Introduction
Office and out-of-office blood pressure (BP) levels are associated with a greater risk of cardiovascular (CV) and renal events [1]. It is also known that ambulatory BP monitoring (ABPM) is a better predictor of hypertension-mediated organ damage (HMOD) and fatal CV outcomes than conventional measurements [2].
Blood pressure has a physiological circadian pattern with a normal decrease during sleep, so it has been proposed to define as non-dippers and dippers individuals with a fall of mean night-time BP < 10% and ≥ 10% than the average daytime values, respectively [3]. Indeed, it is well known that the risk of CV disease and mortality is higher in non-dipper hypertensive individuals, independently of mean BP [4].
Recent evidence suggests that inflammation, immunity and arterial hypertension (AHT) are related to each other, triggering an inflammatory process that might increase BP and lead to HMOD and CV disease supporting a correlation between vascular and renal damage with the establishment and progression of arterial hypertension mediated by pro-inflammatory cytokines, redox imbalance and a positive feedback mechanism between them [5].
Furthermore, multiple studies have been designed to evaluate the role of certain inflammatory markers in hypertensive patients such as uric acid [6], ultra-sensitive C-reactive protein (US-CRP) [7, 8], platelet count (PTC) [9], erythrocyte sedimentation rate (ESR) [10], fibrinogen [11] and ferritin [12] in an attempt to quantify inflammation.
Some others also hypothesize that inflammatory status could play a role in alterations of BP circadian rhythm [13–15]. However, it is less well known if this relationship could be independent of BP levels themselves. Hence, the aim of our study is to compare the levels of usual inflammatory markers in patients with and without circadian blood pressure abnormalities.
Material and methods
Study design and sample
This is a study with a temporal cross-sectional design conducted in a department of internal medicine (Hypertension and Cardiovascular Risk Unit) from January 2008 to December 2014 which included patients with normal and high BP levels older than 18 years. All patients and variables were collected at the date of the first consultation and there was no subsequent follow-up. Analysis was performed years after data collection at a specific point retrospectively.
Individuals with secondary AHT, coronary arterial or cerebrovascular disease, acute or chronic renal impairment, acute or chronic inflammation or infectious disease, fever, malignancy or hematological disease were excluded from the study. Patients with acute or chronic respiratory diseases including obesity hypoventilation syndrome and sleep apnea syndrome were also excluded.
Parameters of clinic blood pressure and ambulatory blood pressure monitoring collection
Systolic BP (SBP), diastolic BP (DBP) and heart rate (HR) of each patient were automatically measured every 20 min during the day (07:00 a.m. to 11:00 p.m.) and every 30 min during the night for 24 consecutive hours with an oscillometric Space-Labs 90207 device (Space-Labs Inc., Redmon, Washington). They were instructed to go about their usual activities with minimal restrictions but to follow a similar schedule during the day of ABPM. The BP cuff was worn on the non-dominant arm with cuff size determined by upper arm circumference at each study visit. During monitoring each subject kept a diary of their activities and time of retiring to bed so ABPM recordings were subdivided into awake or asleep periods based on such diary entries. The method was considered reliable if > 70% of measurements were valid. Our study has complied with the recommendations of the main international clinical practice guidelines on ABPM [4, 16] and our patients have filled in a diary referring to sleep quality.
Patients were separated into two groups according to the circadian profile of BP (dipper and no dipper groups) based on the results of the 24-hour ABPM. The dipper pattern was defined as a decrease in mean nocturnal blood pressure ≥ 10% of mean diurnal BP [3].
Clinical and laboratory variables
All individuals were assessed for demographic characteristics, CV risk factors, including smoking status (non-smokers/current or former smokers), alcohol intake (no consumption/consumption of any quantity), body mass index (BMI), waist circumference, diabetes mellitus (DM), hyperlipidemia (HLP), AHT, and used drugs.
Arterial hypertension and HLP were defined according to the European Society of Cardiology Clinical Practice Guidelines [17, 18]. Diabetes mellitus was considered according to American Diabetes Association guidelines (ADA) [19]. Waist perimeter was measured with the same standardized tape measure in all cases. Infection and acute illness were determined based on the anamnesis and physical examination.
