaires. 782 were recovered and valid. The effective rate was 100%. Studies were performed with the understanding and consent of each subject including doctors and patients, with the approval of the Ethics Committee of Zhengzhou University. Each subject signed informed consent.
Quantitative evaluation for the degree of occupational burnout
The questionnaire of the Maslach Burnout Inventory-General Survey (MBI-GS) [8] was applied to evaluate the degree of occupational burnout in doctors including three aspects of emotional exhaustion, depersonalization and sense of personal achievement. The burnout scoring criteria of three aspects are as follows: the scores of mild burnout are less than 9, less than 3 and more than 18 points, scores of moderate burnout are 9–13, 3–9 and 18–30, and scores of high burnout are more than 13, more than 9 and less than 18 points, respectively. The Cronbach’s α coefficient values of three aspects were respectively 0.87, 0.81 and 0.82, which were of high reliability.
Quantitative evaluation for the tensity of doctor–patient relationship
The Difficult Doctor-Patient Relationship Questionnaire-10 (DDPRQ-10) [9, 10] is widely used to quantitatively evaluate the cognitive situation of DPR tensity in doctors. The Patient-Doctor Relationship Questionnaire-15 (PDRQ-15) was developed by Van der Feliz-Cornelis et al. in 2004 for evaluating the patients’ cognition of DPR tensity [11]. It has been developed into a multinational version for evaluation and application [11–14]. Yang et al. revised them to form a Chinese-specific DDPRQ-8 and PDRQ-13, which had good reliability and validity [15, 16]. The contents and scoring methods of DDPRQ-8 and PDRQ-13 are shown in Tables I and II, respectively. The higher the score was, the greater was the difficulty doctors or patients faced in the DPR and the more serious the DPR tensity was. 50% of theoretical maximum scores of DDPRQ-8 and PDRQ-13 are 24 and 32.5 points respectively. Scores higher than or equal to 24 or 32.5 points suggest that doctors or patients have poor cognition of DPR tensity, and lower scores suggest good cognition.
Table I
Difficult Doctor–Patient Relationship Questionnaire-8 (DDPRQ-8) for doctors
Table II
Patient–Doctor Relationship Questionnaire-13 (PDRQ-13) for patients
Statistical analysis
All data were analyzed using SPSS 22.0 statistical software. According to age, sex, educational background and professional title, the differences between the occupational burnout scores of each group were compared by the one-way ANOVA (homogeneity of variance assumptions were satisfied) or Kruskal-Wallis test (homogeneity of variance assumptions were not satisfied). The difference of the cognitions of DPR tensity between doctors and patients was compared by the χ2 test. The correlation between the degree of occupational burnout and cognition of DPR tensity in doctors was analyzed by both the Spearmen correlation analysis and the χ2 test. The differences were considered to be statistically significant when the adjusted P-values were < 0.05.
Results
Baseline information of doctors
There were 265 doctors (172 males and 93 females) as respondents in 22 departments including internal, surgery, gynecology and obstetrics, pediatrics, ophthalmology, otorhinolaryngology, and emergency. The average age was 39.6 ±8.76 (40.7 ±8.21 in males, 37.5 ±9.38 in females) years. The specific baseline information of age, sex, educational background and professional title is shown in Table III.
