Introduction
Lung cancer is one of the most deadly malignancies that can endanger a person’s life or health [1]. Many nations have seen lung cancer incidence and death rise during the last 50 years [2]. The American Cancer Society (ACS) projected 608,570 fatalities and 1,898,160 new cases in 2021 [3]. As a prominent radiological signal, lung nodules are used to diagnose lung cancer early. Diameter determines nodule malignancy [4]. Nodules in the pulmonary interstitium, which consists of the basement membrane, pulmonary capillary endothelium, alveolar epithelium, and perilymphatic and perivascular tissues, are typically small, spherical, and circumscribed [5, 6]. Lung nodules vary in size, shape, and kind [7]. Nodules can vary in size from less than 2 mm to 30 mm, and some are difficult to detect because of their complex circulatory connections in places with numerous vessels [8]. There are certain solid and sub-solid nodules (SSNs) with densities that are marginally greater than those of the parenchyma of the lung [9]. Solid nodules (SNs) are the most common nodules and comprise the core functioning lung tissues, while SSNs often represent early-stage lung cancers appearing as areas of partial ground-glass opacity. SSNs may be part-solid or pure ground-glass nodules [10]. These nodules do not obscure the bronchovascular structures, but their opacities are denser than those of the surrounding tissues [7].
Accurate nodule diameter measurements are essential for diagnosis since nodule size is correlated with malignancy. Several studies [5, 11, 12] offer valuable insights [13]. The End-Use Load and Consumer Assessment Program (ELCAP) database [3] reports a 1% malignancy risk for nodules under 5 mm, 24% for 6–10 mm, 33% for 11–20 mm, and 80% for 20+ mm [14]. However, measuring the diameters of extremely small nodules may result in errors. The therapy for cancer of the lung nodules is complicated. Almost 70% of individuals with lung cancer require radiation treatment; however, radiation-induced lung damage may reduce treatment rates and raise morbidity and death. Radiologists rely on computer-aided diagnostic (CAD) technologies to extract more information from nodules and enhance classification accuracy. CAD systems minimize observational errors, false-negative rates, and medical image interpretation and diagnostic second opinions [15, 16]. Numerous studies indicate that CAD systems improve image diagnosis, with lower inter-observer variance [17]. CAD systems can also quantify clinical decisions such as biopsy recommendations [18], facilitate diagnostic checks, minimize thoracotomies and false-positive biopsies [16, 19], and distinguish tumor malignancies [20, 21]. Clinical success has led to the introduction of CAD models for lung cancer diagnosis. Early diagnosis of lung nodules may improve survival using such devices. Current computed tomography (CT) CAD applications search for spherically distributed lung nodule-like pulmonary densities [15]. Thus, lung nodule screening by CT CAD has become a prominent area of research. Lung nodule detection initially was based on non-machine learning techniques [22–28]. Later, data-driven machine learning-based algorithms [29–34] were developed to delineate the ideal nodule border [35]. Deep learning (DL) inspired algorithms have recently attracted interest because of their precise predictions. Unlike traditional CAD systems, DL-based models can be optimized and applied to vast volumes of data [36]. DL using CNNs has improved pulmonary nodule diagnosis and treatment [37–40]. Three modules of DL are used to recognize, segment, and categorize lung nodules. Detection identifies the nodule, segmentation delineates its voxels, and classification determines whether it is benign or malignant [35].
Lung cancer often remains asymptomatic in its early stages, leading to delayed diagnoses. When symptoms appear, they frequently include shortness of breath, wheezing, hoarseness, chest pain, coughing up blood, and a persistent cough. Additional signs may involve recurrent respiratory infections, unexplained weight loss, and fatigue. Moreover, these symptoms might differ from person to person and can mimic those of other respiratory disorders [41].
Regarding mortality, lung cancer remains a leading cause of cancer-related deaths globally. For instance, in the United States, an estimated 124,730 lung cancer-related deaths are anticipated for 2025. The mortality rate is significantly higher in older populations, with three-quarters of lung cancer deaths occurring among those aged 65 and older. Increasing survival rates require early detection through screening programs, since lung cancer can often be identified at an advanced stage when there are few available treatment choices [41].
Previous studies have explored the detection approaches for pulmonary nodules [35, 36, 42–48] with various goals. The primary aim of this article is to provide a comprehensive review of deep learning (DL) methodologies employed for pulmonary nodule identification and classification in CT images. This study aims to explore the effectiveness of various DL models, including multi-view convolutional neural networks (CNNs) and 3D architectures, in improving diagnostic accuracy and efficiency in lung cancer screening. Furthermore, it aims to identify current challenges, such as data variability and the need for external validation, and suggest directions for future research to facilitate the integration of these advanced technologies into routine clinical practice. This study introduces a novel deep learning-based system using two 3D models for automated pulmonary nodule detection, aiming to enhance diagnostic accuracy and reduce false positives.
