Early childhood is a critical period for neurodevelopment, during which biological maturation, prenatal development, and the social environment interact to shape later cognitive, motor, and socioemotional functioning. Among the factors that can influence a child’s progress prenatally, maternal smoking is particularly important, as it has been associated with adverse outcomes in several domains of early childhood development, regardless of gestational age and birth weight [1–3]. On the other hand, several studies have shown that longer and exclusive breastfeeding positively affects communicative, motor, and personal and social development and reduces the risk of neurological impairment [4, 5]. These findings highlight the importance of systematic developmental monitoring and early identification of modifiable risk factors during the first years of life.
Standardised developmental screening tools are widely recommended, to aid in the early detection of developmental vulnerabilities and timely referral for early intervention. The Ages & Stages Questionnaire, Third Edition (ASQ-3) is a validated parent-administered screening instrument that assesses development in 5 domains: communication, gross motor skills, fine motor skills, problem-solving, and personal–social development [6]. The ASQ-3 has been successfully applied in population-based and early childhood intervention studies in diverse cultural and socioeconomic contexts [7].
Despite its wide international application, population-based data derived from standardised developmental screening instruments remain limited in Bulgaria. Existing national studies have focused primarily on high-risk neonatal populations, while studies examining typically developing children in infancy using validated screening instruments are scarce. The present study aimed to investigate the biological, pregnancy-related, and social determinants of early childhood development in a Bulgarian kindergarten cohort using the ASQ-3.
This cross-sectional study included children who were born at term and were attending 3 daycare centres in Ruse, Bulgaria, between January and October 2025. Children with prematurity, congenital anomalies, genetic syndromes, or chronic medical conditions potentially affecting development were excluded. Of the 246 initially screened children, 167 met the inclusion criteria, and parents provided written consent to participate in the study. The study was conducted in accordance with the principles of the Declaration of Helsinki. Formal approval by an ethics committee was not required because the study involved non-invasive developmental screening using a parent-completed questionnaire and did not include any medical interventions. Participation was voluntary, and written informed consent was obtained from all parents or legal guardians prior to inclusion. All data were collected anonymously and analysed in aggregated form. The final sample included children aged 14–42 months, of whom 52% were girls.
Children’s development was assessed using parent-completed ASQ-3 questionnaires. A preliminary comparison of parent-, teacher-, and researcher-completed questionnaires conducted during the baseline phase of the study demonstrated the highest concordance between parent ratings and ratings performed by the principal investigator (Table I). Based on these findings, parent reports were used for all subsequent assessments. ASQ-3 domain scores were analysed as continuous variables.
Table I
Mean ranks of ASQ-3 total scores according to the type of rater (Friedman test)
| Rater | Mean rank |
|---|---|
| Teachers | 1.35 |
| Parents | 2.32 |
| Investigator | 2.33 |
Data on potential developmental determinants were collected through parental questionnaires completed at the time of informed consent. Predictors examined included child sex, birth weight, gestational age, maternal smoking during pregnancy, thyroid disease requiring hormone replacement therapy, hypertensive disorders of pregnancy, thrombophilia, mode of delivery, duration of breastfeeding, maternal education level, family structure, and home language environment.
Statistical analysis were performed using Pearson correlation coefficients (two-tailed), with statistical significance set at p < 0.05.
Of the 167 children included in the analysis, 116 scored above the ASQ-3 observation zone in all developmental domains. Fifty-one children presented with at least one domain falling within the observation zone or requiring referral for specialist intervention. A follow-up developmental screening conducted 6 months later showed improvement above the observation thresholds in 38 of these children. Six children remained with one domain within the observation zone and continued to be monitored, while 7 children showed persistent developmental difficulties requiring continued specialist support.
