Introduction
Clinical inertia is a common problem with asymptomatic chronic disease management [1] and is defined as the failure to achieve appropriate targets because of delayed time to achieve treatment intensification [2–4]. Three processes define clinical inertia in an operational sense. First, the clinical target must be selected. Second, the disease treatment must be defined and must be measurable. Finally, the time to evaluate treatment intensification must be determined [1, 5]. Therefore, assessing clinical inertia in each chronic disease study differs. Type 2 diabetes mellitus (T2DM) is a major health problem worldwide [6], and drug therapies are not optimal [7]. Universal standard measurement to quantify clinical inertia is still lacking [8]. One study in the US revealed that 72.8% of patients with T2DM experienced clinical inertia [9]. In Thailand, Ostaphan et al. found that 68.4% of patients with T2DM had experienced clinical inertia [10]. Furthermore, Pholdee et al. reported that 5903 (38.8%) patients had clinical inertia [11]. Clinical inertia can lead to cardiovascular complications and progress to diabetic retinopathy [10, 12]. Research focusing on clinical inertia in T2DM is well documented in developed countries [13, 14]. However, corresponding data are needed in developing countries [14].
A study by Osataphan et al. defined clinical inertia as a state in which patients with T2DM presenting an glycated haemoglobin (HbA1c) level ≥ 9% did not receive treatment intensification with insulin initiation within three months [10]. This study evaluated clinical inertia based on injectable insulin only and also considered the results within a certain timeframe. A study by Pholdee et al. selected newly diagnosed T2DM patients [11] while clinical inertia can occur throughout [15]. Our study examined clinical inertia using new criteria: using both injectable and oral antidiabetic drugs (OADs) instead of a sole injectable or OADs alone, and evaluating clinical inertia at the index date or in a subsequent prescription written within the study time limits. In an attempt to describe the extent and factors associated with clinical inertia, this study examined the patterns of patients with T2DM treatment in a tertiary care hospital in Thailand.
Material and methods
Study design
An observational study was undertaken on patients with T2DM using existing data obtained from medical records and the electronic hospital database of the Maharaj Nakorn Chiang Mai Hospital in northern Thailand.
The study was approved by the Ethics Committee Board at the Faculty of Medicine, Chiang Mai University, Thailand.
Database
The Maharaj Nakorn Chiang Mai Hospital is a university hospital affiliated with Chiang Mai University. This large tertiary care public hospital contains 1400 beds serving the needs of residents of Chiang Mai, Thailand (an approximate population of 1,800,000), as well as patients referred from hospitals from nearby provinces in northern Thailand. It services an average of 1,300,000 outpatients and 46,000 inpatients yearly. All patient data were obtained from an electronic medical database (EMD). Data were entered in the EMD at the study hospital by trained nurses. The EMD comprised patient demographics, medications prescribed at any outpatient visits, laboratory data, follow-up appointment, and types of prescribers classified as general practitioners, residents, or specialists [16]. Then, all data were reviewed and recorded on a case record form (CRF) for data analysis.
Study patients
All T2DM patients attending the outpatient clinic at Maharaj Nakorn Chiang Mai Hospital between 1 January 2017 and 31 December 2017 were included. If patients were not followed up in this centre, be it at another centre or not at all, we excluded those patients from the study. Patients are advised to test for HbA1c once a year. In general, the doctor makes the appointment every three months unless the patient has high blood sugar at the time of the appointment. If they do, the next appointment can be earlier. Inclusion criteria: (1) a previous diagnosis of T2DM aged 40 to 65 years, (2) presenting an HbA1c level ≥ 7.00% and (3) receiving at least 1 OAD. Exclusion criteria: (1) having a history of symptomatic hypoglycaemia, (2) pregnancy and lactation, (3) end-of-life care, (4) using insulin only, (5) multiple comorbidities, and (6) history of poor lifestyle modifications or adherence.
The comorbidity was evaluated using the Charlson Comorbidity Index (CCI). The CCI predicts the 10-year survival of a patient who may have a range of comorbid conditions. Each condition is assigned a score of 1, 2, 3, or 6 depending on the level of risk [17]. If participants had a CCI score of at least 3, they were classified as multiple comorbidities. Poor lifestyle modifications or adherence was identified when a patient was recorded on the medical card by the health care provider as having poor lifestyle modifications or nonadherence to treatment or missing their appointment.
Definition of terms
The index date was defined as the date of the first HbA1c laboratory test above the target level (HbA1c ≥ 7.00%) during the study period from 1 January to 31 December 2017.