Nodule detection
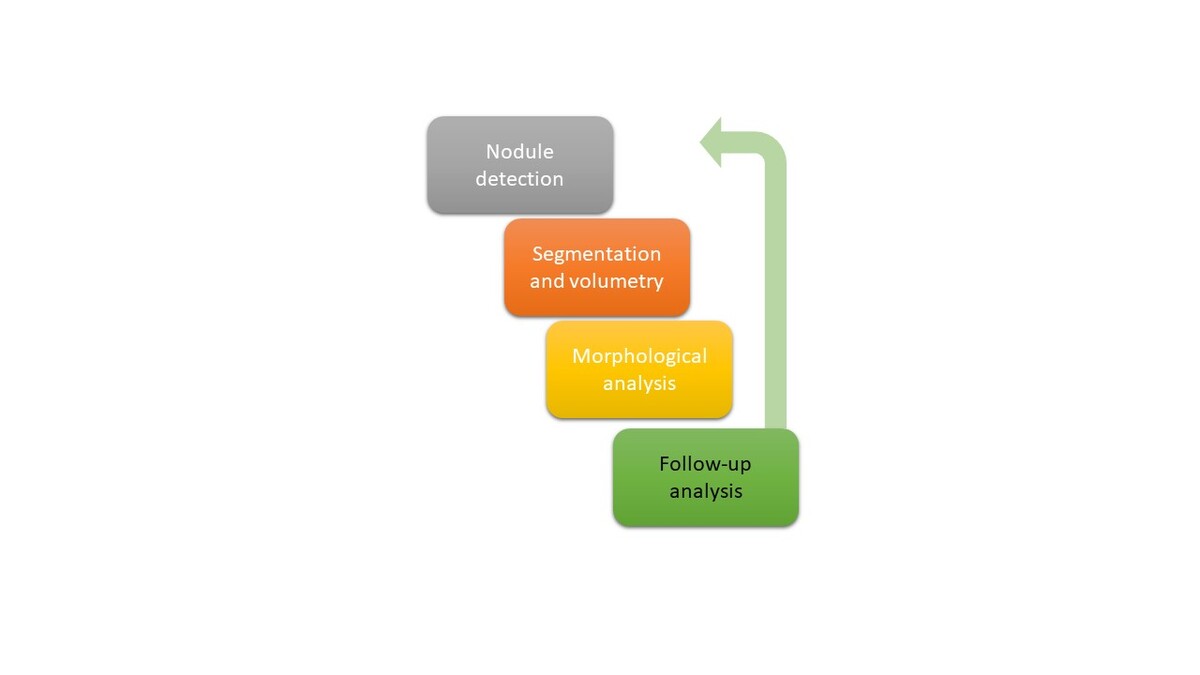
Identifying microscopic pulmonary nodules is challenging yet important for lung cancer diagnosis. Chest volumetric CT images exceed 9 million voxels. Five-mm lung nodules occupy 130 voxels, corresponding to about 1.4 × 10–5 of the lung volume [49]. Radiologists may be able to detect these nodules based on their shape, size, density, location, and closeness to adjacent structures. Early CT screening missed 8.9% of malignancies in the NLST CT screening arm [50]. The pathological analysis of biopsy samples is still the most reliable method for identifying and defining pulmonary nodules, even though imaging approaches are significant for their detection. Although having two observers simultaneously read a scan improves diagnostic sensitivity, performing it repeatedly is time-consuming and impracticable [51]. This emphasizes the significance of machine-learning technology to assist radiologists detect nodules, one of the most studied CAD applications that reduce the time needed to interpret scans [52]. Several studies have demonstrated that deep learning may improve nodule detection sensitivity. Figure 1 shows the steps in the lung nodule treatment route using AI.
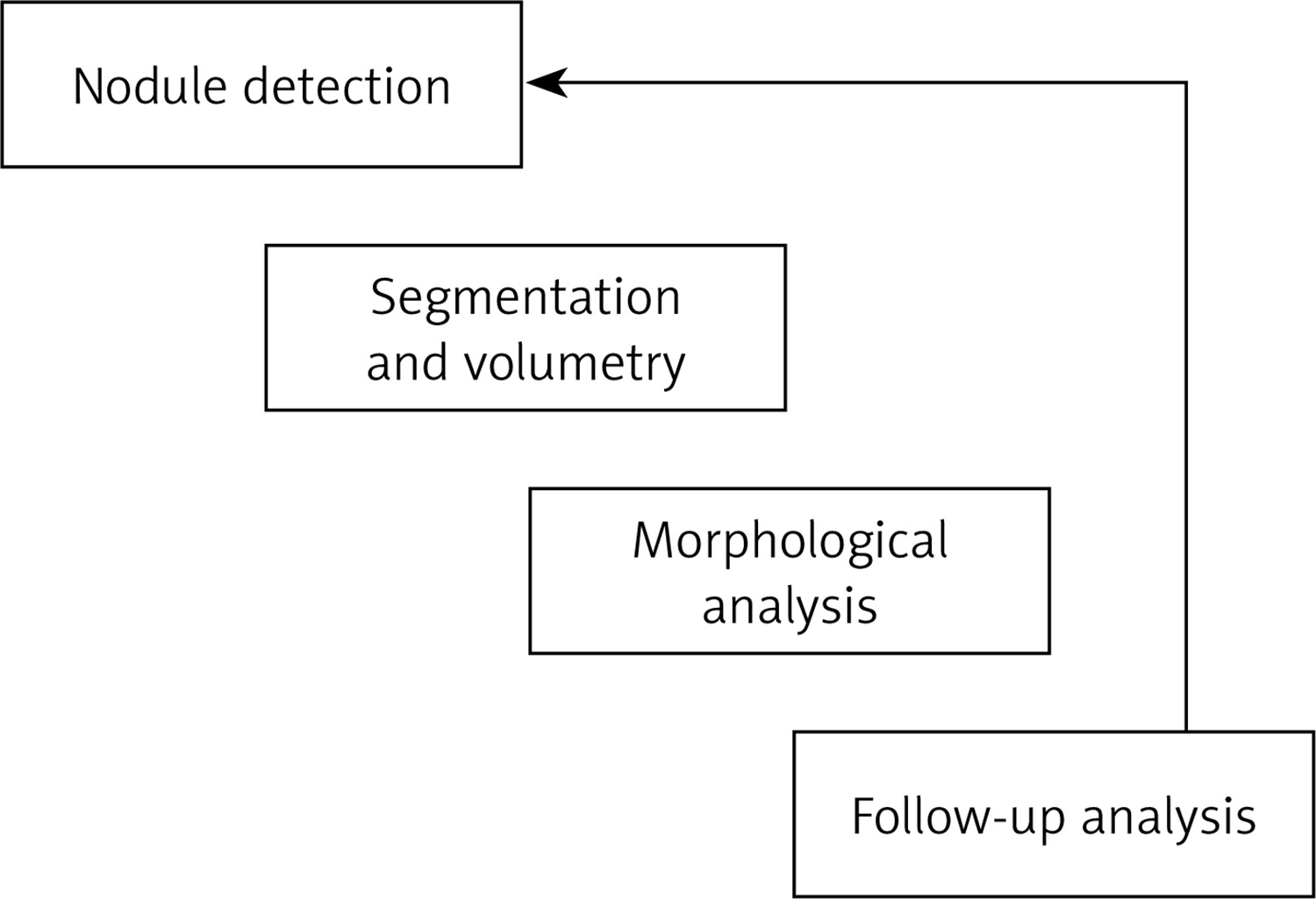
This CAD application has been extensively investigated and has been demonstrated to minimize scan interpretation time [52]. Various studies have reported that deep learning can enhance the sensitivity of nodule identification [53].
