Burns are a leading cause of accidental injury and disability in children worldwide, imposing substantial physical pain, psychological trauma, and economic burden on affected children, their families, and the global healthcare system [1, 2]. Paediatric burns are particularly concerning due to children’s immature skin barrier, limited hazard recognition ability, and poor self-protection awareness, which not only increase their vulnerability to burn injuries but also elevate the risk of long-term complications such as scar contracture, functional impairment, and post-traumatic stress disorder. Notably, epidemiological characteristics of paediatric burns (including aetiology, age distribution, injury setting, and severity) vary significantly across regions due to differences in socioeconomic development, living habits, care patterns, and healthcare access [3–6].
Hangzhou, a major city in eastern China with rapid urbanisation and distinct urban-rural differences, has unique dietary habits, family care models, and living environments, which may lead to specific epidemiological features of paediatric burns that differ from other regions. However, there is a lack of large-sample, long-term retrospective studies on paediatric burns in Hangzhou in recent years, resulting in insufficient evidence-based support for formulating targeted local prevention and control strategies, optimising clinical management protocols, and reducing the incidence and disability rate of paediatric burns. Therefore, this study aimed to fill this research gap by analysing 1184 hospitalized paediatric burn patients from the period 2020 to 2024, clarifying the epidemiological characteristics of paediatric burns in this region, and highlighting the study’s significance for future clinical practice and public health intervention.
Methods
Patient enrolment
All families had visited the Children’s Hospital of Zhejiang University School of Medicine, Hangzhou, Zhejiang Province, China. The institutional review board of the Children’s Hospital of Zhejiang University School of Medicine (2023-IRB-0219-P-01) approved this study. Informed written consent was obtained from all the participants in this study.
The inclusion criteria for patients were as follows: (1) first hospitalisation after burn injury; (2) less than 14 years old; and (3) admitted between 1 January 2020 and 31 December 2024. The exclusion criteria for patients were as follows: (1) patients who were transferred or discontinued treatment less than 24 h after admission and (2) were readmitted after burn injury due to chronic wounds, scar reconstruction, or rehabilitation. Demographic data (total number, annual number, age, gender), burn conditions (site, area, depth, severity), injury factors and environment (cause of injury, family source, location), and injury occurrence time (time and month) were collected. Postinjury management included prehospital treatment, postadmission treatment, surgical and nonsurgical treatment, length of stay, and outcome. On the day of discharge, the clinical outcome was divided into cured, improved, otherwise, and dead, as follows: cured – the wound healed completely; improved – most of the wound healed (> 50% wound area); otherwise – the wound was not healed, or the patient was discharged from the hospital within a short period (≤ 3 days) against medical advice.
Statistical analysis
After the data were collected, sorted, and checked, the χ2 test was performed to evaluate the gender distribution of the children at different ages, and Fisher’s exact probability method was used to compare the causes of injury. Prehospital treatment and outcome were tested by the Wilcoxon rank sum test. A t-test was performed to compare the length of hospital stay among patients who underwent different wound treatment methods. P < 0.05 was considered to indicate statistical significance.
Results
Age and gender
A total of 1184 children (< 14 years) were hospitalised for burn injuries during the period 2020–2024 (217 in 2020, 212 in 2021, 260 in 2022, 256 in 2023, and 239 in 2024). Overall, 707 patients were male (59.7%) and 477 were female (40.3%), yielding a male-to-female ratio of 1.48 : 1. By age category, children aged ≥ 1 and < 3 years represented the largest proportion (63.1%). The gender distribution did not differ significantly across age groups (χ2 = 5.635, p > 0.05) (Supplementary Table SI).
