
Introduction
The first laboratory confirmed case of SARS-CoV-2 in Poland was announced on March 4th, 2020 [1]. On March 10th the mode of SARS-CoV-2 transmission in Poland was officially declared by the World Health Organization as having shifted from imported cases only to local transmission [2]. In order to limit viral transmission, Polish authorities initiated lockdown type measures in mid-March. An official epidemic was declared on March 20th [3]. According to the Main Sanitary Inspectorate, meeting the suspect case definition for COVID-19 is an indication for laboratory testing in order to confirm or exclude a diagnosis. A suspected COVID-19 case is defined as a person meeting one of the following criteria [4]:
– presenting group A clinical symptoms (cough, fever, shortness of breath) without other confirmed etiology and staying or returning from an area with local or low-frequency COVID-19 transmission within the last 14 days or having close contact with a confirmed COVID-19 case,
– being hospitalized with symptoms of severe respiratory infection without other confirmed etiology or presenting life or health threatening symptoms of respiratory failure.
A confirmed COVID-19 case is defined as a positive result of real-time reverse-transcriptase-polymerase-chain-reaction (RT-PCR) assay of nasal or pharyngeal swab specimens. Official case fatality rates in Poland initially included only deaths of confirmed COVID-19 cases (U07.1 according to the ICD-10). Since April 1st, in keeping with a report published by the National Institute of Public Health, fatalities that were clinically or epidemiologically diagnosed as COVID-19 (U07.2) were also considered as deaths due to COVID-19 [5].
The aim of this study was to analyze the basic COVID-19 epidemiological data on a regional level and to examine which indicators related to epidemiology, population characteristics and healthcare quality affect COVID-19 incidence, mortality and case fatality in Poland. The results may potentially help to better understand the epidemiology of COVID-19 and could be useful for policymakers to plan ahead in order to relieve the risk of overload of the healthcare system.
Material and methods
Poland is made up of 16 voivodeships, which represent the highest level of administrative subdivision. This division was used in the study to portray geographical variety within the country. The study was based on national data as of May 4th, 2020: epidemiological data (number of confirmed cases and deaths, number of performed tests, dates of the first confirmed case) from all 16 voivodeships have been retrieved from official coronavirus source data [6]; data on population, population density, proportion of urban population and proportion of population aged above 65 for each voivodeship were obtained from Statistics Poland reports [7]; indicators used to characterize voivodeships in terms of the healthcare system performance (healthcare performance index, health consumer index, effective financial management index) were derived from a report published by PricewaterhouseCoopers Poland [8]; the number of hospitals with isolation wards in each voivodeship were retrieved from the list of hospitals published by the Ministry of Health [9]; the number of beds in general hospitals per 10,000 population and the number of beds in infectious disease wards by voivodeships were obtained from Statistics Poland [10] and voivodeship office reports [11].
For each voivodeship morbidity indicator (incidence rate, i.e. COVID-19 cases per 10,000 population), death rate indicator (mortality rate, i.e. number of people who have died due to COVID-19 per 10,000 population), disease severity indicator (case fatality rate, i.e. proportion of deaths among patients with COVID-19) and DCI (daily cumulative index, defined as cumulative cases divided by the number of days between the first reported case and May 4th, 2020) were calculated.
Pearson’s correlation coefficient (PCC) and Spearman’s rank correlation coefficient (SRCC) were used to examine the links between incidence, mortality, case fatality and various epidemiological indicators. PCC is typically used to evaluate the linear relationship between normally distributed variables. For nonnormally distributed data, ordinal data or data with relevant outliers, SRCC is more appropriate. Both correlation coefficients range in value from –1 to +1. When it equals 1 the two variables perfectly correlate in a positive way, when it equals 0 they are independent from one another, and when it equals –1 they perfectly correlate in a negative way (anti-correlation). The strength of association between the two variables is considered very strong if the coefficient ranges from 0.8 to 1, moderate (or strong) if it ranges from 0.5 to 0.8, weak (or fair) if it ranges from 0.2 to 0.5, and very weak (or poor) when it is less than 0.2.
Results
As of May 4th, nearly 10,000 people in a million have been tested, a total of 14,006 cases have been confirmed, and 697 persons have died due to COVID-19 in Poland. The mean age of death among women was 77.6 (the youngest registered deceased patient was 27 years old) and among men it was 72.3 (the youngest registered deceased patient was 18 years old). The overall incidence rate was 3.65 per 10,000 population, mortality rate 0.18 per 10,000 population and case fatality rate 5%.