Nodule segmentation
Malignancy is strongly predicted by nodule size; in the NELSON trial, those with nodules < 100 mm3 had the same baseline cancer risk (0.5%) as those without nodules [54]. Traditional nodule size assessment involves manual 2D caliper measurement of the largest transverse diameter. Current screening studies and national and worldwide guidelines on nodule treatment have recommended evaluating volume rather than diameter because it is less susceptible to intra- and interobserver variability [55], better incorporates the three-dimensional (3D) character of a lung nodule [56], is more susceptible to size change, and detects malignancy sooner than 2D diameter measures [57]. Nodule segmentation is essential for volumetric measurements. Numerous CAD methods for nodule segmentation have been developed since the 1980s [44]. Detecting microscopic pulmonary nodules is challenging yet significant for lung cancer diagnosis. Chest volumetric CT images exceed 9 million voxels. Five-mm lung nodules occupy 130 voxels, corresponding to about 1.4 × 10–5 of the lung volume. These nodules may be detectable by radiologists depending on their shape, size, density, location, and proximity to other structures.16e18 Early CT screening missed 8.9% of malignancies in the NLST CT screening arm [58].
Subsolid nodules are more challenging to segment than solid lesions because there is less attenuation difference between the tumor and the surrounding parenchyma. It is also more challenging to distinguish the solid component of these very large nodules from nearby vessels. However, current research indicates that these problems can be addressed [59]. Multiple manual, semi-automatic, and automated volumetric analysis software programs have been reported in recent years. Although these software tools may produce slightly different size measurements, they provide reliable repeat measurements. The variance is larger in irregular and juxta-pleural nodules [60]. The British Thoracic Society’s pulmonary nodule management guidelines suggest reducing variability in nodule volumetry [61].
Research has demonstrated that deep learning can improve nodule segmentation. A single click can volumetrically segment 7,927 NLST nodules using a deep learning model. These parameters were used to evaluate the Brock University Cancer Prediction Model’s malignancy prediction accuracy. The AUC for volumetric analysis was 88.17, compared to 85.96 for NLST radiologists’ 2D measurements, demonstrating a 2.21% enhancement in predictive value. As CNN algorithms implicitly segment nodules, deep learning may eliminate nodule segmentation [38, 62].
The issue of detecting lung nodules in daily clinical practice
Lung cancer is the leading cause of cancer death worldwide [63]. Symptoms typically appear after cancer has spread, and therefore late diagnosis is usual [64]. To detect malignancies early, the US, China, and Korea have implemented nationwide lung tumor screening programs. High-risk individuals (older smokers) are invited for a low-dose CT lung scan in a screening program [65]. Lung cancer may manifest as a “nodule” or spot. Trials show that low-dose CT screening reduces lung carcinoma mortality [66, 67], but Europe and other nations have been sluggish in embracing it. Therefore, early-stage lung cancer is often identified incidentally through nodules observed in CT scans carried out for unrelated medical reasons [68, 69]. It can be challenging to detect lung nodules. CT scans are highly heterogeneous and not optimized to identify lung cancer due to the growing diversity of scanning methods and patients [49]. Nodule detection and treatment will become more crucial because radiologists’ workload has increased significantly over the past 15 years, primarily due to the demand for CT imaging [70].
Artificial intelligence for radiological support
AI software may help radiologists find lung lesions in CT images. The use of AI software as an auxiliary reader enhances radiologists’ reading time, management recommendation uniformity, and detection sensitivity [71–74]. A few studies have explored AI solutions in non-screening environments. The generalization performance of the AI software was tested using a multi-center study approach to expand this research area and address three common issues. Second, we used five qualified thoracic radiologists rather than one or two to establish the reference standard, because nodule detection varies greatly. Third, and perhaps most importantly, we examined whether an AI system could identify the important nodules using reliable nodule-level malignancy labels. Research on AI has either looked at all nodules (regardless of malignancy) or scan-level cancer detection. Therefore, our effort aims to connect AI investigations for nodule identification and lung malignancy.