Table III
Scores of doctors’ occupational burnout degree under the baseline information
| Baseline information | n (%) | Scores ( | ||
|---|---|---|---|---|
| Emotional Exhaustion | Depersonalization | Sense of personal achievement | ||
| Age [years]: | ||||
| ≤ 30 | 47 (17.7) | 10.79 ±8.93 | 5.28 ±6.73 | 25.15 ±8.26a |
| 31-40 | 104 (39.2) | 11.98 ±8.62 | 6.27 ±6.35 | 28.09 ±8.06 |
| 41-50 | 74 (27.9) | 9.84 ±8.88 | 4.39 ±5.17 | 30.53 ±7.27 |
| ≥ 51 | 40 (15.1) | 8.08 ±7.73 | 3.90 ±6.42 | 29.35 ±8.91 |
| Gender: | ||||
| Male | 172 (64.9) | 10.34 ±8.73 | 5.15 ±6.23 | 28.62 ±8.38 |
| Female | 93 (35.1) | 11.03 ±8.63 | 5.32 ±6.07 | 28.10 ±7.84 |
| Educational background: | ||||
| Bachelor | 51 (19.2) | 10.00 ±9.25 | 5.43 ±7.03 | 27.20 ±9.03 |
| Master | 139 (52.5) | 11.40 ±9.08 | 5.40 ±6.21 | 28.68 ±7.92 |
| PhD/MD | 75 (28.3) | 9.45 ±7.39 | 4.71 ±5.47 | 28.83 ±8.08 |
| Professional title: | ||||
| Resident physician | 20 (7.5) | 8.90 ±8.53 | 3.30 ±4.44 | 25.15 ±8.32c |
| Attending physician | 111 (41.9) | 12.08 ±9.12b | 6.19 ±6.54 | 27.29 ±8.30c |
| Associate Chief Physician | 61 (23.0) | 10.97 ±8.63 | 5.56 ±6.63 | 29.16 ±7.43 |
| Chief Physician | 73 (27.5) | 8.44 ±7.68 | 3.96 ±5.29 | 30.48 ±8.13 |
The degree proportions of occupational burnout in doctors
The degree proportions of occupational burnout in doctors on three dimensions (emotional exhaustion, depersonalization and sense of personal achievement) are shown in Table IV. The proportions of doctors with moderate and severe burnout in three dimensions were 50.9%, 53.2% and 48.7% respectively, which all reached about half.
Degrees of occupational burnout under the baseline information of doctors
According to ages, the score of sense of personal achievement was lowest in doctors under 30 years old, and highest in doctors aged 41 to 50; the differences were statistically significant (p = 0.003). There were no significant differences in the scores of emotional exhaustion and depersonalization (p > 0.05). According to professional titles, the score of emotional exhaustion in attending physicians was higher than that in chief physicians (p = 0.024). The scores of sense of personal achievement in resident and attending physicians were lower than those in chief physicians (p = 0.009). There were no significant differences in the scores of depersonalization (p > 0.05). According to sex and educational background, there were no statistically significant differences in the three dimensions of occupational burnout (p > 0.05) (Table III).
Comparisons of both doctors and patients’ cognitions of doctor–patient relationship tensity