Blood samples were obtained at 08:00 p.m. following overnight fasting. The following analytical variables were collected: complete blood count and biochemical parameters including serum glucose, creatinine, and uric acid, lipid profile (total and fractionated cholesterol, triglycerides), US-CRP, ESR, ferritin and fibrinogen.
Based on the evidence on inflammation in the pathogenesis of AHT and according to a possible role of some noted parameters in its quantification, we decided to select as inflammatory markers uric acid, US-CRP, PTC, ESR, fibrinogen and ferritin [6–12].
Possible biases and ethical aspects
In order to minimize bias, only the patients who were sent for ABPM to our consultation were finally selected. The variables of interest were collected according to the information provided by the regional digital health records (IANUS, SERGAS).
Non-categorical predictive variables of interest (age, BMI, waist circumference, HR and analytical parameters) were categorized independently of the initial type of variable to improve the efficiency of multivariate analysis and to manage confusion and interaction [20]. Thresholds for categories were chosen as the median of each variable over the study sample.
Sample size was determined by the total number of recruited patients in the department. This study was approved by the state Ethics Committee of Clinical Research and adhered to the ethical standards outlined in the Helsinki Declaration. All subjects gave written informed consent.
Statistical analysis
Statistical analysis was performed using SPSS version 22 for Windows (IBM Corp., Armonk, NY, USA). An assessment of the normality of continuous data was tested by using the Kolmogorov-Smirnov test. A t-test was performed and the results are shown as mean ± standard deviation (SD). Qualitative variables were evaluated using the χ2 statistic test and the results are shown as the relative risk estimation adjusted by the Mantel-Haenszel method. We used multivariate techniques to perform a statistical analysis of interaction and confounding. Multivariate logistic regression was performed including variables that were statistically significant based on univariate analysis with a p-value < 0.05 to identify which of them were associated with non-dipper status in order to construct a receiver operating characteristics (ROC) model.
Results
The study included 551 patients (mean age of 54 years, 47% women) with a total of 379 individuals in the dipper group (mean 24-hour SBP and DBP: 128 ±12 mm Hg and 78 ±10 mm Hg) and a total of 172 patients in the non-dipper group (mean 24-hour SBP and DBP: 129 ±15 mm Hg and 74 ±11 mm Hg). The sample consisted of 508 (92%) hypertensive patients with a total of 382 (69%) and 160 (29%) suffering from HLP and DM respectively.
A total of 303 (54%) patients were under treatment and the most prevalent therapeutic group was RAS blockers (50%). Angiotensin II receptor blocker use was more frequent in the non-dipper group. Baseline demographic and clinical characteristics are summarized in Table I.
Table I
Baseline demographic and clinical characteristics
| Variables | All patients (n = 551) | Dipper (n = 379) | Non-dipper (n = 172) | P-value |
|---|---|---|---|---|
| Age [years]* | 54 ±14 | 51 ±14 | 60 ±13 | < 0.001 |
| Women, n (%)** | 266 (47) | 180 (47) | 82 (47) | NS |
| Waist circumference [cm]* | 100 ±12 | 98 ±12 | 104 ±12 | < 0.001 |
| BMI [kg/m2]* | 31 ±12 | 31 ±14 | 31 ±5 | NS |
| HR [bpm]* | 71 ±13 | 71 ±12 | 71 ±13 | NS |