Connecting the gap between nodule detection and lung cancer AI studies
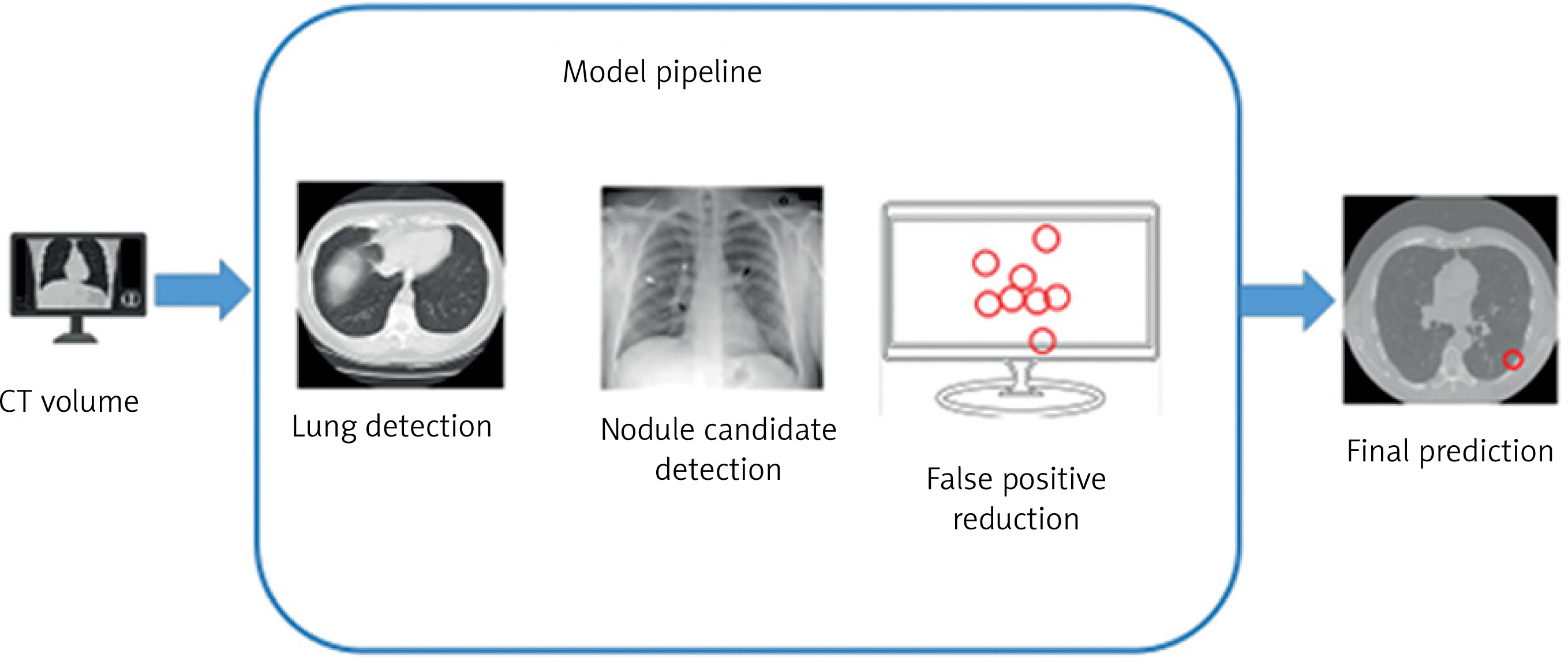
The DL-based technique was retrospectively tested for identifying actionable benign nodules (requiring follow-up), minor lung cancers, and metastases in CT images from two Dutch hospitals’ typical clinical contexts. Moreover, the nodule detection method locates a specific lung region slice by slice using a CT scan. Five-slice overlapping CT volumes yield nodule candidates. Finally, nine slices from a 3D area around each nodule candidate are inspected for nodules. Nodules from lung arteries and other structures can be promptly identified in CT scans using the 2.5D identification method (Figure 2).
DL strategies for detecting lung cancer
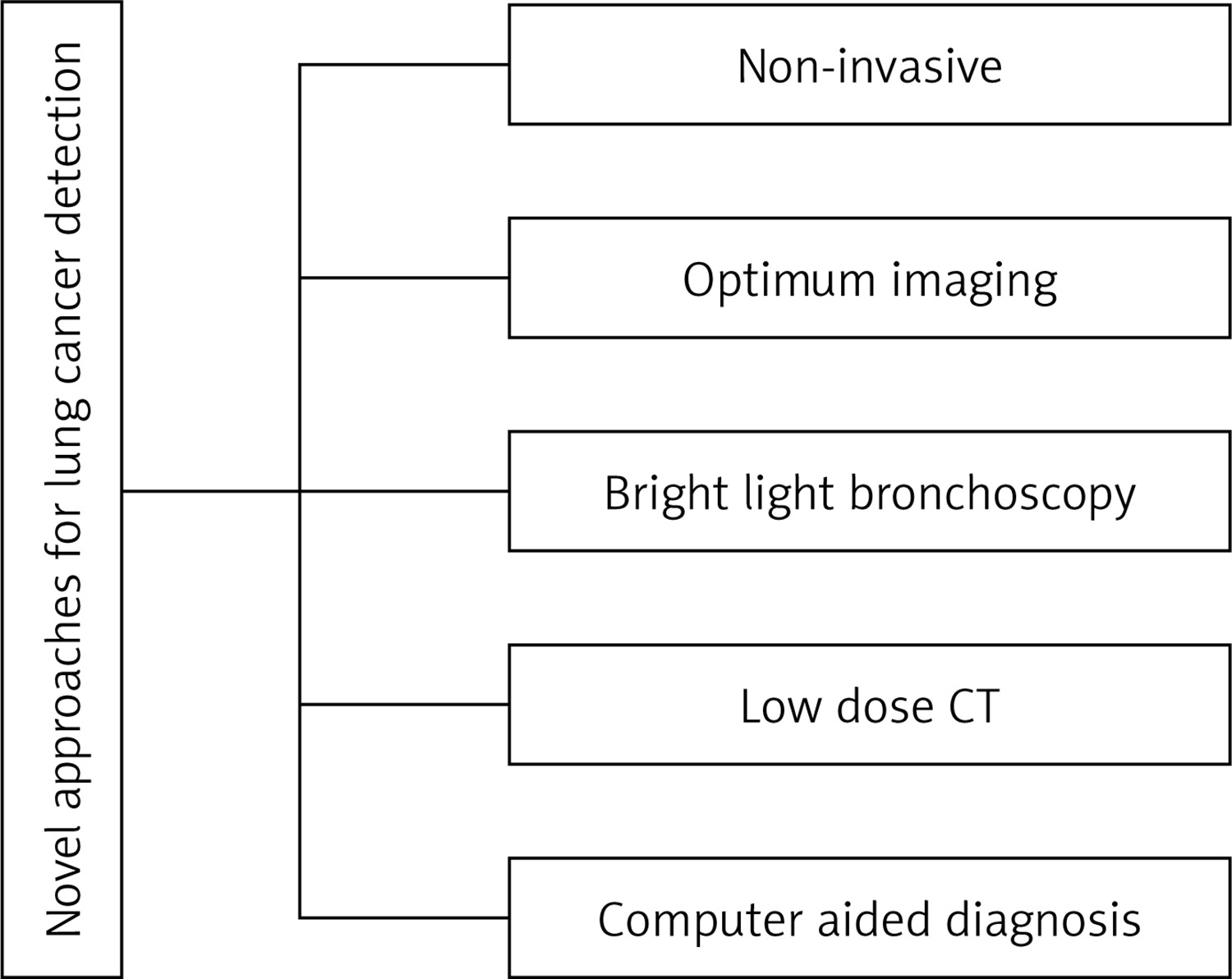
Automation has the potential to assist in diagnosing various diseases through CAD [75]. This method employs software to identify, predict, and classify symptoms, assisting in identifying the presence and severity of a disease. This study reviews CAD approaches for lung CT nodule detection. CT scans can identify nodules of lung cancer, especially large ones in the advanced stages [76]. The nodules need to be identified early because they are often very small before a lung tumor the size of a golf ball grows. Figure 3 shows that manually distinguishing and segmenting nodules is challenging.
CNNs are highly effective for image classification. Their architecture is inspired by the human visual system. CNN filters assess a small portion of the image by simulating neurons with receptive zones. Deeper layers of these neurons may learn and detect more complicated hierarchical patterns due to their larger receptive fields. CNNs can be thought of as a collection of sliding windows with small neural networks spread around the image [77].
CNNs can learn patterns regardless of location due to their location invariance. The filter can learn image designs using sliding windows. Since CNNs are hierarchical, they can automatically identify more abstract patterns [78]. Boundaries and structures may be occupied by the initial layers, followed by forms in the intermediate layers and overall object shapes in the higher layers. CNNs are capable of analyzing 3D images rather than slices from CT scans. A sliding cube, instead of a movable pane, can be employed to develop 3D CNNs for feature extraction at each stage [79].
Computer-assisted lung cancer detection using CT images