Burn characteristics. Among the 1184 inpatients, 261 (22.0%) sustained burns at a single site, whereas 923 (78.0%) had involvement of two or more body regions. The most frequently affected areas were the trunk (691, 58.4%) and upper limbs (610, 51.5%), followed by the head/face/neck (518, 43.8%) and lower limbs (532, 44.9%); buttocks/perineum burns were less common (142, 12.0%). Total body surface area (TBSA) involvement ranged from 1% to 80%. Most children had moderate-sized burns, with 722 (61.0%) involving 5–15% TBSA; 100 (8.4%) had < 5% TBSA, 270 (22.8%) had 15–25% TBSA, and 92 (7.8%) had ≥ 25% TBSA. Regarding depth, shallow second-degree burns accounted for 215 cases (18.2%), mixed shallow-to-deep second-degree burns for 632 (53.4%), deep second-degree burns for 170 (14.4%), deep second-degree to third-degree burns for 92 (7.8%), and third-degree burns for 75 (6.3%). Based on area and depth, burn severity was classified as mild in 52 (4.4%), moderate in 816 (68.9%), severe in 225 (19.0%), and extremely severe in 91 (7.7%) (Supplementary Table SII).
Aetiology
Hydrothermal scalds (e.g. hot water, soup, oil) were the dominant cause, affecting 1100 (92.9%) children. Flame burns accounted for 51 (4.3%) cases, including gas explosions, electrical fires, carbon fires, fireworks, and related mechanisms. Other aetiologies were uncommon: electric burns (8), chemical burns (9; e.g. wormwood exposure, cleaning agents, lime water), thermal compression injuries (9; e.g. sealing machines, conveyor belts), and hot solid burns (7; e.g. metal, paper ash, incense ash). With increasing age, scald-related burns decreased, while flame and other causes increased (χ2 = 92.060, p < 0.01) (Supplementary Table SIII).
Setting and timing
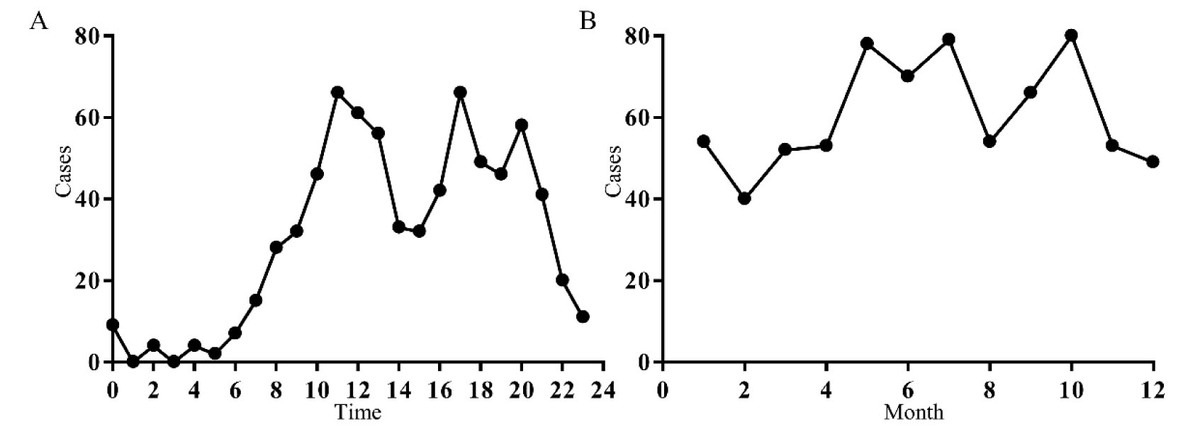
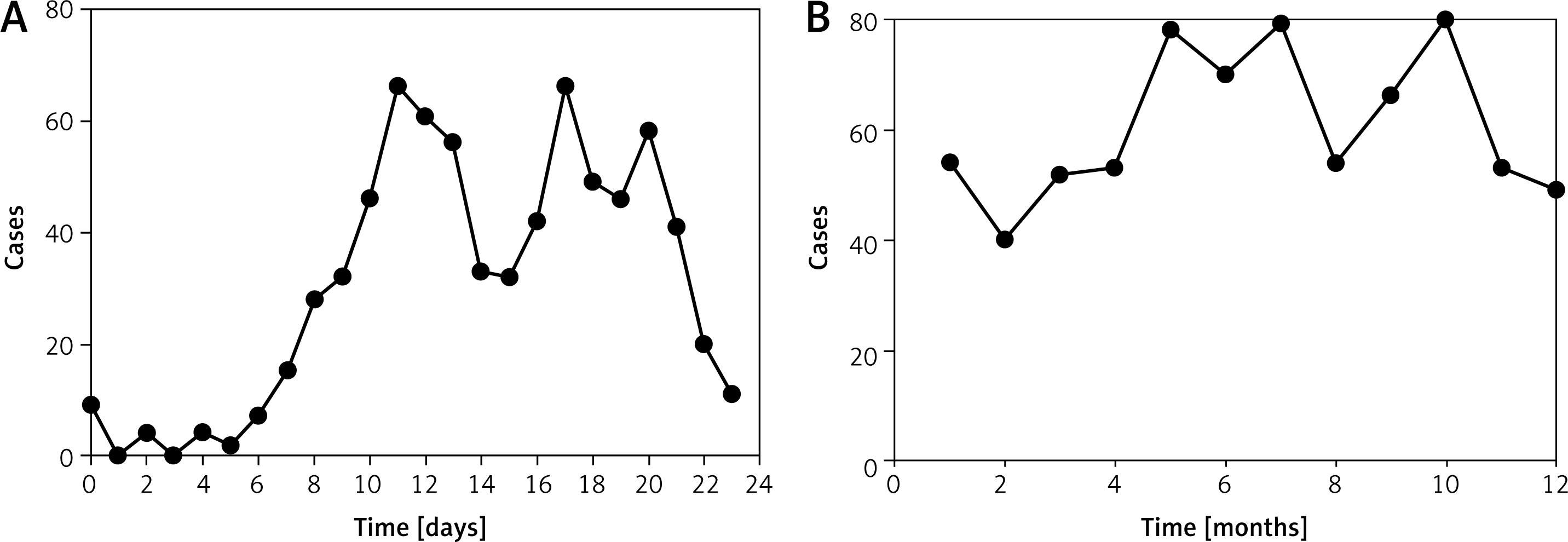