Clinical inertia was identified when an HbA1c level was found at ≥ 7.00%, at the index date, followed by no treatment intensification from the index date and the subsequent prescription.
No clinical inertia was identified using two methods. First, patients had an HbA1c level ≥ 7.00% at the index date and received treatment intensification at the index date or at a subsequent prescription. Second, patients did not receive treatment intensification at the index but at the next follow-up time, and they had a blood sugar test within the target level.
Treatment intensification was defined either as the addition of a new antidiabetic drug, a change from an OAD to an injectable antidiabetic drug, or an increase in dose of an existing antidiabetic drug, without discontinuing or reducing the dose of other antidiabetic drugs.
Statistical analysis
Data were analysed using STATA® Version 14. Descriptive statistics were used to summarise patient demographics. We considered a nonlinear model of success of clinical inertia. The dependent variable (clinical inertia) is dichotomous and can assume two levels: 0 (“no clinical inertia”) or 1 (“clinical inertia”). We obtained independent variables from the electronic medical record at the index date: age, sex, duration of T2DM, health insurance coverage, history of hypertension, dyslipidaemia, gout, baseline HbA1c, number of antidiabetic drugs used, and use of insulin. The type of doctor was recorded at the occurrence of clinical inertia or at treatment intensification. Health insurance coverage was recorded as Universal Health Care Coverage (UC), Civil Servant Medical Benefit Scheme (CSMBS), Social Health Insurance (SHI), and self-pay. Hypertension, dyslipidaemia, or gout was attributed when patients were given this diagnosis by the treating doctor and/or received drug treatment. The type of doctor was recorded as general practitioner, resident, or specialist. Externs and interns were classified as general practitioners. Fellow and staff were classified as specialists. We selected these factors based on previously published literature and our clinical experience of patients with T2DM. Significantly associated variables (p < 0.200) were entered into a multivariable logistic regression model to predict clinical inertia. Predictors that had a variant inflation factor (VIF) value > 2 were excluded from the multivariable logistic regression. The final model was tested for goodness of fit by Hosmer-Lemeshow test. P-value less than 0.050 was used to determine the statistical significance.
Results
Baseline characteristics
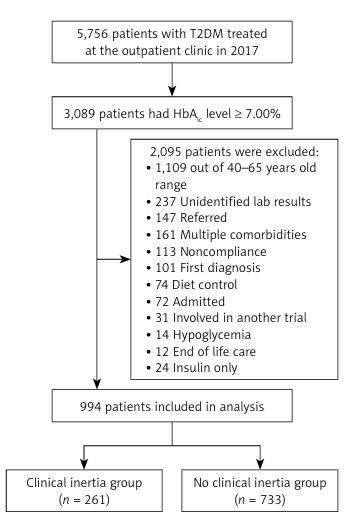
Between 1 January and 31 December 2017 there were a total of 5756 T2DM outpatients. Of these, 3089 patients presenting HbA1c level ≥ 7.00%; 994 patients met the inclusion criteria, and 2095 patients met the exclusion criteria (Figure 1). A total of 994 patients were included in this study. Among all patients, 58.6% were female, the mean age of patients was 55.55 ±6.10 years, median (IQR) duration of diabetes was 5 (2–9) years, and baseline HbA1c was mostly 7.00–7.99%. Most participants were covered by social health insurance. In addition, most patients used two OADs and were treated mainly by specialists (Table I).