| Current/Former smokers, n (%)** | 179 (32) | 118 (31) | 57 (33) | NS |
| Alcohol intake, n (%)** | 188 (34) | 129 (34) | 55 (32) | NS |
| Hypertension, n (%)** | 508 (92) | 332 (87) | 166 (96) | < 0.001 |
| Hyperlipidemia, n (%)** | 382 (69) | 235 (62) | 136 (79) | < 0.001 |
| Diabetes mellitus, n (%)** | 160 (29) | 77 (20) | 74 (43) | < 0.001 |
| SBP in consultation [mm Hg]* | 144 ±18 | 144 ±18 | 146 ±18 | NS |
| DBP in consultation [mm Hg]* | 84 ±11 | 85 ±10 | 81 ±12 | < 0.001 |
| SBP, 24 h [mm Hg]* | 128 ±13 | 128 ±12 | 129 ±15 | NS |
| SBP, awake [mm Hg]* | 133 ±13 | 134 ±12 | 130 ±15 | 0.001 |
| SBP, asleep [mm Hg]* | 119 ±14 | 115 ±11 | 127 ±15 | < 0.001 |
| DBP, 24 h [mm Hg]* | 76 ±10 | 78 ±10 | 74 ±11 | < 0.001 |
| DBP, awake [mm Hg]* | 81 ±11 | 83 ±10 | 75 ±11 | < 0.001 |
| DBP, asleep [mm Hg]* | 68 ±9 | 67 ±9 | 71 ±10 | < 0.001 |
| Antihypertensive drugs, n (%)** | 303 (54) | 164 (43) | 128 (74) | < 0.001 |
| RAS blockers, n (%)** | 278 (50) | 153 (40) | 114 (66) | < 0.001 |
| ACEI, n (%) | 37 (6.7) | 24 (6.3) | 13 (7.6) | NS |
| ARBs, n (%) | 226 (41) | 128 (33) | 98 (57) | < 0.001 |
| Anti-aldosterone agents, n (%) | 14 (2.5) | 3 (0.8) | 11 (6.4) | < 0.001 |
| Statins, n (%) | 176 (32) | 94 (24) | 82 (47) | < 0.001 |
| Compliant patients, n (%)*** | 328 (94.8) | 205 (94.9) | 123 (94.6) | NS |
Among all patients, mean glucose and creatinine levels were 110 ±35 mg/dl and 0.9 ±0.2 mg/dl. Mean total and low density lipoprotein cholesterol (LDL-C) levels were significantly higher in the dipper group (204 ±41 and 127 ±34 mg/dl vs. 190 ±43 and 114 ±36 mg/dl, p < 0.001). Main analytical findings are summarized in Table II.
Table II
Analytical findings
| Variables | All patients (n = 551) | Dipper (n = 379) | Non-Dipper (n = 172) | P-value |
|---|---|---|---|---|
| FPG [mg/dl]* | 110 ±35 | 105 ±35 | 118 ±34 | < 0.001 |
| Creatinine [mg/dl]* | 0.9 ±0.2 | 0.92 ±0.2 | 0.98 ±0.2 | 0.004 |
| TG [mg/dl]* | 127 ±79 | 126 ±84 | 127 ±69 | NS |
| TC [mg/dl]* | 199 ±42 | 204 ±41 | 190 ±43 | < 0.001 |
| LDL-C [mg/dl]* | 122 ±35 | 127 ±34 | 114 ±36 | < 0.001 |
| HDL-C [mg/dl]* | 47 ±15 | 48 ±15 | 45 ±14 | NS |
| Uric acid [mg/dl]** | 6.0 ±4.1 | 5.6 (4.6–6.7) | 6.0 (4.9–6.9) | 0.034 |
| ESR [mm/h]* | 15 ±24 | 13.6 ±21.6 | 19.1 ±29.7 | 0.017 |
| US-RCP [mg/l]* | 0.9 ±2.8 | 0.9 ±3.1 | 0.7 ±2.1 | NS |
| Fibrinogen [mg/dl]* | 385 ±67 | 380 ±64 | 394 ±73 | 0.028 |
| Ferritin [mg/dl]* | 124 ±126 | 121 ±127 | 132 ±126 | NS |
| PTC [103/µl]* | 250 ±61 | 256 ±62 | 237 ±59 | 0.001 |
| MPV [fl]* | 9.1 ±1.1 | 9.1 ±1.1 | 9.0 ±1.1 | NS |
| Leukocytes [103/ul]* | 7.38 ±1.9 | 7.37 ±1.9 | 7.42 ±2.0 | NS |
| Hemoglobin [g/dl]* | 14.5 ±5 | 14.4 ±1.3 | 14.7 ±8.8 | NS |
FPG – fasting plasma glucose, TG – triglyceride, TC – total cholesterol, LDL-C – low-density lipoprotein cholesterol, HDL-C – high-density lipoprotein cholesterol, ESR – erythrocyte sedimentation rate, US-CRP – ultra-sensitive C-reactive protein, PTC – platelet count, MPV – medium platelet volume. Results expressed as
The group of non-dipper patients had a higher percentage of individuals with higher ESR (OR = 1.77, 95% CI: 1.23–1.55, p = 0.001), uric acid (OR = 1.50, 95% CI: 1.04–2.16, p = 0.028) and fibrinogen (OR = 1.72, 95% CI: 1.18–2.51, p = 0.001) levels than those of the control group. A higher percentage of patients with higher PTC was observed in the dipper group (OR = 0.54, 95% CI: 0.37–0.78, p = 0.005). These results were independent of age, waist circumference, presence of AHT, DM or HLP, and use of antihypertensive drugs including RAS blockers (Table III).