By residence, 501 (42.3%) children were from rural areas, 253 (21.4%) from urban areas, and 430 (36.3%) from suburban areas. Most injuries occurred at home (1093, 92.3%), whereas 91 (7.7%) occurred outdoors or in public places; outdoor/public burns were proportionally more frequent among rural children (Supplementary Table SIV). Daily burn peaks were observed around 12:00, 17:00, and 20:00 (Figure 1 A). Seasonally, cases clustered from May to October, with notable peaks in May, July, and October, and more cases in summer/autumn (693) than winter/spring (491) (Figure 1 B).
Postinjury management and outcomes
Only 293 (24.7%) children received appropriate cold therapy before admission. Burn ointment was used in 298 (25.2%), 40 (3.4%) received clearly inappropriate measures (e.g. toothpaste, soy sauce, honey, gasoline, or unidentified herbs), and 553 (46.7%) received no prehospital treatment. Reasonable prehospital care (cold therapy, burn ointment, or burn management at other hospitals) was associated with significantly better clinical outcomes than non-reasonable care (Z = 3.221, p < 0.01), and outcomes differed between reasonable and unreasonable measures (Z = 2.134, p < 0.05), whereas untreated and unreasonable groups did not differ significantly (Z = 1.202, p > 0.05) (Supplementary Table SV). After admission, 1026 (86.7%) patients received conservative wound care (including dressing changes and acellular dermis coverage), and 158 (13.3%) underwent surgical interventions (e.g. debridement, negative-pressure therapy, or skin grafting). Overall, mean hospitalisation was 12.9 days (median 10.0). Among second-degree burns, children treated with acellular dermis (n = 162) had shorter hospital stays than those treated with conventional dressing changes (10.78 ±4.00 vs. 13.26 ±6.71 days; t = 3.588, p = 0.0004) (Supplementary Table SVI).