COVID-19 incidence, mortality and case fatality rates and number of performed tests for individual voivodeships, grouped by population density, are presented in Table I. Individual voivodeships and corresponding DCI are presented in Figure 1. The highest incidence per 10,000 population was observed in Lower Silesian and Silesian voivodeships (5.94 and 5.86, respectively) and the lowest in Lubusz voivodeship (0.89). The highest number of deaths per 10,000 population was reported in the Masovian voivodeship (0.39), whereas Lubusz voivodeship registered no deaths due to COVID-19. The case fatality rate reached the highest values in Masovian (8%), Opole (7%) and Subcarpathian (7%) voivodeships. The highest DCI value was recorded in Silesian (51.08), followed by Masovian (47.28), Lower Silesian (29.2) and Greater Poland (26.82) voivodeships (Figure 1).
Table I
Incidence, mortality and case fatality rates and number of performed tests for individual voivodeships, grouped by population density
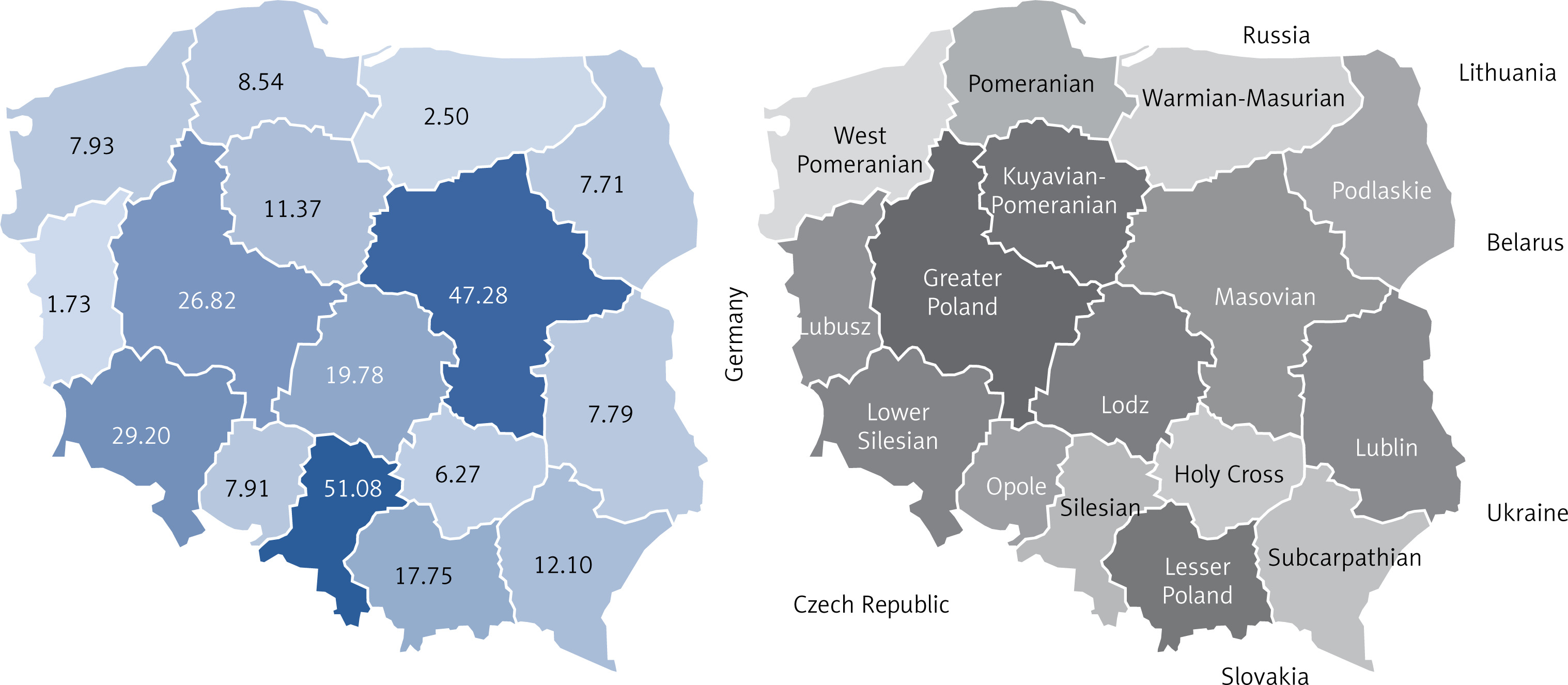
Table II and Figures 2 and 3 present the results of correlation analyses. All three disease indicators (i.e. incidence rate, mortality rate, case fatality rate) were positively correlated with DCI and negatively correlated with the number of hospital beds in infectious disease wards per 10,000 population. Additionally, both incidence and mortality rates were positively correlated with population density and number of cases per COVID-19 designated hospital. Only incidence was found to have a strong positive correlation with the proportion of people aged above 65. Among variables analyzed in our study, incidence rate, case fatality rate and age > 65 were distributed normally, which justified the use of PCC. However, in most cases the assumptions of PCC were not met and SRCC was more applicable.