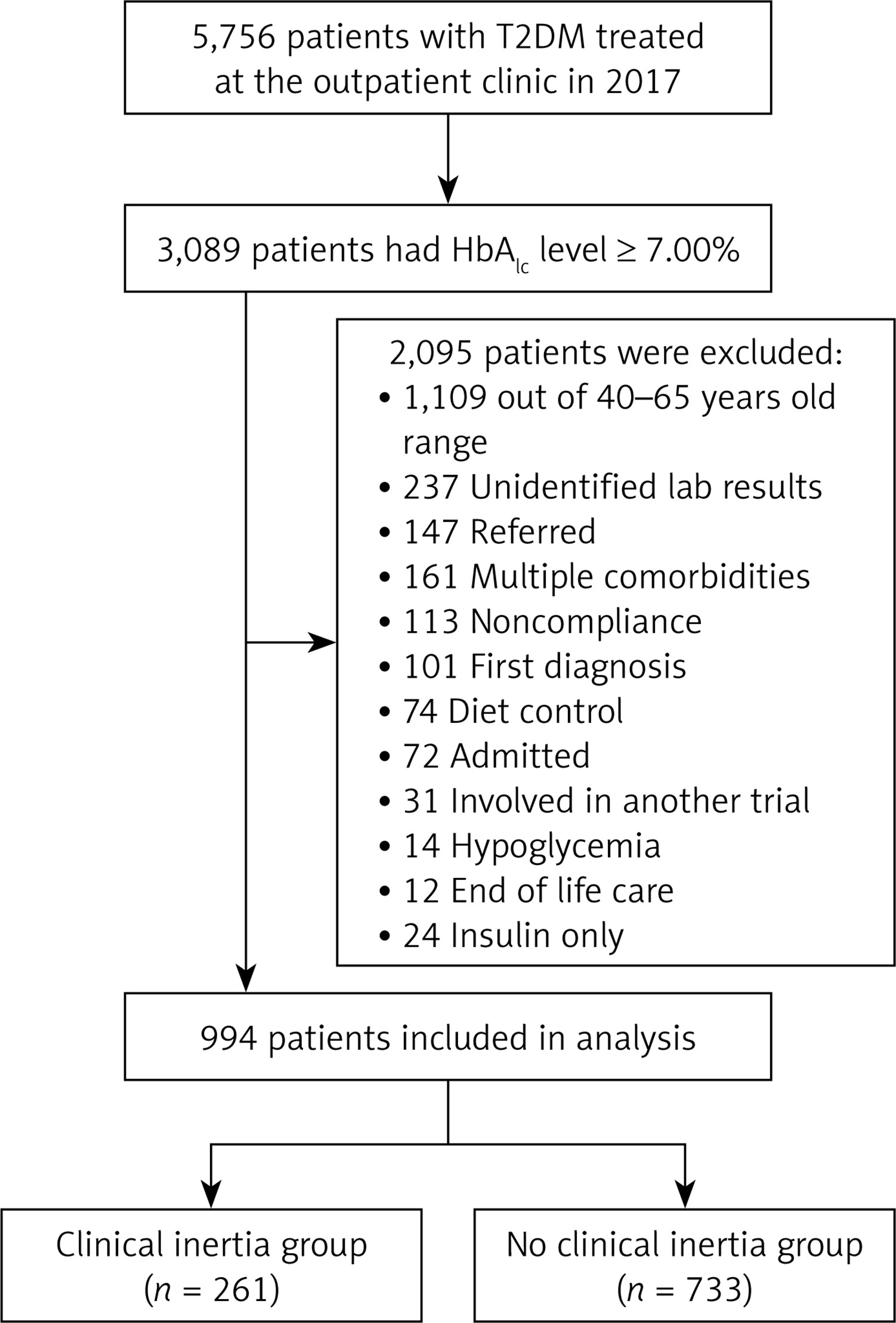
Table I
Baseline characteristics
| Characteristic | All (n = 994) | Clinical inertia (n = 261) | No clinical inertia (n = 733) | P-value* |
|---|---|---|---|---|
| Sex: | ||||
| Female | 583 (58.6) | 145 (55.6) | 438 (59.8) | 0.237 |
| Male | 411 (41.4) | 116 (44.4) | 295 (40.2) | |
| Age [years] | 55.55 ±6.10 | 55.92 ±6.20 | 55.42 ±6.06 | 0.250 |
| Duration of T2DM [years] | 5 (2–9) | 6 (3–9) | 5 (2–9) | 0.341 |
| Health insurance: | ||||
| Self-pay | 37 (3.7) | 7 (2.7) | 30 (4.1) | 0.001 |
| Civil Servant Medical Benefit Scheme | 411 (41.4) | 135 (51.7) | 276 (37.6) | |
| Social Health Insurance | 458 (46.1) | 98 (37.6) | 360 (49.1) | |
| Universal Coverage Scheme | 88 (8.8) | 21 (8.1) | 67 (9.1) | |
| Current drinker | 127 (13.4) | 33 (13.6) | 94 (13.3) | 0.893 |
| Current smoker | 33 (3.5) | 8 (3.3) | 25 (3.5) | 0.863 |
| Hypertension | 726 (73.0) | 199 (76.2) | 527 (71.9) | 0.174 |
| Dyslipidaemia | 690 (69.4) | 195 (74.7) | 495 (67.5) | 0.031 |
| Gout | 25 (2.5) | 10 (3.8) | 15 (2.0) | 0.114 |
| Charlson comorbidity index: | ||||
| 1 | 838 (84.3) | 218 (83.5) | 620 (84.6) | 0.686 |
| 2 | 156 (15.7) | 43 (16.5) | 113 (15.4) | |
| HbA1c at index date: | ||||
| 7.00–7.99% | 494 (49.7) | 149 (57.1) | 345 (47.1) | 0.005 |
| 8.00–8.99% | 276 (27.8) | 70 (26.8) | 206 (28.1) | |
| ≥ 9.00% | 224 (22.5) | 42 (16.1) | 182 (24.8) | |
| Lipid profile: | ||||
| Total cholesterol [mg/dl] | 170.40 ±43.48 | 169.28 ±44.08 | 170.86 ±43.29 | 0.700 |
| Triglyceride [mg/dl] | 136 (96–199) | 152 (103–218) | 129 (95–190) | 0.042 |
| HDL-C [mg/dl] | 51.24 ±22.45 | 48.98 ±12.61 | 52.18 ±25.40 | 0.049 |
| LDL-C [mg/dl] | 96 (78–126) | 93 (80–125) | 97 (78–128) | 0.626 |
| Blood pressure: | ||||
| Systolic [mm Hg] | 132.07 ±14.42 | 133.17 ±14.53 | 131.68 ±14.36 | 0.150 |
| Diastolic [mm Hg] | 77.02 ±10.36 | 76.20 ±11.37 | 77.31 ±9.97 | 0.162 |
| eGFR [ml/min/1.73 m2] | 86.00 ±20.26 | 86.56 ±20.27 | 85.80 ±20.27 | 0.663 |