Discussion
The prevention and management of paediatric burns remain global priorities, but epidemiological patterns and risk contexts vary across regions. Local surveillance is therefore essential to tailor prevention strategies and improve early care. In this retrospective investigation from Hangzhou, we summarise the clinical and contextual characteristics of hospitalised paediatric burns and propose practical prevention measures for families, schools, and the wider community.
To further clarify the importance of this study and its implications for future management of paediatric burn cases, it is essential to link our epidemiological findings to practical clinical and public health strategies. The core significance of this study lies in 3 aspects: first, it fills the gap in large-sample, long-term epidemiological data of paediatric burns in Hangzhou, providing a reliable evidence base for local healthcare authorities to formulate targeted prevention and control policies; second, it identifies key high-risk groups, aetiologies, and risk windows of paediatric burns in this region, enabling precise intervention to reduce injury incidence; third, it verifies the impact of prehospital first aid and clinical treatment methods on patient outcomes, providing guidance for optimising clinical management and improving prognosis. These findings are not only applicable to Hangzhou but also provide a reference for other cities in eastern China with similar socioeconomic and living conditions.
Children aged 1–3 years constituted the largest proportion of burn inpatients, and boys outnumbered girls. This pattern is consistent with early-childhood developmental and behavioural features: toddlers rapidly expand mobility and curiosity but lack mature hazard recognition, increasing vulnerability to hot liquids and household heat sources. Boys may show more exploratory and risk-taking behaviours, raising exposure to hazards such as heaters, sockets, and fireworks. A similar male predominance has been reported elsewhere [5–9]. With increasing age, improved cognition and experience likely reduce preventable household exposures, contributing to fewer cases in older children.
Injury patterns were characterised by multi-site involvement, most commonly affecting the upper limbs and trunk, with burn size typically 5–15% TBSA and depth mainly shallow II° to deep II° with mixed components. The predominance of moderate burns aligns with prior epidemiological reports [10]. This distribution probably reflects common scald mechanisms: children reach for containers on tables or countertops, sustaining initial upper-limb contact followed by downward flow onto the chest, neck, or abdomen. Given thinner paediatric skin and regional differences in skin thickness, similar exposures may result in deeper or mixed-depth injuries. Prevention should therefore prioritise limiting toddlers’ access to hot liquids and unstable containers, particularly to reduce functionally and cosmetically significant scarring on the upper limbs, neck, and chest.
Hydrothermal scalds were overwhelmingly dominant in Hangzhou, followed by flame burns, while electrical and chemical burns were uncommon. This pattern is consistent with domestic exposure: hot water, soup, and oil are frequently present during cooking, and dining and can be accessed by toddlers. Spills may occur when children pull, reach, or knock over thermoses, bowls, or hotpots. Other scenarios included hot water bottle leakage in winter and exposure to hot bathwater. Flame injuries were linked to candles or alcohol ignition, gas explosions, and fireworks; electrical burns were associated with unsafe household installations; and chemical burns often involved lime or strong cleaning agents stored at home. Most burns occurred at home, with fewer cases outdoors or in public settings, kindergartens, and other locations. We also observed a higher proportion of cases from urban and suburban areas than rural areas, differing from some prior findings [11], and potentially reflecting differences in local development, urbanisation, caregiving patterns, and health-care access that influence both exposure and hospitalisation.
Temporal patterns highlighted preventable risk windows. Daily peaks occurred around 12:00 and 17:00 (meal preparation/mealtimes) and around 20:00 (bathing). Seasonally, injuries clustered from May to October, with peaks in May, July, and October. Warmer months may increase exposed skin area due to lighter clothing, and high temperatures may elevate gas-related risks; winter heating-related burns were less prominent, possibly reflecting improved living conditions and safer practices.