Table III
Univariate and multivariate analysis
Age, waist perimeter, presence of AHT, DM or HLP, RAS blockers and statin use, ESR, uric acid, fibrinogen and PTC were included in a stepwise regression model. Variables that maintained statistical significance in multivariate analysis were the presence of DM, ESR, uric acid, fibrinogen and PTC.
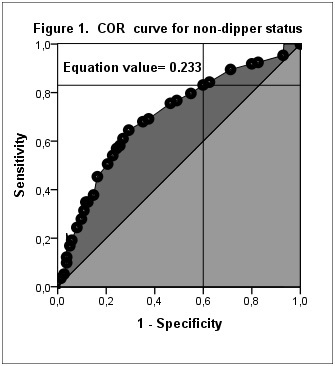
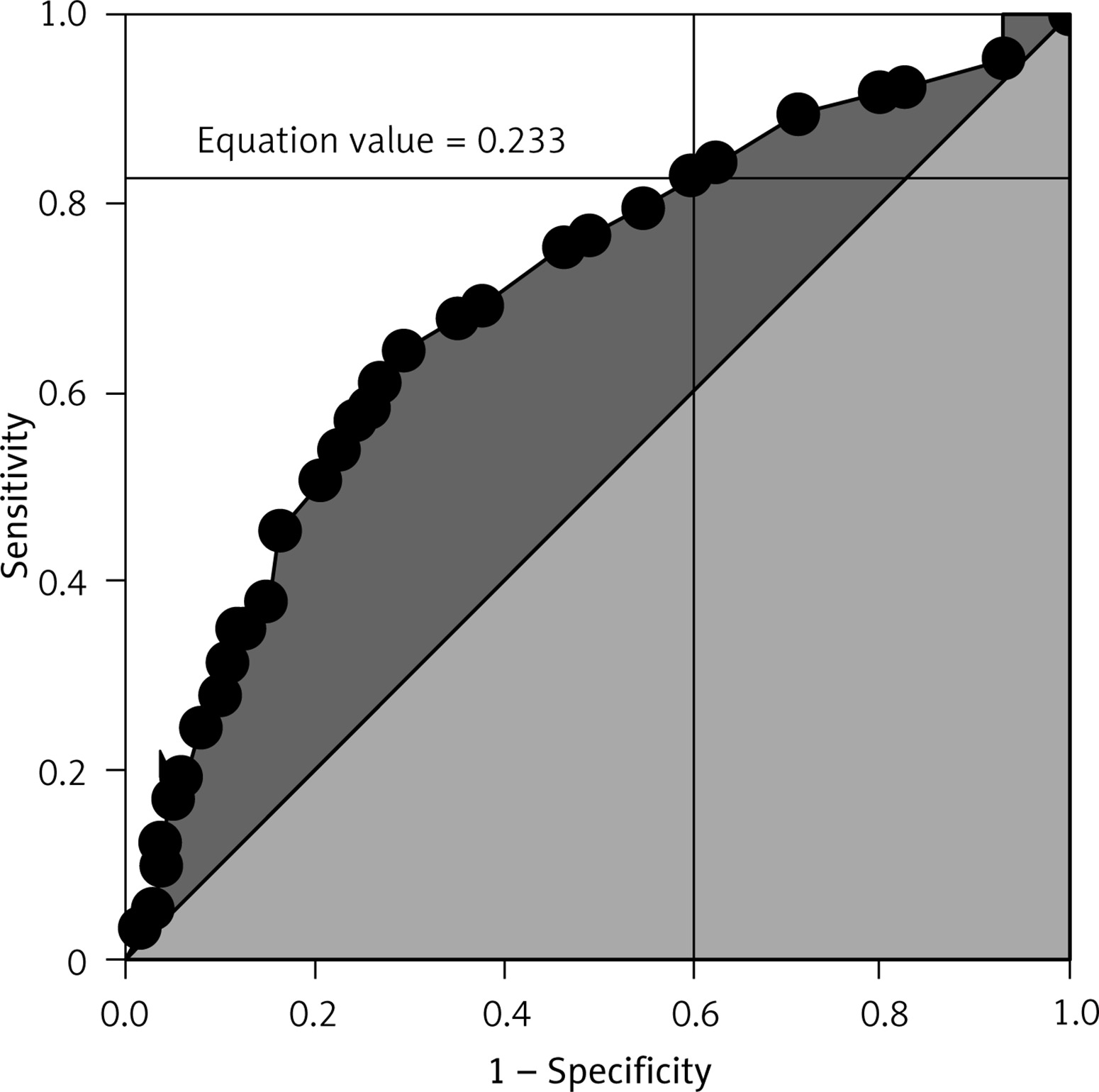
The model equation is summarized in Table III. A model equation value of 0.233 or higher predicted non-dipper status with 83% sensitivity and 40% specificity (AUC (area under curve) ± SE (standard error) = 0.702 ±0.024, 95% CI: 0.654–0.750, p < 0.001) (Figure 1).
Discussion
Our approach was that patients with impaired circadian BP rhythm could be associated with an unfavorable inflammatory status. In our study, the main results were that patients in the non-dipper group had higher levels of some conventional inflammatory markers (such as ESR, uric acid and fibrinogen) and lower PTC than those in the dipper group with statistical significance and independently of possible confounding and/or interaction variables such as presence of AHT, DM or HLP, age, waist circumference and differential use of drugs including RAS blockers.
There is increasing evidence of a relationship between hypertension and inflammation [5] and some inflammatory markers have been studied in this context [6–12]. However, the correlation between alterations in the circadian profile of BP and inflammation in hypertensive patients is a less studied aspect and nothing is known of this possible correlation in normotensive patients.
C-reactive protein (CRP) is a pentaxin synthesized primarily in the liver in response to pro-inflammatory cytokines that is one of the best known markers of CV disease. C-reactive protein and especially US-CRP levels were shown to predict the development of AHT and were associated with endothelial dysfunction, atherosclerosis, HMOD and CV events in hypertensive patients [21, 22].
