Introduction
One of the most important prognostic factors in patients after myocardial infarction (MI) is reduced left ventricular ejection fraction (LVEF). In the last three decades, LVEF has been used as the main diagnostic and prognostic parameter in the management of patients after MI and heart failure (HF) [1–3]. Heart failure has been classified in the 2016 guidelines of the European Society of Cardiology (ESC) as HF with preserved ejection fraction (EF) (HFpEF, EF ≥ 50%), HF with mid-range EF (HFmrEF, EF 40–49%), and HF with reduced EF (HFrEF, EF < 40%) [3].
One of the factors that seems to affect the long-term prognosis in patients with reduced LVEF is atrial fibrillation (AF) [4, 5]. In patients with ST-segment elevation myocardial infarction (STEMI), the frequency of AF reaches up to 21% [6]. In a study of post-MI patients with LVEF ≤ 40%, the 12-month incidence of AF was 32% [7]. In the OPTIMAAL (Optima Trial in Myocardial Infarction with the Angiotensin II Antagonist Losartan) trial, patients after MI with signs of left ventricular dysfunction and concomitant AF had an increased risk of death and stroke during the follow-up period [8]. Atrial fibrillation is the most common arrhythmia in HF. It increases the risk of thromboembolic complications, particularly the risk of stroke. It may worsen cardiac function [3]. Therefore, patients with AF require special management and treatment. Notwithstanding, most of the papers focus mainly on the role of reduced LVEF on the long-term prognosis in patients after MI, and they often pass over concomitant AF and its influence on long-term results in this group of patients [2, 9, 10].
Due to data limitation, the present study aimed to compare the clinical characteristics, treatment, and 12-month outcomes of patients after MI with EF < 40% and with or without AF, who survived index hospitalization and were enrolled in the Polish Registry of Acute Coronary Syndromes (PL-ACS).
Material and methods
Registry design
We used the data from the PL-ACS. The registry was established in 2003 and gathers detailed data on in-hospital management, the treatment, and the results of patients with acute coronary syndrome (ACS). The registry was a joint initiative of the Silesian Center for Heart Diseases in Zabrze and the Polish Ministry of Health. The design, methods, and logistic aspects of the PL-ACS registry have been described previously [11].
According to the protocol, all admitted patients with suspected ACS were screened for eligibility to enter the registry, though they were not enrolled until ACS had been confirmed. Patient data were collected by skilled physicians and entered directly using a dedicated web-based form.
Data collection
The follow-up data regarding the rates of all-cause mortality, recurrent hospitalization, and stroke were available for a limited number of patients. The information was obtained from the Silesian Cardiovascular Database (SILCARD) and the Acute Myocardial Infarction in Poland (AMI-PL) registry. The SILCARD database was based on the agreement between the Silesian Center for Heart Diseases and the Regional Department of National Health Fund in Katowice to conduct a comprehensive analysis of patients with cardiovascular diseases in the Silesian Province [12]. The AMI-PL gathers administrative data from all MI hospitalizations recorded by the national healthcare provider. The detailed design and logistic aspects of SILCARD and AMI-PL databases have been presented previously [13].
Endpoints and definitions
Major adverse cardiovascular events (MACEs) involved death, non-fatal MI, rehospitalization due to HF, and stroke within the 12-month follow-up. Death was considered as all-cause death. Non-fatal MI was defined as an ischemic event that met the ESC/American College of Cardiology criteria for MI [14]. Stroke was recognized as an acute neurological deficit lasting > 24 h and affecting the possibility to perform daily activities or resulting in death. The analysis included only the patients with a confirmed diagnosis of STEMI and non-ST elevation myocardial infarction (NSTEMI). STEMI was defined as the presence of: 1) a typical anginal pain and/or ischemic symptoms at rest lasting more than 20 min; 2) ST-segment elevation consistent with myocardial infarction of 2 mm or higher in the adjacent chest leads and/or ST-segment elevation of 1 mm or higher in 2 or more standard leads, or a new left bundle branch block; and 3) positive markers for cardiac necrosis. NSTEMI was defined as: 1) the absence of ST-segment elevation as defined above and 2) positive markers for cardiac necrosis.