A key concern was the low rate of appropriate cold-water first aid (24.7%). Some caregivers used ineffective or harmful substances such as soy sauce, sesame oil, toothpaste, honey, charcoal powder, plant ash, or unidentified herbs, which may complicate wound care. Although the proportion of inappropriate measures was lower than reported elsewhere [12], nearly half of children received no prehospital care, indicating persistent gaps in first-aid knowledge. Importantly, reasonable prehospital management was associated with better outcomes, supporting strengthened community education on immediate burn first aid.
Most wounds were managed conservatively with dressing changes or acellular dermis coverage, consistent with prior studies [13, 14]. Early acellular dermis use for II° paediatric burns was associated with shorter hospitalisation than routine dressing changes, possibly by reducing exudation, providing barrier protection, and supporting re-epithelialisation. For deeper injuries, early debridement with negative-pressure therapy followed by grafting remains a rational approach.
Building on the above findings, this study provides targeted, multi-level preventive strategies that address the specific epidemiological characteristics of paediatric burns in Hangzhou, which is critical for reducing the incidence and burden of this injury – consistent with the “preventive strategies” highlighted in the manuscript title. These strategies should be implemented through coordinated efforts across families, schools, medical institutions, and the wider community, with each level focusing on key risk factors identified in our study:
At the family level, targeted interventions should focus on children aged 1–3 years (the high-risk group, accounting for 63.1% of cases). Caregivers should be educated to strengthen supervision during high-risk time windows (12:00, 17:00, and 20:00, corresponding to mealtimes and bathing time). Specific measures include keeping hot liquids (hot water, soup, oil) out of children’s reach, installing anti-scald devices on water heaters to control water temperature (≤ 49oC is recommended), avoiding leaving children alone in the kitchen or bathroom, and using anti-scald tableware and thermoses to prevent spills. For winter heating and summer cooling, caregivers should check heating equipment (e.g., hot water bags) for leaks and ensure that cooling appliances (e.g., air conditioners, electric fans) are used safely to avoid accidental contact burns.
At the school level, age-appropriate safety education should be integrated into daily teaching, especially for children aged 4–14 years, for whom flame burns increase with age. For younger children (4–6 years), simple safety awareness training (e.g. through animations, picture books) can help them recognise hot objects and avoid dangerous behaviours. For older children (7–14 years), more in-depth education on fire safety (e.g. safe use of gas, avoiding fireworks, and handling electrical appliances) and basic burn first aid should be provided to reduce flame and electric burns, which are more common in this age group.
At the community and public health level, health management departments should carry out regular public education campaigns, focusing on burn first aid and prevention knowledge. Given that only 24.7% of children received appropriate prehospital cold therapy, community training should emphasise the correct method of cold therapy (cool running water irrigation for 15–20 min) and warn against inappropriate measures (e.g. toothpaste, soy sauce, herbs), which can exacerbate wound damage. For rural and suburban areas where outdoor/public burns are more frequent, targeted outreach programs should be implemented to improve caregiving awareness and first-aid capabilities. Additionally, public facilities (e.g. kindergartens, parks) should be equipped with first-aid kits containing burn dressings, and staff should be trained in basic burn management.
At the medical institution level, clinicians should integrate epidemiological findings into clinical practice to optimise management protocols. For second-degree burns, early application of acellular dermis (which our study found shortens hospitalization by 2.48 days on average) should be promoted as a routine intervention to improve outcomes and reduce medical costs. Moreover, medical institutions should establish long-term follow-up systems for burn patients to monitor medium- and long-term outcomes (e.g. scarring, functional impairment), which were not evaluated in this study, and provide timely rehabilitation guidance to reduce disability rates.