CT-based lung tumor identification and detection employing DL algorithms has been the subject of numerous studies. Healthy and unhealthy CT scans have different image attenuation patterns. To separate the lungs from the nearby tissues, numerical, grey-level thresholding, and shape-based methods have been employed [80]. Brown and coworkers introduced an automatic, knowledge-based chest segmentation approach [81]. This approach requires organ volume, relative location, shape, and X-ray attenuation. To extract useful CT image data, Brown et al. developed a knowledge-based automatic segmentation method [82]. They automatically created indirect quantitative values of single lung activities that routine pulmonary function tests cannot. Hu et al. created a completely automated pulmonary segmentation approach from 3D lung X-ray images [83]. The technique was tested employing 3D CT information sets from 8 healthy individuals. Computer and human analysis showed a 0.8-pixel root mean square difference. Lung segmentation was fully automated using a pixel-value threshold based on slices, together with two sets of categorization criteria that incorporate size, circularity, and position data [84]. They achieved 94.0% segmentation precision with 2969 thick slice images and 97.6% with 1161 thin slice images based on 101 CT cases [85]. The lung volume was segmented and visualized using anisotropic filtering and wavelet transform-based interpolation. The robustness and application of the approach were demonstrated using single-detector CT scans, which showed improvements in volume overlap and volume difference percentages.
Swierczynski et al. devised a level-set-based segmentation approach that combined traditional segmentation with active dense displaced field prediction [86]. The developed approach outperformed methods that performed registration and segmentation independently. A substitutional level set technique for CT scan lung nodule segmentation was developed using a global lung nodule form model [87]. Nodule kind or position did not affect the proposed technique. Moreover, to improve lung nodule detection, a parameter-free segmentation method was developed that focused on juxtapleural lesions [88]. LIDC’s 403 juxtapleural nodules indicated a 92.6% re-inclusion rate. Zhang et al. [89] developed an automated lung segmentation approach and a global optimum hybrid geometric active contour model. Incorporating global region and edge information increased algorithm performance in places with narrow bands or weak boundaries. Furthermore, in another study [90], a sphere was placed within the segmented lung target and deformed in response to forces applied to the lung boundaries. The system was tested on 40 CT images, achieving an average F-measure of 99.22%.