Study objectives
The study population involved patients after MI with EF < 40% divided into the two groups: with or without previous or on-admission AF. The analysis included only those patients who survived index hospitalization. We compared the differences in clinical characteristics, treatment strategy, as well as in-hospital and 12-month outcomes, including the number of MACEs. Finally, we identified the independent predictors of death and MACE incidence.
Statistical analysis
All continuous variables had a skewed distribution and were presented as medians and interquartile ranges [IQR]. Categorical variables were presented as percentages. We used the χ2 and Mann-Whitney U tests as appropriate to test for differences between the patients with and without AF. A p-value of < 0.05 was considered significant. Kaplan-Maier cumulative survival curves were constructed and the difference in mortality and MACE in the 12-month follow-up was compared using the log-rank test. To identify the independent predictors of 12-month outcomes for the final group of 10,231 patients, a logistic regression analysis was performed.
Forty-six variables with potentially predictive significance were used in the multivariate analysis, including baseline characteristics, comorbidities, hospital treatment, in-hospital events, and the treatment administered at admission. The stepwise forward regression was performed and only variables with a p-value of less than 0.05 were included. Analyses were performed using the Statistica 13.3 software (StatSoft).
Results
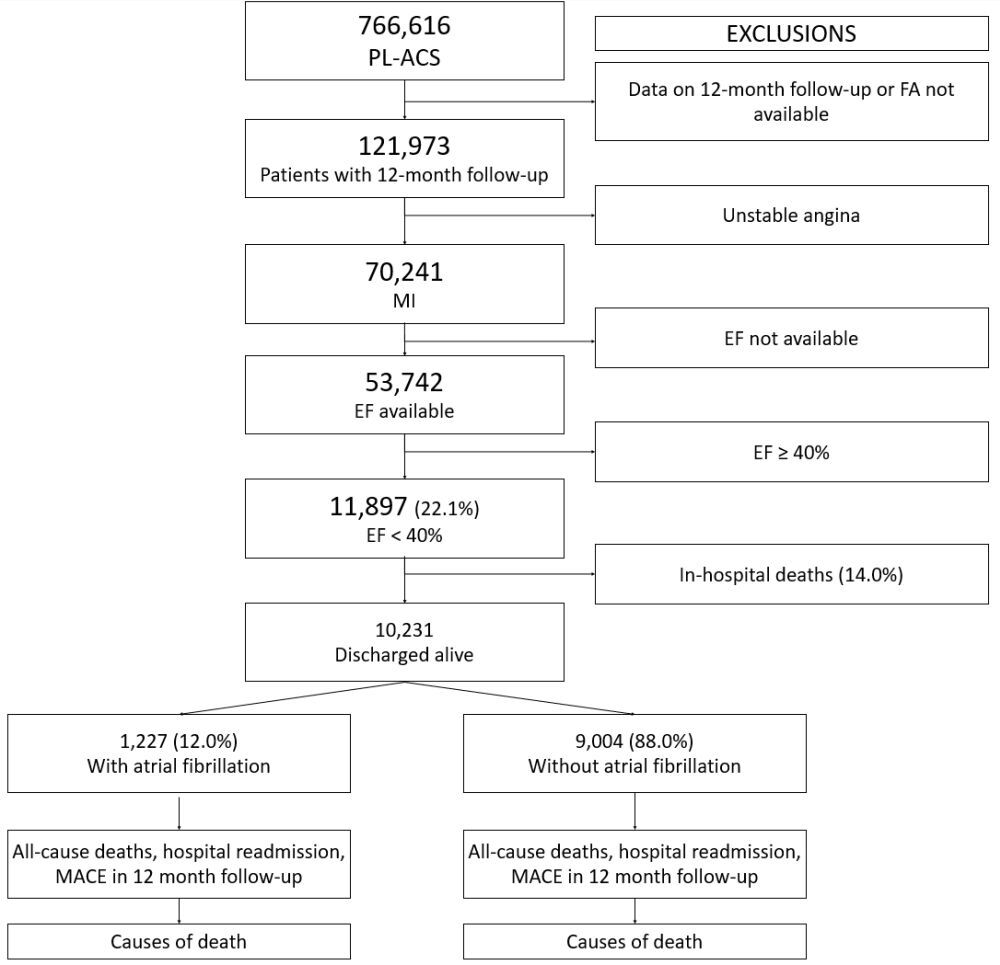