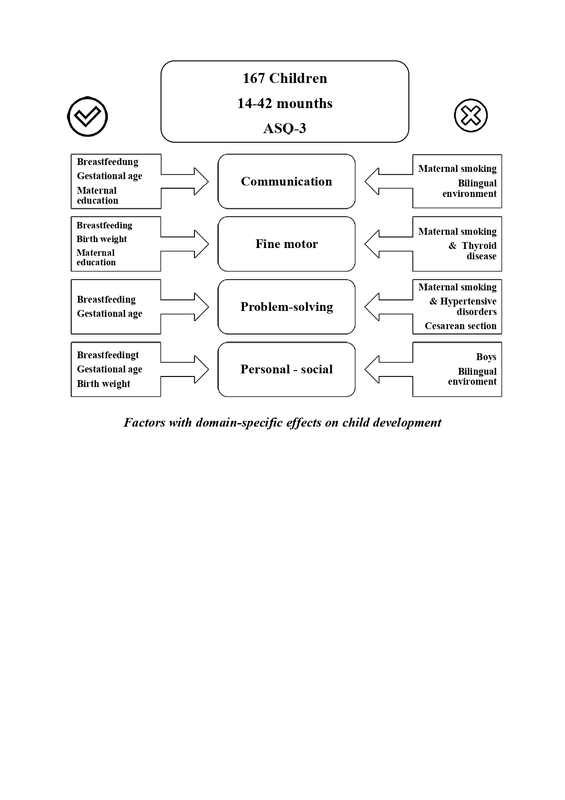
Several significant relationships were identified between developmental outcomes and the predictors studied. Higher communication scores were positively associated with longer duration of breastfeeding (r = 0.230, p = 0.003), higher maternal education (r = 0.222, p = 0.004), and older gestational age at birth (r = 0.206, p = 0.008). Negative associations were observed with maternal smoking during pregnancy (r = –0.254, p = 0.001) and a bilingual home language environment (r = –0.186, p = 0.016). These findings are consistent with previous evidence highlighting the role of breastfeeding, parental educational resources, and gestational maturity in language development [1, 4, 5] (Table II).
Table II
Pearson correlation coefficients for ASQ-3 domain scores and selected predictors
Fine motor development was positively associated with birth weight (r = 0.230, p = 0.003), duration of breastfeeding (r = 0.215, p = 0.005), and maternal education (r = 0.206, p = 0.008). In contrast, negative associations were found with maternal smoking during pregnancy (r = –0.237, p = 0.002) and maternal thyroid disease requiring hormone replacement therapy (r = –0.227, p = 0.003), supporting existing evidence linking prenatal health conditions to early motor maturation [1, 8].
Problem-solving scores were positively correlated with gestational age (r = 0.254, p = 0.001) and duration of breastfeeding (r = 0.242, p = 0.002). Lower scores were observed among children born by caesarean section (r = –0.216, p = 0.005), those exposed to maternal smoking during pregnancy (r = –0.247, p = 0.001), those whose mothers had hypertensive disorders during pregnancy (r = –0.167, p = 0.031), and children raised in non-marital cohabiting families (r = –0.172, p = 0.026).
Measures of personal and social development were positively correlated with gestational age (r = 0.155, p = 0.045), breastfeeding duration (r = 0.168, p = 0.030), and maternal education level (r = 0.183, p = 0.018). Lower scores were observed among boys (r = –0.252, p = 0.001) and among children raised in bilingual households (r = –0.191, p = 0.013), consistent with evidence that early bilingual exposure may be associated with temporary differences in socio-communicative outcomes in early life without suggesting a long-term problem [9].
No statistically significant associations were observed between maternal thrombophilia or place of residence (urban versus rural) and any ASQ-3 developmental domain.
Overall, these findings highlight the combined influence of biological maturity, maternal health-related behaviours, and social context on early childhood development. Duration of breastfeeding, maternal education, and gestational age emerged as consistent positive determinants, while prenatal smoking was the strongest negative predictor across multiple developmental domains. Importantly, the documented improvement in a significant proportion of children after structured follow-up and provision of stimulating activities highlights the potential value of early developmental monitoring combined with parent-directed activities and timely referral. Routine developmental screening using the ASQ-3 in kindergartens may therefore aid in the early identification of modifiable risk factors and inform preventive strategies and public health policies aimed at optimising early developmental outcomes.