Table II
Correlations between incidence, mortality, case fatality rates and selected epidemiological indicators
Figure 2
Associations between disease indicators and daily cumulative index (DCI) of COVID-19. A – Correlation between mortality rate and DCI. B – Correlation between case fatality rate and DCI
PCC – Pearson’s correlation coefficient, SRCC – Spearman’s rank correlation coefficient.
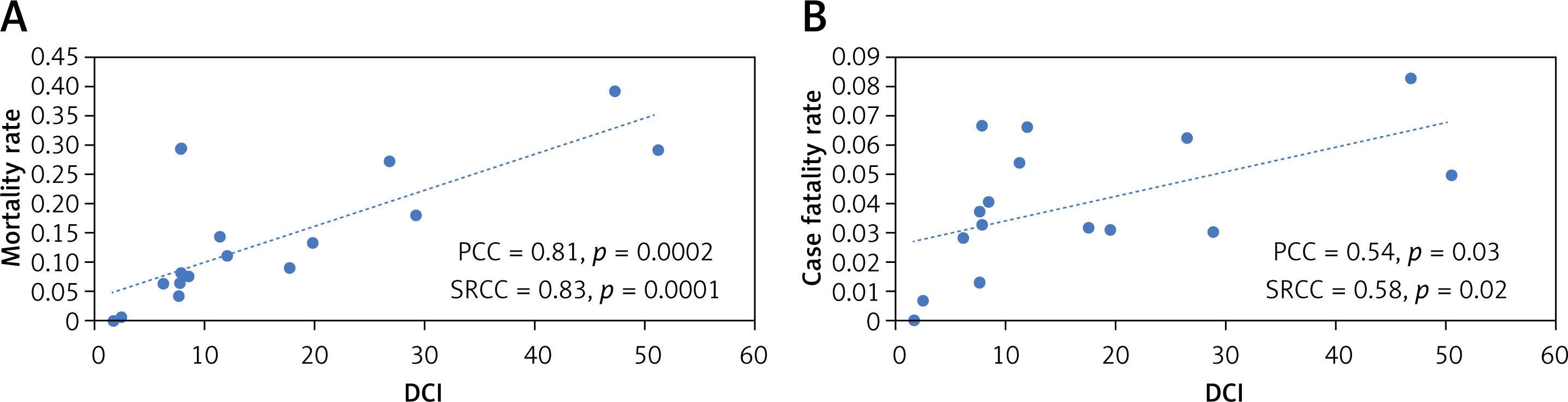
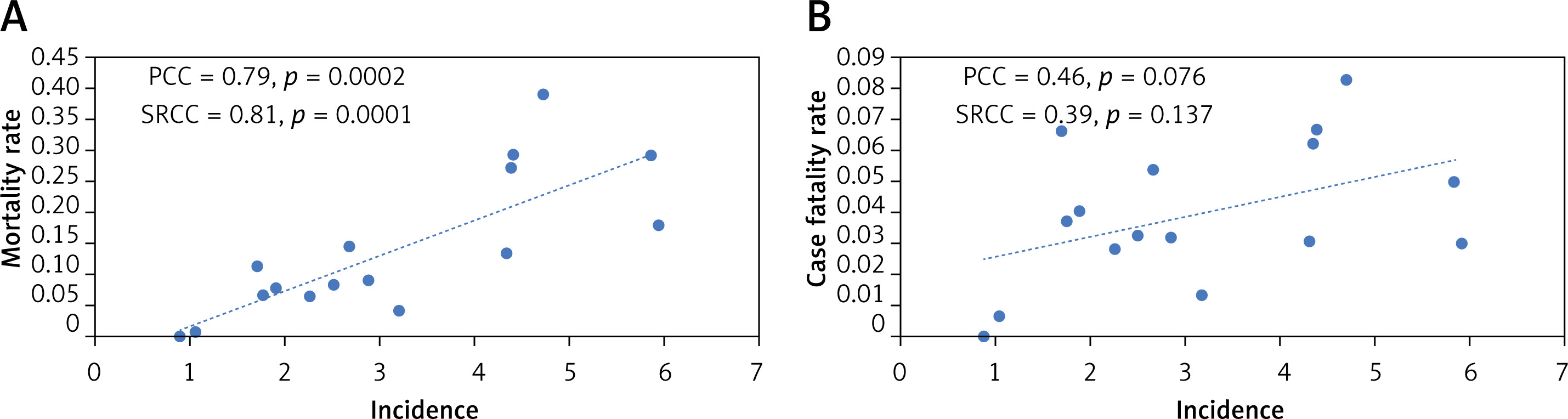
Figure 3
Associations between disease indicators and incidence of COVID-19. A – Correlation between mortality rate and incidence. B – Correlation between case fatality rate and incidence
PCC – Pearson’s correlation coefficient, SRCC – Spearman’s rank correlation coefficient.