From October 2003 to April 2019, a total of 766,616 consecutive patients with ACS were enrolled in the ongoing, prospective PL-ACS registry. The final analysis involved 10,222 surviving patients with MI whose EF had been assessed during index hospitalization and the 12-month follow-up data. The study population flowchart is presented in Figure 1. The baseline demographic and clinical characteristics of patients with AF compared to those without AF are listed in Table I. The patients with AF were older and had a greater prevalence of previous MI, percutaneous coronary intervention (PCI), coronary artery bypass graft surgery, and HF hospitalization. Pulmonary edema, cardiogenic shock, and NSTEMI on admission were more frequent in the AF patients. LVEF was also significantly lower in the AF group. The in-hospital data are presented in Table II. In patients with AF, coronary angiography and PCI were performed less frequently. Patients from this group were more often diagnosed with multivessel coronary artery disease (p < 0.001).
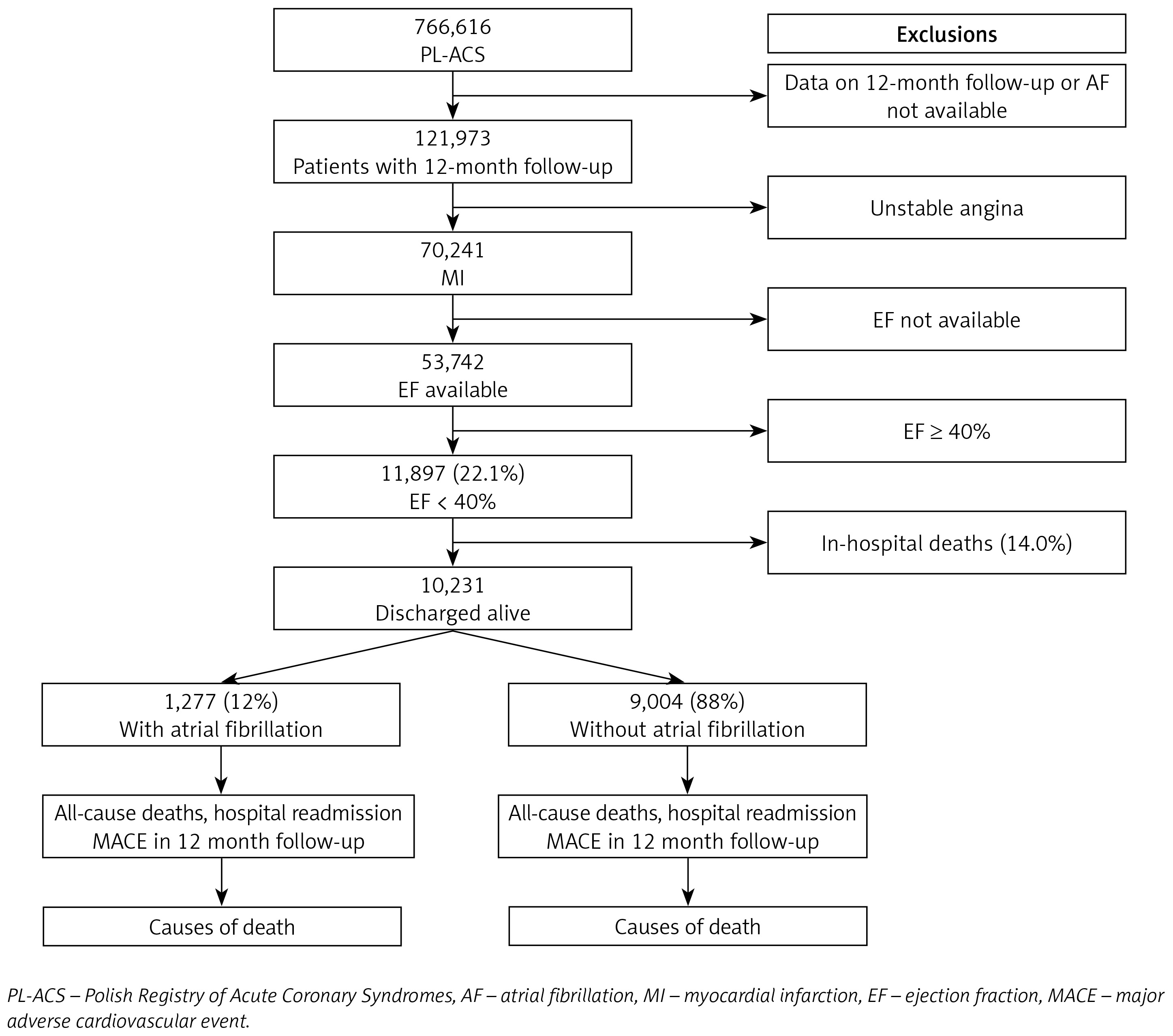
Table I
Baseline demographic and clinical characteristics of the study groups
| Variables | AF (n = 1,227) | Non-AF (n = 8,995) | P-value |
|---|---|---|---|
| Age [years], med [IQR] | 73.7 [13.1] | 68.3 [16.4] | < 0.001 |
| Males, n (%) | 802 (65.4) | 6250 (69.4) | 0.003 |
| Previous MI, n (%) | 453 (37.3) | 2907 (32.4) | 0.0007 |
| Previous PCI, n (%) | 335 (27.5) | 2116 (23.6) | 0.002 |
| Previous CABG, n/n (%) | 141/1217 (11.6) | 802/8986 (8.9) | 0.003 |
| Previous stroke, n (%) | 105 (10.6) | 397 (5.7) | < 0.001 |
| Previous PM, n (%) | 17/248 (6.9) | 19/933 (2.0) | 0.0002 Y |
| Previous ICD, n (%) | 25/248 (10.1) | 28/933 (3.0) | < 0.001 Y |
| Previous CRT-D, n (%) | 4/248 (1.6) | 19/932 (2.0) | 0.86 Y |
| Previous HF hospitalization, n (%) | 343 (34.6) | 1367 (19.7) | < 0.001 |
| CHA2DS2-VASc score, med [IQR] | 4 [2] | 3 [3] | < 0.0001 |
| CHA2DS2-VASc score (mean, SD) | 4.2 (1.6) | 3.5 (1.5) | < 0.0001 |