Researchers have been examining CNNs’ durability in computer vision for 10 years. Multiple CNN-based methods have been reported for medical and natural image processing. Several methods have been proposed using AI and CT images for the detection of lung cancer [91]. Lung nodule classification was carried out using a three-dimensional CNN with three modules. This technique outperformed manual evaluation with 84.4% sensitivity. Nasser and Naser [92] used an ANN to diagnose lung cancer with 96.67% accuracy. Cifci [93] reported that DL, combined with Instantaneously Trained Neural Networks (DITNN) and Increased Profuse Clustering (IPCT), improved lung image quality and lung cancer detection, achieving an accuracy of 98.42%. Moreover, in another study [94], a double convolutional deep neural network (CDNN) and a regular CDNN were employed to identify lung nodules, achieving an accuracy of 0.909 and 0.872.
Wang et al. [95] developed a CAD system with low false negative and positive rates as well as high nodule detection precision. In another approach [96], the deep model achieved 95.41% sensitivity in lung image detection using inception-v3 transfer learning instead of randomized initialization. Finally, a multi-group patch-based learning system was reported, revealing an 80.06% sensitivity with 4.7 false positives per scan or a 94% sensitivity with 15.1 false positives per scan. Furthermore, a dense convolutional binary-tree network (DenseBTNet) was developed which showed high parameter effectiveness and extracted features at several scales [97]. Li et al. found that early detection reduces the death rate from lung cancer [98]. They developed a DL-CAD system that could recognize and classify lung nodules under 3 mm and estimate their malignancy risk. The system demonstrated an accuracy of 86.2% in sensitivity testing carried out on the LIDC-IDRI and NLST datasets.
Similarly, a deep 3D residual CNN was employed to reduce false positives for automated lung nodule diagnosis in CT images [99]. A spatial pooling and cropping (SPC) layer gathered multi-level contextual information, and their 27-layer network achieved 98.3% sensitivity using the LUNA-16 dataset. Teramoto et al. [100] developed a deep convolutional neural network (DCNN) comprising convolutional, completely linked, and pooling layers to automatically classify lung cancer. DCNN training employed 76 cancer cases and achieved 71% classification accuracy. In a study, a 3D convolutional neural network was employed for volumetric CT-based computer-aided lung nodule identification [101]. They used the LUNA16 dataset to test their model, which had 3D convolutional, max-pooling, completely linked, and softmax layers. Their findings suggested that 3D CNNs significantly improved detection accuracy, achieving a sensitivity of 94.4%.
Similarly, DL algorithms were employed to predict lung cancer survival, determine EGFR mutation status, and classify subtypes based on CT scans [102, 103]. Several studies have explored the use of DL algorithms for pulmonary nodule segmentation and categorization in CT imaging [35]. A 3D deep-learning model and low-dose chest CT images were employed to develop an end-to-end lung tumor detection system [104]. Shao et al. [105] employed DL algorithms to screen mobile low-dose CT images for lung tumors in resource-constrained areas. Moreover, a model [106] was designed that identified the EGFR mutations and expression of PD-L1 status in non-small-cell lung tumors using CT images. A study [107] provided an in-depth analysis of different DL approaches for identifying and diagnosing lung nodules in CT scans.
Deep neural networks were employed to segment lung CT images [11] in addition to categorization. Lakshmanaprabu et al. [108] determined that the DL model achieved the highest classification accuracy of 96.3% for lung tumors using CT data. The application of DL models in chest radiography and lung tumor identification using CT images was investigated by Lee et al. [109], who observed that these models may increase clinical efficacy and accuracy. To identify lung cancer, Bhatia et al. [110] proposed a DL technique with 93.55% sensitivity and 91.5% specificity. Moreover, another model [111] was designed using DL on CT scans to detect expression of PD-L1 in non-small cell lung tumors and predict immune checkpoint suppressor responses for a smaller nodule. Hu et al. [112] proposed a DL system for lung cancer stage extraction from CT data with an F1 score of 0.848. A machine learning strategy that can detect preinvasive, benign, and invasive lung nodules on 1-mm-thick CT scans was proposed [74, 113] to demonstrate the efficacy of a DL-enhanced CAD system in recognizing them. Deep learning was also used to predict lung cancer with an accuracy of 87.63% [114].
Rajasekar et al. [115] developed six DL models (CNN GD, CNN, Inception V3, VGG-16, Resnet-50, and VGG-19) that efficiently identified lung tumors by employing CT scans and histopathology images. CNN-GD outperformed other models in precision, F-score, sensitivity, accuracy, and specificity, achieving 97.86%, 96.39%, 96.79%, and 97.40%, respectively. Wankhade et al. [116] presented a 3D-CNN and recurrent neural network (RNN) approach that achieved 95% accuracy in classifying malignant lung nodules. Efficiency can be improved using big-data analytics and cascade classifiers. Abunajm et al. [117] proposed a CNN-based model for primary lung cancer prediction and recognition using CT scan imaging, distinguishing malignant, benign, and normal cases. Initial lung cancer detection improves survival and timing of therapy. The model reduced false positives and achieved an accuracy of 99.45%.
In a study [118], radiomics and deep learning were employed for lung cancer identification and treatment. Experts explain that radiomics enables the quantification of medical images, enhancing cancer diagnosis and prognosis. Deep learning systems can be used for data analysis. Deep learning was used to forecast the risk of cardiovascular disorders from low-dose CT scans used to test for lung tumors [119]. The researchers used a massive cardiovascular risk dataset to train a DL system to predict heart disease risk from lung CT images. Moreover, in a study [120], dense clustering and DL were combined to immediately train neural networks to improve lung tumor detection from CT images. They demonstrated the efficiency of their lung nodule detection approach by comparing it with existing lung cancer detection methods. A newly developed DCNN was assessed on a large dataset of CT scans to detect and classify lung nodules in 3D CT images [121]. Zhao et al. [122] proposed a weighted discriminatory extreme learning machine for electronic nasal system lung tumor detection. They were able to differentiate between the two groups by using an electronic nasal device to examine breath samples from lung tumor patients and healthy controls. Chen et al. [123] developed a multimodality attention-guided 3D detection system for non-small cell lung cancer using 18 F-FDG PET/CT images. The accuracy of PET/CT lung cancer detection was improved by the researchers using deep learning algorithms, which could help in early diagnosis and treatment. Table I lists the uses, advantages, and drawbacks of lung imaging technologies, while Table II lists the models studied between 2018 and 2022.