Although the exact mechanisms underlying the relationship between alteration of circadian rhythm of BP in hypertensive patients and development of HMOD and CV events are unknown, it has been attributed to inflammation and some studies suggest that US-CRP levels could play a role [7, 13]. However, in our study we did not observe significant differences between the groups and our results were also consistent with those from some other similar studies [23, 24].
The differences found in ESR between groups in both qualitative and quantitative analysis should be highlighted because it is a scarcely commented aspect in the literature reviewed [25]. It is known that ESR is a nonspecific marker of inflammation that may also rise because of non-inflammatory causes such as patient age or presence of anemia. In our study, there were significant differences in age between the groups, but age-adjusted results maintained significant differences. In this sense it is possible that higher ESR is correlated with higher levels of pro-inflammatory molecules that we are not measuring [26].
In another vein, asymptomatic elevation of uric acid is considered a cardiovascular risk factor and patients with AHT have higher levels of uric acid [27]. Some pathogenic models suggest that high blood levels of uric acid are able to produce renal dysfunction due to hyperactivation of the RAS system, redox imbalance and microvascular disease, and vascular endothelial dysfunction leading to initially reactive and finally established AHT due to inflammation and remodeling [6]. Along these lines, some studies including ours suggest that non-dipper patients have higher uric acid levels [13, 21].