Doctors generally held a negative attitude towards DPR. The average scores of doctors’ cognitions of DPR tensity were close to 24 points in almost all departments, and more than 24 points in 40.91% of departments. The top three departments with poor cognitions of DPR tensity were respiratory, emergency and gastrointestinal surgery departments. The patients’ cognition of DPR tensity was more optimistic than that of doctors. The cognitive scores in patients in all departments were obviously lower than 32.5 points. They thought that DPR was good, and the overall trend of cognitions was stable (Table V). χ2 analysis showed that there are statistically significant differences in the cognitive scores of DPR tensity between doctors and patients (χ2 = 290.178, p < 0.0001) (Table VI).
Table V
Cognitive scores of doctor–patient relationship tensity in doctors and patients in clinical departments
Correlation between degrees of occupational burnout and cognition of doctor–patient relationship tensity in doctors
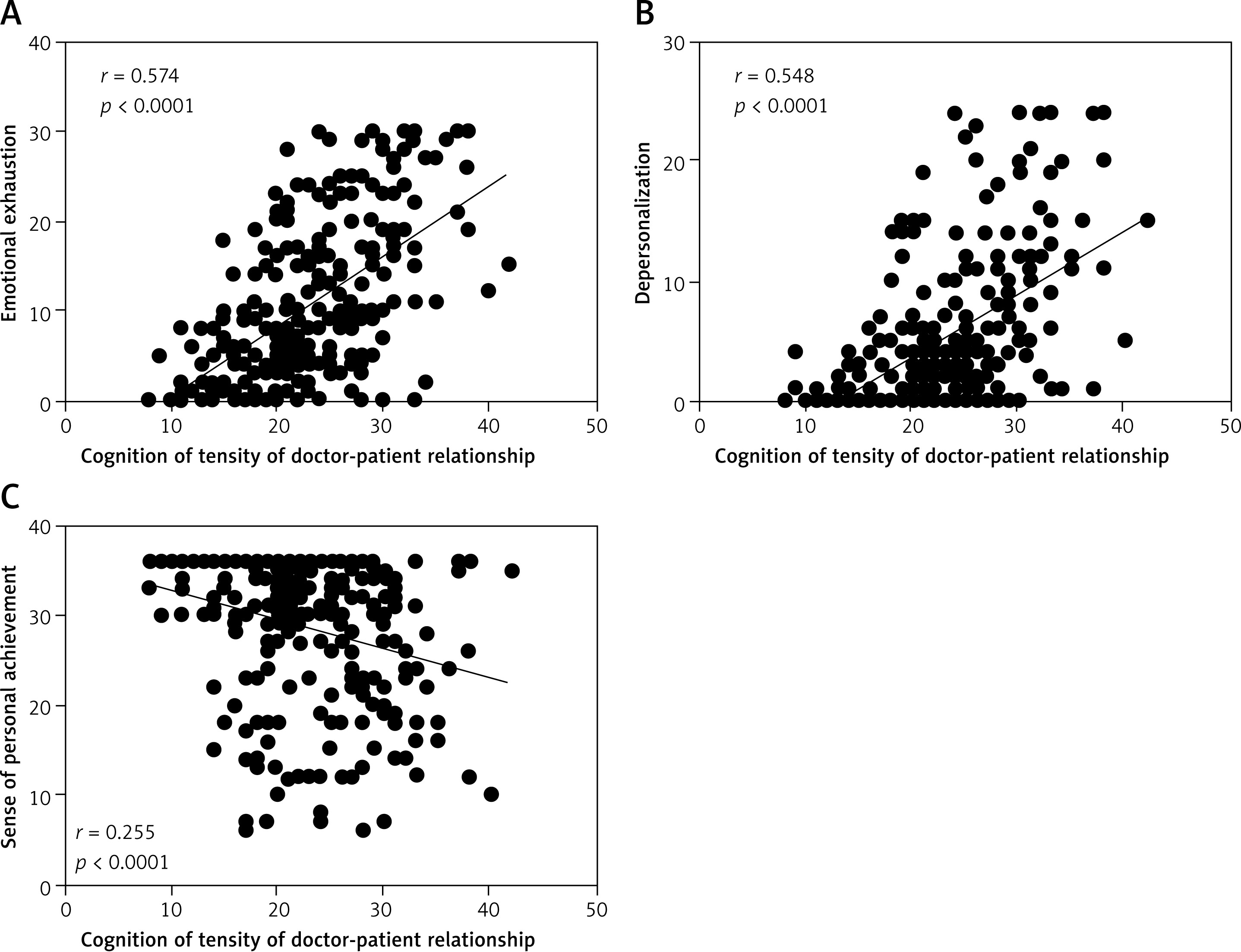
Spearman correlation analysis results suggested that emotional exhaustion and depersonalization were positively correlated with poor cognition (r = 0.574, p < 0.0001; r = 0.548, p < 0.0001) (Figures 1 A, B), while the sense of personal achievement was negatively correlated with that (r = –0.255, p < 0.0001) (Figure 1 C).
Figure 1
Correlation between three dimensions of occupational burnout and cognition of tensity of doctor–patient relationship (DPR) in doctors. A – Emotional exhaustion was positively correlated with poor cognition of DPR tensity (r = 0.574, p < 0.0001). B – Depersonalization was positively correlated with poor cognition of DPR tensity (r = 0.548, p < 0.0001). C – Sense of personal achievement was negatively correlated with poor cognition of DPR tensity (r = –0.255, p < 0.0001)
Doctors with low occupational burnout had good cognition of DPR tensity, with 77.4%, 79.2% and 65.4% of doctors having good cognition of depersonalization, emotional exhaustion and personal accomplishment respectively. Doctors with high occupational burnout generally have poor cognition of DPR tensity, with 80.7%, 70.7% and 58.8% of doctors having poor perception of three dimensions respectively. χ2 test results indicated that doctors’ cognition of DPR tensity had statistical significance under different degrees of occupational burnout (p < 0.01) (Table VII).
Table VII
Degree proportions of cognitions of doctor–patient relationship tensity in doctors with occupational burnout (n (%))
Discussion
Occupational burnout was first proposed by the American psychiatrist Freudenberger in 1974, and refers to a state of extreme exhaustion caused by excessive demand for energy and all the resources which an individual possesses [17]. As the pressure of social competition increases, the phenomenon of occupational burnout becomes more and more common and can affect a wide range of professions, but people who are engaged in work that helps others are particularly vulnerable to this effect [18]. It could not be ignored that a high degree of occupational burnout exists in medical staff [8, 19–21].