| BMI [kg/m2] | 26.90 ±4.94 | 27.22 ±4.98 | 26.78 ±4.92 | 0.276 |
| Number of drugs used | 2.17 ±1.03 | 2.31 ±1.05 | 2.12 ±1.02 | 0.011 |
| The use of insulin | 154 (15.5) | 26 (10.0) | 128 (17.5) | 0.004 |
| Type of doctor: | ||||
| General practitioners | 213 (21.4) | 84 (32.2) | 129 (17.6) | < 0.001 |
| Residents | 350 (35.2) | 80 (30.6) | 270 (36.8) | |
| Specialists | 431 (43.4) | 97 (37.2) | 334 (45.6) | |
Values are summarised as mean ± SD or median (IQR). Categorical variables are summarised as percentages.
* P-value for statistical significance was obtained using Fisher’s exact test for categorical variables or independent t-test or Mann-Whitney U test for continuous variables, as appropriate. mean ± SD – mean ± standard deviation, median (IQR) – median (interquartile range), HbA1c – glycated haemoglobin, HDL-C – high-density lipoprotein cholesterol, LDL-C – low-density lipoprotein cholesterol, eGFR – estimated glomerular filtration rate, BMI – body mass index.
Clinical inertia and associated factors
This study found that 261 (26.2%) T2DM outpatients experienced clinical inertia. We found four factors associated with clinical inertia: the use of insulin, HbA1c at the index date, the number of drugs used, and the type of doctor. Patients using insulin were associated with reduced risk of clinical inertia compared with patients not using insulin (adjusted OR (95% CI): 0.59 (0.36–0.97)). Patients with HbA1c level ≥ 9.00% at the index date had significantly reduced clinical inertia compared with patients presenting HbA1c level 7.00–7.99% (adjusted OR (95% CI): 0.60 (0.40–0.91)). An increased number of antidiabetic drugs used at the index date was significantly associated with increased clinical inertia experience. Treatment by general practitioners was significantly associated with a longer delay of treatment intensification compared with management by specialists (adjusted OR (95% CI): 0.35 (0.23–0.52)) (Table II).