Fibrinogen is an acute phase reactant component of the coagulation cascade with a half-life of 1 week [28]. The role it could play as an added marker in the evaluation of inflammatory status of patients with BP abnormalities is a scarcely studied aspect. In our study, fibrinogen levels were higher in non-dipper patients and these results were consistent with those of some similar studies [29]. However, we must bear in mind that there is a strong correlation between ESR and fibrinogen levels [26] but ESR-adjusted results maintained significant clinical and statistical differences.
Recent literature suggests the existence of an association between blood cell abnormalities related to platelet and white blood cell (WBC) counts and activity with inflammation [30, 31]. In this line, some studies provide results in the same way according to a lower platelet count in non-dipper patients although the medium platelet volume (MPV) was identical in both groups [32]. However, our study was not designed for the specific assessment of any leukocyte index although there were no significant differences in the overall WBC count between groups.
In another vein, disability of the RAS axis has been widely studied in the development and progression of AHT. The literature also supports the existence of an anti-inflammatory and anti-degenerative effect of some antihypertensive drugs, of which a representative group would be RAS blockers [33]. In our study there were differences in drug use between the groups consisting of a higher percentage of non-dipper patients under treatment with a higher rate of RAS blockers use although the treatment-adjusted analysis showed no differences. In addition, only a small unquantified percentage of individuals had night time drug use.
The beneficial impact of the pleiotropic effect related to HMG-CoA reductase inhibitors use on the CV health of patients with atherogenic dyslipidemia is also known [18]. In this sense, our results show that there was a higher frequency of statin use in non-dipper patients, which could be in part because they are often patients with a higher CV risk, and greater prevalence of DM and HLP. These findings could partially justify the paradox regarding the results related to the LDL-C levels observed in both groups (Table II).
Given the study design, most patients were screened for DM prior to their inclusion in primary care units. In a small percentage of patients included in the study with suspected and undiagnosed DM (n = 22 participants), HbA1c was requested in order to rule out or confirm the diagnostic suspicion. For this reason, we only have the HbA1c data of these patients which were collected from the first blood analysis in our consultation.
It was a cross-sectional design study with retrospective data analysis in which we have to take into account the possibility of biases related to design. The variables of interest had a similar distribution to those prevailing in the rest of the Caucasian hypertensive patients of our region, since it was a single-center study with a population from the health area of our hospital. In this sense, we must interpret the results cautiously when thinking about applying them to populations that might have other baseline characteristics, diagnostic criteria or thresholds for certain factors.
We have to remark that it is a study of real clinical practice in which all selected patients were referred from primary care to perform ABPM, with a large sample size and great number of variables collected in which we decided not to match groups to maintain good statistical power and external validity and we addressed confusion and/or interaction phenomena during the analysis phase through stratification and multivariate techniques.
We emphasize that our study contained about 8% non-hypertensive patients. In this line, blood pressure-adjusted results for uric acid, fibrinogen, ESR and PTC maintained significant differences, so it would not be far-fetched to think about a relationship between alteration of BP circadian profile and inflammatory status independently of BP levels. However, more studies and better quality of evidence are necessary.
To summarize, the results of our study seem to be favorable to establish the existence of differences in the levels of inflammatory markers between patients with and without alterations in the circadian profile of BP, which could suggest a pro-inflammatory status in those patients without an adequate nocturnal decrease in BP. This study could be the starting point for others with a higher quality design to evaluate the effect that reversal to normal of the circadian profile could have on these inflammatory markers taking into account that the parameters studied in our research have been shown to be accessible, cheap and close to the routine clinical practice of a high blood pressure and cardiovascular risk consultation.
In conclusion, we found that patients with impaired circadian BP rhythm were associated with an unfavorable inflammatory status independently of BP levels (increased uric acid and fibrinogen levels, higher ESR and decreased PTC). This fact could play a role in the prognostic differences observed between dipper and non-dipper patients. The authors suggest that assessment of inflammatory markers should be included as part of the evaluation and follow-up of hypertensive patients, especially those with altered BP profile.