| Smoking, n/n (%) | 585/1179 (49.6) | 5000/8828 (56.6) | < 0.001 |
| Hypercholesterolemia, n (%) | 619 (51.5) | 4584 (51.5) | 0.99 |
| Diabetes mellitus, n (%) | 507 (41.8) | 3153 (35.6) | < 0.001 |
| Hypertension, n (%) | 967 (79.1) | 6637 (74.1) | 0.0002 |
| Previous CKD, n (%) | 263 (26.7) | 917 (13.2) | < 0.001 |
| COPD, n/n (%) | 91//984 (9.2) | 433/6927 (6.3) | 0.0004 |
| Cancer, n/n (%) | 11/243 (4.5) | 40/913 (4.4) | 0.94 Y |
| Clinical presentation | |||
| OHCA, n (%) | 19 (1.5) | 225 (2.5) | 0.051 Y |
| NYHA I, n (%) | 251 (27.3) | 2106 (34.7) | < 0.001 |
| NYHA II, n (%) | 496 (54.0) | 3148 (51.8) | < 0.001 |
| NYHA III, n (%) | 154 (16.8) | 740 (12.2) | < 0.001 |
| NYHA IV, n (%) | 18 (2.0) | 77 (1.3) | < 0.001 |
| Pulmonary edema, n (%) | 116 (9.5) | 636 (7.1) | < 0.001 |
| Cardiogenic shock, n (%) | 50 (4.1) | 389 (4.3) | < 0.001 |
| STEMI, n (%) | 303 (24.7) | 4083 (45.4) | < 0.001 |
| SR (admission ECG), n (%) | 100 (8.1) | 8560 (95.5) | < 0.001 |
| AF (admission ECG), n (%) | 1115 (90.9) | 405 (4.5) | < 0.001 |
| LVEF, % (mean, SD) | 28.7 ±6.7 | 30.4 ±6.4 | < 0.0001 |
[i] AF – atrial fibrillation, IQR – interquartile ranges, MI – myocardial infarction, PCI – percutaneous coronary intervention, CABG – coronary artery bypass grafting, PM – pacemaker, Y – Yates correction, ICD – implantable cardioverter defibrillator, CRT-D – cardiac resynchronization therapy defibrillator, HF – heart failure, CKD – chronic kidney disease, COPD – chronic obstructive pulmonary disease, OHCA – out-of-hospital cardiac arrest, NYHA – New York Heart Association, STEMI – ST-segment elevation myocardial infarction, SR – sinus rhythm, LVEF – left ventricular ejection fraction, SD – standard deviation.
Table II
In-hospital treatment procedures and pharmacotherapy at discharge