Table II
Factors associated with clinical inertia among patients with T2DM
| Factor | Crude OR (95% CI) | P-value* | Adjusted OR (95% CI) | P-value** |
|---|---|---|---|---|
| Sex: | ||||
| Female | 1 | |||
| Male | 1.19 (0.89–1.58) | 0.237 | ||
| Age [years] | 1.01 (0.99–1.04) | 0.250 | ||
| Duration of T2DM: | ||||
| 1–5 years | 1 | |||
| > 5 years | 1.14 (0.86–1.51) | 0.369 | ||
| Health insurance: | ||||
| Self-pay | 1 | 1 | ||
| Civil Servant Medical Benefit Scheme | 2.10 (0.90–4.90) | 0.087 | 2.19 (0.91–5.27) | 0.081 |
| Social Health Insurance | 1.17 (0.50–2.74) | 0.723 | 1.03 (0.42–2.50) | 0.948 |
| Universal Coverage Scheme | 1.34 (0.52–3.50) | 0.546 | 1.16 (0.43–3.15) | 0.766 |
| Hypertension | 1.26 (0.90–1.74) | 0.174 | 1.09 (0.77–1.55) | 0.632 |
| Dyslipidaemia | 1.42 (1.03–1.95) | 0.031 | 1.37 (0.97–1.92) | 0.073 |
| Gout | 1.91 (0.85–4.30) | 0.120 | 1.78 (0.75–4.19) | 0.190 |
| HbA1c at index date: | ||||
| 7.00–7.99% | 1 | 1 | ||
| 8.00–8.99% | 0.79 (0.56–1.10) | 0.157 | 0.84 (0.60–1.20) | 0.343 |
| ≥ 9.00% | 0.53 (0.36–0.79) | 0.001 | 0.60 (0.40–0.91) | 0.016 |
| Number of drugs used: | ||||
| 1 | 1 | 1 | ||
| 2 | 1.31 (0.91–1.88) | 0.146 | 1.68 (1.15–2.47) | 0.008 |
| 3 | 1.74 (1.18–2.59) | 0.006 | 2.14 (1.41–3.27) | < 0.001 |
| ≥ 4 | 1.54 (0.92–2.58) | 0.099 | 2.00 (1.12–3.55) | 0.018 |
| The use of insulin | 0.52 (0.33–0.82) | 0.005 | 0.59 (0.36–0.97) | 0.036 |
| Type of doctor: | ||||
| General practitioner | 1 | 1 | ||
| Resident | 0.46 (0.31–0.66) | < 0.001 | 0.42 (0.28–0.62) | < 0.001 |
| Specialist | 0.45 (0.31–0.64) | < 0.001 | 0.35 (0.23–0.52) | < 0.001 |
Discussion
This study showed that in real-world clinical practice in a tertiary teaching hospital in Thailand, the clinical inertia among patients with T2DM aged 40–65 years was 26.2%. This occurrence was quite low compared with related studies [2, 9–11, 14, 18–20]. One possible explanation for this was our patient selection criteria. Our study included T2DM patients who were young and exhibited less comorbidity. The mean age was 55.55 ±6.10 years. The Charlson’s comorbidity index score of most participants was 1 point. Clinical inertia was more frequently observed among older patients [5]. Patients at older age are more prone to hypoglycaemia than younger patients, so physicians tend to increase treatment intensification in a younger age group. In addition, this study selected patients with fewer comorbidities. Patients with more comorbidities tend to use many drugs. Treatment intensification cases should be aware of drug-drug interactions. Therefore, patients with less comorbidity tend to intensify. As a result, patients at younger age and with fewer comorbidities generally receive appropriate treatment intensification [21]. Additionally, there are many specialists in the hospital to educate patients on diabetes. This could be the cause of low occurrence. Furthermore, differences in clinical inertia assessment, including threshold to assess clinical inertia and definition of treatment intensification, may have affected the occurence. First, our study assessed clinical inertia at the index date and subsequent prescription, unlike other studies, which assessed clinical inertia within the timeframe. Second, treatment intensification was defined as any OADs and injectable antidiabetic drugs in our study. Other studies defined it as injectable antidiabetic drugs only [10, 22].
Regarding conducting a study in a tertiary teaching hospital in Thailand, the frequency of clinical inertia in our study was lower than the former study [10]. The different outcomes among these two studies may have been due to the selection of research participants included in the studies and the definition of treatment intensification. Moreover, the former study showed that 38.8%, 46.9%, and 14.3% of the patients were treated by general practitioners, internal medicines practitioners, and endocrinologists, respectively [10]. In our study, patients were treated by general practitioners, residents, and specialists, totalling 21.4%, 35.2%, and 43.4%, respectively. Patients in our study were mostly treated by specialists, unlike in the former study. Treatment by specialists might have made clinical inertia occur less frequently [23].
Factors associated with clinical inertia
Our study found that use of insulin, HbA1c at the index date, number of drugs used, and type of doctor were factors significantly associated with clinical inertia. These factors were similar to related studies.