Table I
Uses, advantages, and drawbacks of lung imaging technologies
Table II
Studied models for lung image segmentation and nodule detection (2018–2022)
Developing techniques for detecting lung cancer
Lung cancer is a highly fatal form of cancer. Identifying cases is challenging because they typically manifest in the terminal stage. However, mortality can be reduced by early disease detection and treatment. CT imaging is a reliable diagnostic method since it can detect all predicted and unexpected lung tumor nodules [124]. However, medical practitioners and radiologists may misinterpret CT scan intensity and anatomical structure, making malignant cell identification difficult [125]. Therefore, computer-aided diagnostic methods are being employed by radiologists and physicians to diagnose cancer [126]. Numerous technologies have been established, and research into lung cancer detection is still ongoing. Certain systems need to be improved to achieve 100% detection accuracy.
Lung cancer may be cured with the correct medications, early detection, and a precise etiology. Early lung tumor detection is therefore essential, especially when screening high-risk populations such as oil field workers, smokers, individuals exposed to fumes, and others, for whom new biomarkers are required. The precision of the diagnosis also affects the best course of treatment for lung cancer. Therefore, finding sensitive and precise biomarkers is essential for primary diagnosis. Low-dose CT is used in recent lung cancer screening methods. Compared to cases without screening, the NELSON trial [127] reported that this screening method provides 85% sensitivity and 99% specificity. A recent study [128] demonstrated a false-positive rate of less than 81%, necessitating further imaging or testing due to the high incidence.
To explain the lung cancer stage and screening schedule, a brief overview is given here. SCLC and NSCLC are the primary lung cancer subtypes. SCLCs are central tumors that form airway submucosal perihilar masses. Histological studies show that basal bronchial epithelial neuroendocrine cells cause this malignancy. Most cells in this scenario are spindle-shaped, rounded, or small with minimal granular chromatin, cytoplasm, and necrosis [129]. Unlike pure and mixed NSCLC, which may include liver, brain, and bone metastases [130], SCLC has limited or extensive phases [131].
This malignancy [132] may be characterized by metastases to the brain, liver, and bones, with its stages classified as either confined or extensive [133]. Limited SCLC includes the ipsilateral mediastinum, mediastinal, or supraclavicular lymph nodes at a single radiation site. It is a supraclavicular lymph node if it is located on the same side as the cancerous chest. However, broad SCLC can extend to the second lung lobe, bone marrow, and lymph nodes. Chest radiography produces more detailed images than a chest CT scan, but it is less sensitive. With these characteristics, a computer-aided diagnostic (CAD) model for chest radiographs would improve detection sensitivity while preserving low false-positive (FP) rates [134].
Cytological analysis of sputum, especially many samples, may help diagnose lung cancer and find a core tumor in the larger bronchi. Sputum samples seldom include very small adenocarcinomas under 2 cm that originate from airway branches such as the bronchi, bronchioles, and alveoli [135]. As cigarette exposure has influenced the incidence of squamous cell carcinomas and adenocarcinomas, this information has become more and more crucial. Several screening investigations found that sputum cytology had a 20–30% sensitivity for primary lung tumors. Early studies found that the quantity and form of cells in deeper airways can alter pre-malignant detection [136]. It was reported [137] that regular sputum cytology is neither sensitive nor precise for lung cancer screening. White light bronchoscopy is the most common histological lung cancer diagnosis procedure. Bronchoscopy can detect pre-malignant lesions. Tissue biopsy remains the standard method for detecting cancer in general hospitals. The size of lung tissue biopsy specimens is crucial for the histopathological detection of lung cancer subtypes. The first biopsy needs to confirm the diagnosis to avoid recurrent operations that may cause difficulties and delay therapy. Fiber-optic bronchoscopy, image-guided trans-thoracic needle aspiration, endobronchial ultrasound, pleural fluid examination (thoracentesis), mediastinoscopy, thoracoscopy, and operations are employed to diagnose lung tumors. These methods are expensive, error-prone, and need numerous samples [138].
Spiral CT images enhance the performance of peripheral small tumor diagnosis. However, these images show significantly reduced sensitivity for central tumor identification (primarily squamous cell carcinoma) than peripheral tumors [139]. In the National Lung Screening Trial (NLST) using low-dose CT (LDCT), 96% of positive screenings were false positives, with over 40% of participants experiencing at least one positive result [66]. The high frequency of false positive screening results in expensive and intrusive therapies for smokers without malignancies. For diagnosis, screening for lung cancer with low-cost, non-invasive methods is essential.
CNN, a kind of DL, has advanced radiology [140, 141]. In chest radiography, DL-based models have also demonstrated success in detecting masses and nodules, with mean false positives per image (mFPIs) of 0.02–0.34 and sensitivities of 0.51–0.84. Moreover, radiologists were able to identify nodules more accurately with CAD models than with screening procedures without them. It can be difficult for radiologists to identify and differentiate between benign and malignant nodules [142, 143]. Radiologists also need to monitor nodule form and marginal features as typical anatomical structures mimic healthy nodules. Even the most skilled radiologists may make diagnostic mistakes due to circumstances rather than their own shortcomings [144, 145]. The main DL methods for lesion identification are segmentation and detection. The detection approach labels an area, unlike the segmentation method, which labels pixels. Segmentation provides more exact pixel labels than detection. Pixel-level lesion size categorization enhances clinical diagnosis. Lesion size and form variations are easier to monitor using pixel-level classification because the shape may affect detection. As part of the evaluation of management effectiveness, it also displays lesion size and long and short diameters [146].