No statistically significant correlation was observed between disease indicators and number of beds in general hospitals, proportion of urban population, proportion of medical staff per 100,000 population, number of performed tests per 10,000 population and healthcare system performance indexes.
Discussion
Although the epidemic outbreak occurred almost simultaneously in individual voivodeships and national lockdown measures were enforced at the same time, our study revealed considerable regional differences in terms of COVID-19 incidence, mortality and case fatality rates. Findings of our correlation analyses indicate that such disparities might be associated with factors related to epidemiology, population characteristics and healthcare resource availability.
The fact that both incidence and mortality were positively correlated with population density is in line with our knowledge about the spread of the virus and confirms that measures to reduce viral transmission, focusing on social distancing in particular, are reasonable [12–16]. The positive correlation between COVID-19 incidence and the proportion of the population aged above 65 suggests that older adults are more likely to get infected, which has been observed in other countries as well [17–22].
All three disease indicators were found to have a strong positive correlation with DCI. High DCI, i.e. a rapid increase in the number of cases, may speed up the viral transmission in a given population and in consequence the growth of incidence rates. Furthermore, the positive correlation between DCI and both mortality and case fatality suggests that DCI could be considered as an indirect indicator of healthcare burden, as a sudden increase in the number of cases causes higher consumption of medical resources and may lead to worse patient outcomes.
Similarly, the negative correlation between number of hospital beds in infectious disease wards per 10,000 population and both mortality and case fatality indicates an association between deaths due to COVID-19 and healthcare resources availability. At the same time, however, a negative correlation between incidence and the number of hospital beds in infectious diseases wards per 10,000 population was observed. This finding may be explained by the fact that mortality is strongly positively correlated with incidence and parameters correlated with mortality are correlated with incidence as well. The lack of association between all three disease indicators and healthcare performance indexes indicates that these indicators are not specific enough to measure the quality of healthcare in the context of COVID-19.
The current pandemic is a novel and rapidly emerging worldwide crisis. To date only a few studies have aimed to examine the potential relationship between COVID-19 and parameters related to epidemiology and availability of healthcare resources. Our results are in line with a previously published study which associates higher number of infections with higher mortality [23]. Our analysis also reveals that both mortality and case fatality are positively correlated with DCI (Figure 2) [24]. However, contrary to mortality, no positive correlation between case fatality and incidence was found (Figure 3). Acknowledging the potential association of mortality and healthcare resource availability [25] implies that DCI could be used as an indirect indicator of healthcare burden. Still, it is important to stress that mortality due to COVID-19 may be strongly affected by patients’ underlying conditions and critical care capacity (number of mechanical ventilators, intensive care units, critical care providers) [17, 26].
The major strength of our study was analyzing individual regions within one country. This ensured that similar epidemic outbreak dates occurred and equal lockdown and diagnostic measures were enforced. However, the results of our study should be interpreted cautiously, bearing in mind limitations attributable to the quality of data available at the time of analysis. The testing strategy is central to obtain actual data on the number of COVID-19 cases, and no country knows the number of infected people, as it depends on how widespread the testing is. Furthermore, due to the lack of current regional data on the number of intensive care units, mechanical ventilators, critical care providers and their potential impact on analyzed COVID-19 indicators, future studies covering these parameters might be valuable.
In conclusion, additionally to incidence rate, DCI may be used as an indicator of increased COVID-19 mortality and case fatality rates. Mortality and case fatality rates may be affected by healthcare resource availability, and it is therefore crucial to develop strategies aimed at preventing the capacities of the healthcare system being exceeded. According to our results, social distancing and common testing play a vital role in reducing SARS-CoV-2 transmission. The results of our analysis might help political leaders and health authorities to allocate enough medical resources to manage the present pandemic, as well as future pandemics.