The use of insulin
Our study revealed that patients with T2DM using insulin had a decreased chance of experiencing clinical inertia. Patients using insulin were more progressive in their disease than patients not using insulin [22]. Another reason was the lack of an upper limit regarding insulin doses [24]. Therefore, physicians tend to intensify treatment to decrease the occurrence of complications.
HbA1c at the index date
Patients with a higher HbA1c at the index date had significantly less clinical inertia. Related studies showed that patients having HbA1c level 8.0–9.0%, and ≥ 9.0% had a significantly shorter time to reach treatment intensification than patients with an HbA1c level 7.0–8.0% [25]. This result was consistent with Lin et al., who showed that a higher index HbA1c significantly reduced the occurrence of clinical inertia (p < 0.001) [9]. Patients with HbA1c level ≥ 8.0% had 5.52 times greater risk of intensification than patients with HbA1c level < 6.5% (p < 0.001) [26]. Evidence from a large real-world dataset revealed that patients who had HbA1c level ≥ 9.0%, 8.0–8.9%, and 7.0–7.9% received treatment intensification of 59.6%, 46.7%, and 28.4%, respectively [4]. One possible explanation is that physicians may be less inclined to intensify therapy among patients having an HbA1c level near the target [2, 25]. They possibly recommend lifestyle modification instead [19, 20]. Patients having an extremely high HbA1c level above target often experience treatment intensification because controlling the glucose level within the target is beneficial in reducing complications [27–30].
Number of drugs used
In our study, an increase in the number of drugs used at the index date was associated with experiencing clinical inertia. However, the association between the number of drugs used and clinical inertia in T2DM remains ambiguous, in contrast with other studies. Lin et al. found that an increase in the number of drugs used significantly increased the prevalence of clinical inertia (p < 0.001) [9], similarly to our study. Ruiz Negron et al. found that clinical inertia was associated with a higher number of baseline antidiabetic drugs [19]. In contrast, the results of the study by Osataphan et al. showed that patients receiving more than two OADs had 1.4 times greater insulin initiation than patients receiving two OADs (p = 0.51) [10]. Khunti et al. found that patients using a higher number of OADs received significantly more treatment intensification with insulin than patients with a lower number of OADs (p = 0.0012) [22]. Patients using a higher number of drugs were more prone to clinical inertia because adding more antidiabetics is probably less desirable for patients already using a high number of drugs. Additionally, treatment intensification increased drug-drug interactions, medication-related adverse events, and polypharmacy [19, 21].
Type of doctor
The type of treating doctor was also found to be associated with clinical inertia. Our study found that treatment by a specialist was less likely to result in clinical inertia than treatment by a general practitioner (p < 0.001). The Osataphan et al. study also found that treatment by general practitioners was 2.95 times more likely to result in clinical inertia than treatment by specialists [10]. The study by Shah et al. also found that specialists’ care (45.1%) was more intensive than general practitioners’ care (37.4%) (p = 0.009) [23]. Patients treated by general practitioners experienced more clinical inertia because general practitioners have less experience in treatment than specialists and are less certain about optimal drug choices [9]. Given this finding, a need was observed for general practitioners to undertake confirming professional education to manage patients with T2DM.
Other factors
Aside from significantly associated factors, health insurance plans were revealed as an interesting factor. This study found that a difference in health insurance was not associated with clinical inertia, similarly to the study by Osataphan et al. [10]. This result revealed that health insurance plans did not have an impact on T2DM treatment in Thailand because all health insurance plans cover an essential drug (ED). Antidiabetic drugs in the essential drug are optimal and sufficient for treating diabetes, and basic laboratory tests and treatment by specialists are covered by all health insurance plans.
Limitations
This study encountered limitations. First, this study employed a retrospective observational design. We were concerned about missing data, including adherence and lifestyle modifications. Second, we also did not know the reasons why doctors did not add new drugs or increased the dose of existing drugs because this was not recorded in the OPD cards. Third, we were unable to collect analysis data concerning the patient’s socio-economic and education level, occupation, and level of patient diabetes knowledge, to determine whether these variables influenced clinical inertia. Fourth, this study was conducted in a tertiary care hospital. Different factors regarding lower level hospitals and the community setting would be involved such as availability of drugs, knowledge of doctors, etc. While these results make a valuable contribution, they should be interpreted with caution.
In conclusion, the clinical inertia in this study was about 26%. The finding of this study revealed that the use of insulin, HbA1c at the index date, number of drugs used, and type of doctor were associated with clinical inertia. A better understanding of clinical inertia and the specific related interventions should be developed to more precisely address this problem.