[i] AF – atrial fibrillation, PCI – percutaneous coronary intervention, CAD – coronary artery disease, GP – glycoprotein, TIMI – thrombolysis in myocardial infarction, IABP – intra-aortic balloon pump, Y – Yates correction, CABG – coronary artery bypass grafting, VKA – vitamin K antagonist, NOAC – new oral anticoagulant, LMWH – low molecular weight heparin, ACEI – angiotensin-converting enzyme inhibitor, ARB – angiotensin receptor blocker, ARNI – angiotensin receptor-neprilysin inhibitor.
The 12-month outcomes are presented in Table III. Significantly higher mortality, HF hospitalization, as well as stroke and MACE rates were observed in patients with AF. Patients with AF and a MACE during the follow-up period had a higher mean CHA2DS2-VASc score at admission compared to those without a MACE (Table IV). The Kaplan-Meier curves comparing the mortality and MACE differences between the 2 groups during the 1-year follow-up showed a better prognosis for the patients without AF (Figures 2 and 3). In the multivariate analysis of the entire study population, AF was revealed to be one of the factors associated with a higher all-cause mortality (OR = 1.20, 95% CI: 1.03–1.40, p = 0.018) and MACE incidence (OR = 1.23, 95% CI: 1.08–1.41, p = 0.002) during the 12-month follow-up period (Tables V and VI).
Table III
Cardiac implantable electronic device implantation and events in 12-month follow-up
[i] AF – atrial fibrillation, CIED – cardiac implantable electronic device, PM – pacemaker, ICD – implantable cardioverter defibrillator, CRT-D – cardiac resynchronization therapy defibrillator, Y – Yates correction, CRT-P – cardiac resynchronization therapy pacemaker, MI – myocardial infarction, HF – heart failure, MACE – major adverse cardiac events.