Burnout is a syndrome of emotional exhaustion, depersonalization and reduced personal achievement that can occur among individuals who do “people work of some kind” [22]. Our study revealed that in a general hospital, about half of the doctors have moderate or severe burnout in each of the three dimensions of emotional exhaustion, depersonalization and sense of personal achievement. More than a third of doctors had severe emotional exhaustion.
The degree of emotional exhaustion was most severe in attending physicians, which was not noted in previous studies [23]. The reasons may be as follows: attending physicians are responsible for the main clinical work in the department, as well as the heavy research and teaching tasks; their labor intensity is great while the work position is relatively low; they also face various pressures from superior physicians, patients, promotion and career development.
However, the occupational burnout of resident physicians was mainly reflected in the low sense of personal achievement, which is similar to the previous findings [24–26]. The reasons may be related to the junior stage of work, lack of medical experience, deficiency of professional skills, difficulties and setbacks in work and distrust of patients.
The cognitive situations of DPR tensity in doctors and patients were also evaluated. The doctors generally had a negative attitude towards DPR tensity, and thought that DPR was poor. In contrast, patients’ attitude toward DPR was obviously optimistic. Patients generally believed that DPR was good, and there was a deviation from doctors’ poor cognition, which was consistent with a previous study [27]. The difference in the cognitions of DPR tensity between doctors and patients, which creates obstacles for smooth communication and mutual understanding, may lead to tense DPR and conflict between doctors and patients [28].
Doctors’ poor cognition of DPR tensity might have an effect on their psychological condition, and bring antipathy towards patients, hospitals, departments and daily work. This could aggravate the sense of occupational burnout for doctors. Conversely, the high ratio and degree of occupational burnout may seriously endanger the quality of life, work enthusiasm and physical and mental health of doctors [29], which would lead to inefficiency in diagnosis and treatment, decline in service quality [7, 30–32], increase in risk of mistakes and difficulties in communication between patients and doctors. These may strain DPR and proliferate the medical conflicts [33].
However, it is not clear whether there is a correlation between the degree of occupational burnout and cognition of DPR tensity in doctors. Few related studies have been published. Some studies suggested that the rise in the sense of occupational burnout in doctors would cause tense DPR based on a lack of quantitative evaluation [34, 35]. Our study quantified the cognitive situation of DPR tensity in doctors by DDPRQ-8, and conducted a correlation analysis with the degree of occupational burnout. It was found that the degree of occupational burnout in doctors was significantly correlated with the cognition of DPR tensity. In three dimensions of emotional exhaustion, depersonalization and personal accomplishment, more than 60% of doctors with less burnout had good cognition of DPR. With the increase of burnout degree, doctors’ cognition of DPR tensity tended to deteriorate.
This suggests that the level of doctors’ occupational burnout and their cognition of DPR tensity interact. Further research will be carried out to ascertain whether improving the status quo of one of them might promote the improvement of the other’s status.
Accordingly, the following measures are recommended. First, improve doctors’ awareness of occupational burnout, popularize self-assessment and determination of their degrees of occupational burnout in time. Second, psychological counseling and means of relief should be provided for doctors with occupational burnout as soon as possible, and the hospital should give humane care and take measures for pressure reduction to control the production and aggravation of occupational burnout in doctors. Third, doctors should know the cognitive difference between doctors and patients in DPR tensity, patients’ cognition usually being more optimistic than that of doctors, so as to provide preconditions and guarantee for cognitive convergence on DPR tensity in order to reconstruct a harmonious DPR. The above measures can reduce the degree of occupational burnout in doctors, which might change the doctors’ poor cognition of DPR tensity into good cognition. This could reduce the iatrogenic risk of tense DPR, and promote the improvement of DPR.
In conclusion, doctors play a vital role in maintaining a normal DPR. The degree of doctors’ occupational burnout is at a high level and correlated with the poor cognition of DPR tensity in China. Hospitals and society should pay attention to the status quo of doctors’ occupational burnout and take measures to improve it. It is possible to improve the DPR by reducing the degree of doctors’ occupational burnout. This will provide a new way for the formation and maintenance of a good DPR.