Investigation gaps and limitations
Better survival rates depend on the primary detection of lung tumors; however, this is difficult because of factors such as heterogeneity, low contrast fluctuations, and visual similarities between benign and malignant nodules in CT images [147]. Identifying lung nodules with medical imaging is challenging owing to the complex architecture and time-consuming acquisition of labeled samples [148]. Deep learning algorithms are frequently compared to traditional CAD systems that employ manually created features, even though they can automatically identify features in lung nodule CT scans [149]. There is limited research on employing CNNs to analyze EBUS images, which makes it challenging to distinguish benign from potentially malignant tumors [150]. While some studies have employed CT scans to predict mortality risks in NSCLC patients, they have not identified primary-stage lung or lobe-related malignancies [151]. The mechanism by which CNNs predict nodule malignancy and the influence of area or contextual information on their output remains unclear [152]. Computer-assisted lung disease detection is crucial owing to noise signals affecting cancer image quality during acquisition [153]. Training DCNNs is challenging because of the various kinds of lung nodules and limited availability of positive samples in many datasets [154].
Segmentation process
Image segmentation shows organ or structural outlines. DL techniques improve semantic segmentation, which makes them useful for medical diagnosis. This method evaluates the sizes and shapes of organs or lesions using MRI or CT scans [155, 156]. Many researchers have proposed automated segmentation methods. However, pre-processing typically involves edge detection and the application of mathematical filters. Further, deep machine learning extracted complex traits. Creating and extracting hand-crafted features was the biggest challenge for such a system, limiting deployment. Medical researchers segmented images using 2D, 2.5D, and 3D CNN [157, 158]. A CT scan can easily separate the lung and non-lung areas in a typical lung due to their different image attenuation. Early lung segmentation approaches encompassed numerical methods, gray-level thresholding, and shape-based approaches to distinguish lung regions from non-lung areas.
Various CNN-based methods have been established for both medical and natural image processing. Early research focused on lung nodule segmentation [156]. In a study [159], a basic CNN model for lung segmentation was developed employing a clustering algorithm-based training dataset. The k-means clustering technique divided CT slices into two groups using the image patch’s mean and minimum intensity. Cross-shaped confirmation, volume intersection, linked component analysis, and patch expansion were used to construct the dataset. The CNN design comprised a single layer of convolution with 6 kernels, one maximally pooled layer, and two fully connected layers. An eightfold cross-validation method was employed to evaluate CNN models trained on the produced datasets. The researchers designed automated lung segmentation techniques to denoise lung CT images without affecting lung outlines using an image decomposition-based filtering technique [160]. The lungs were segmented using wavelet transformation and morphological methods. Finally, contour correction was used to smooth the lung outlines during segmentation refinement.
Khanna et al. [161] developed a false-positive-reducing Residual U-Net for lung CT segmentation. The more complex network with residual units in the suggested model makes it easier to extract lung segmentation information. Performance comparisons of U-Net and E-Net were also performed [162]. These models partition pulmonary fibrosis parenchyma quickly and effectively.
Furthermore, a U-Net-based lung segmentation approach was developed that had an expanding route for high-level information and a contracting route for low-level information [163]. The model achieved a Dice coefficient of 0.9502 in the experiments. Mask R-CNN and supervised and unsupervised machine learning were used to produce another automated lung segmentation method [164]. The benchmarked methods were slower and less precise than our approach, which achieved a segmentation precision of 97.68% and was completed in 11.2 s.
Setio et al. presented a multi-view convolution network to recognize lung nodules using discriminative features of training data [165]. The three-nodule potential detectors target solid, subsolid, and large nodules. The proposed method integrates several 2-D ConvNet streams with a reliable classification algorithm. The LIDC-IDRI dataset shows four false positives per scan and 85.4% detection sensitivity. Similarly, a 3D CNN was trained using LIDC dataset volumes of interest to autonomously identify lung nodules [166]. Furthermore, a 3D CNN was employed to quickly produce the volume score map in a single run by generating a 3D fully convolutional network (FCN). Candidate regions of interest were quickly generated by the discriminating CNN using the FCN-based architecture.
In another study [167], DL and shape-driven level sets were employed to produce another automatic lung nodule segmentation system. The invention of shape-driven level sets was the first step toward fine segmentation. Similarly, the model was automatically initialized by the level sets using seed points from the deep network’s coarse segmentation.
Conclusion and recommendations
This study highlights the significant progress made in pulmonary nodule diagnosis and segmentation through deep learning (DL) techniques. The study addresses issues including heterogeneity, low contrast variations, and the visual similarities between benign and malignant formations in CT imaging by using CNNs and transfers learning techniques to improve the accuracy of lung nodule identification and delineation. The integration of DL approaches has shown superiority over traditional computer-aided diagnostic (CAD) systems that rely on hand-crafted features, offering a more robust and automated solution for early lung cancer detection.
For future research, a deeper exploration of DL model interpretability is crucial to clarify the specific features and contextual information these networks use to distinguish between benign and malignant nodules. Furthermore, expanding the diversity and size of annotated datasets will enhance the generalizability and performance of DL models. Collaborative efforts between multidisciplinary teams, including radiologists, data scientists, and clinicians, are essential to translate these technological advancements into clinical practice, ultimately improving patient outcomes through early and accurate lung cancer diagnosis.