Beyond preventive strategies, this study also provides clear implications for the future management of paediatric burn cases, guiding clinical practice, public health policies, and research directions. In clinical management, the findings emphasise the importance of standardised prehospital first aid and personalised treatment based on age and burn characteristics. For example, younger children (1–3 years) with hot liquid scalds often present with multi-site, moderate burns, so clinicians should prioritise wound care and infection prevention to avoid scar contracture; older children with flame burns may require more aggressive surgical intervention (e.g. debridement, skin grafting) due to deeper burn depths, and psychological support should also be provided to address trauma.
In terms of public health policy, the study data can inform the development of regional burn prevention and control plans. For instance, targeted resource allocation to high-risk groups (1–3 years old) and high-risk seasons (May–October) can improve the efficiency of public health interventions. Additionally, the study highlights the need for a multi-sectoral collaboration mechanism involving health, education, and civil affairs departments to integrate burn prevention into public health services, forming a comprehensive prevention and management system.
For future research, this study identifies several key directions to address its limitations and further improve paediatric burn management. First, multi-centre studies including outpatient cases should be conducted to avoid selection bias and obtain a more comprehensive understanding of paediatric burn epidemiology in Hangzhou. Second, multivariate analysis models should be established to control for confounders (e.g. age, burn depth) and clarify the independent impact of prehospital care and treatment methods on outcomes. Third, long-term follow-up studies are needed to evaluate the long-term physical and psychological impact of burns on children, providing evidence for more comprehensive rehabilitation strategies. Finally, comparative studies with other regions can help identify regional differences in paediatric burn characteristics and promote the sharing of effective prevention and management experiences.
In conclusion, this retrospective analysis of paediatric burn inpatients in Hangzhou over a 5-year period highlights distinct epidemiological characteristics and identifies critical targets for prevention and clinical management. Burn injuries predominantly affected young children, particularly toddlers, reflecting age-related behavioural vulnerability and limited hazard awareness. Most cases involved multiple anatomical sites and were characterised by moderate severity, with scalds from hot liquids occurring primarily in domestic settings. Temporal clustering around mealtimes, bathing periods, and warmer months further underscores the role of daily caregiving routines and environmental factors in injury risk. Prehospital burn first aid was frequently inadequate, and appropriate early management was associated with improved clinical outcomes, emphasising the importance of caregiver education. In addition, early application of acellular dermis in second-degree burns was associated with faster wound recovery and shorter hospitalisation, supporting its clinical value in paediatric burn care. Collectively, these findings indicate that effective prevention of paediatric burns requires a coordinated, multi-level approach integrating enhanced family supervision of young children, strengthened burn safety and first-aid education in schools and communities – particularly in rural areas – and the promotion of standardised prehospital and in-hospital treatment strategies. Such measures are essential for reducing the incidence, severity, and long-term burden of paediatric burn injuries.
This study has several limitations that should be acknowledged when interpreting the results. First, it is a single-centre retrospective study conducted at a tertiary children’s hospital in Hangzhou, which may limit the generalisability of the findings to other regions or healthcare settings in China, especially primary hospitals or community clinics. Second, the study only included hospitalised paediatric burn patients, leading to inherent selection bias. Mild burn cases (e.g. < 5% TBSA, superficial II° burns) managed on an outpatient basis or treated at home were not captured, which may underestimate the overall incidence of paediatric burns in Hangzhou and skew the epidemiological profile; for example, the proportion of mild injuries, specific aetiologies of minor burns, and prehospital management patterns of non-hospitalised cases were not reflected. Third, as a retrospective analysis, the study relied on medical record data, which may have unavoidable information biases (e.g. incomplete documentation of prehospital care details or injury circumstances). Future studies should address these limitations by conducting multi-centre investigations involving primary hospitals, community clinics, and emergency departments to include both hospitalised and outpatient cases, thereby providing a more comprehensive and representative picture of paediatric burns in the region. Additionally, prospective studies with detailed follow-up could further explore long-term outcomes (e.g. scar formation, functional recovery, psychological impact) and the effectiveness of targeted preventive interventions.