Table IV
Values of CHA2DS2-VASc score in atrial fibrillation patients with or without MACE incidence during the follow-up period
Figure 2
All-cause mortality in 12-month follow-up in patients without and with atrial fibrillation. Kaplan-Meier curves
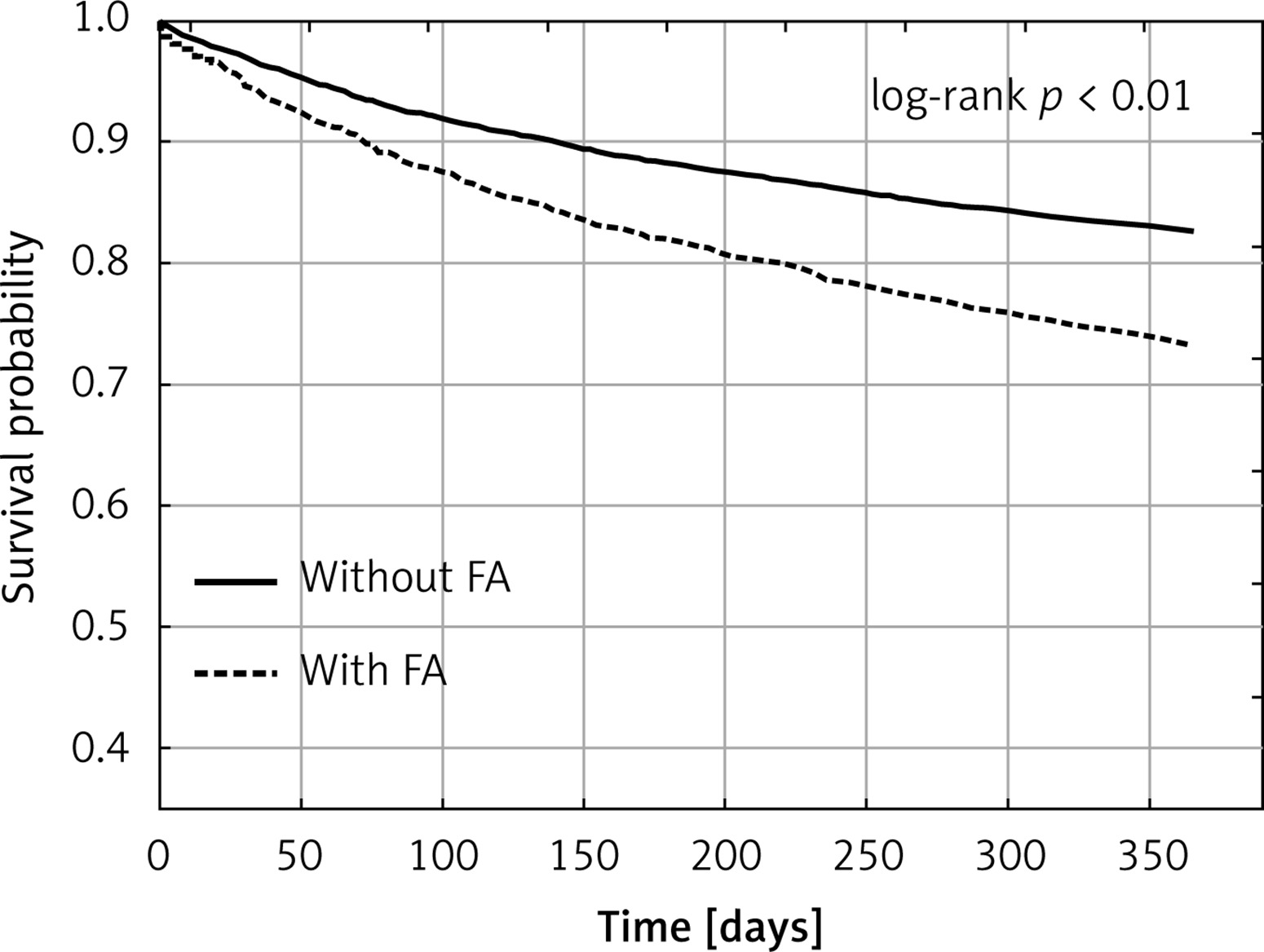
Figure 3
Major adverse cardiovascular event incidence in 12-month follow-up in patients without and with atrial fibrillation. Kaplan-Meier curves
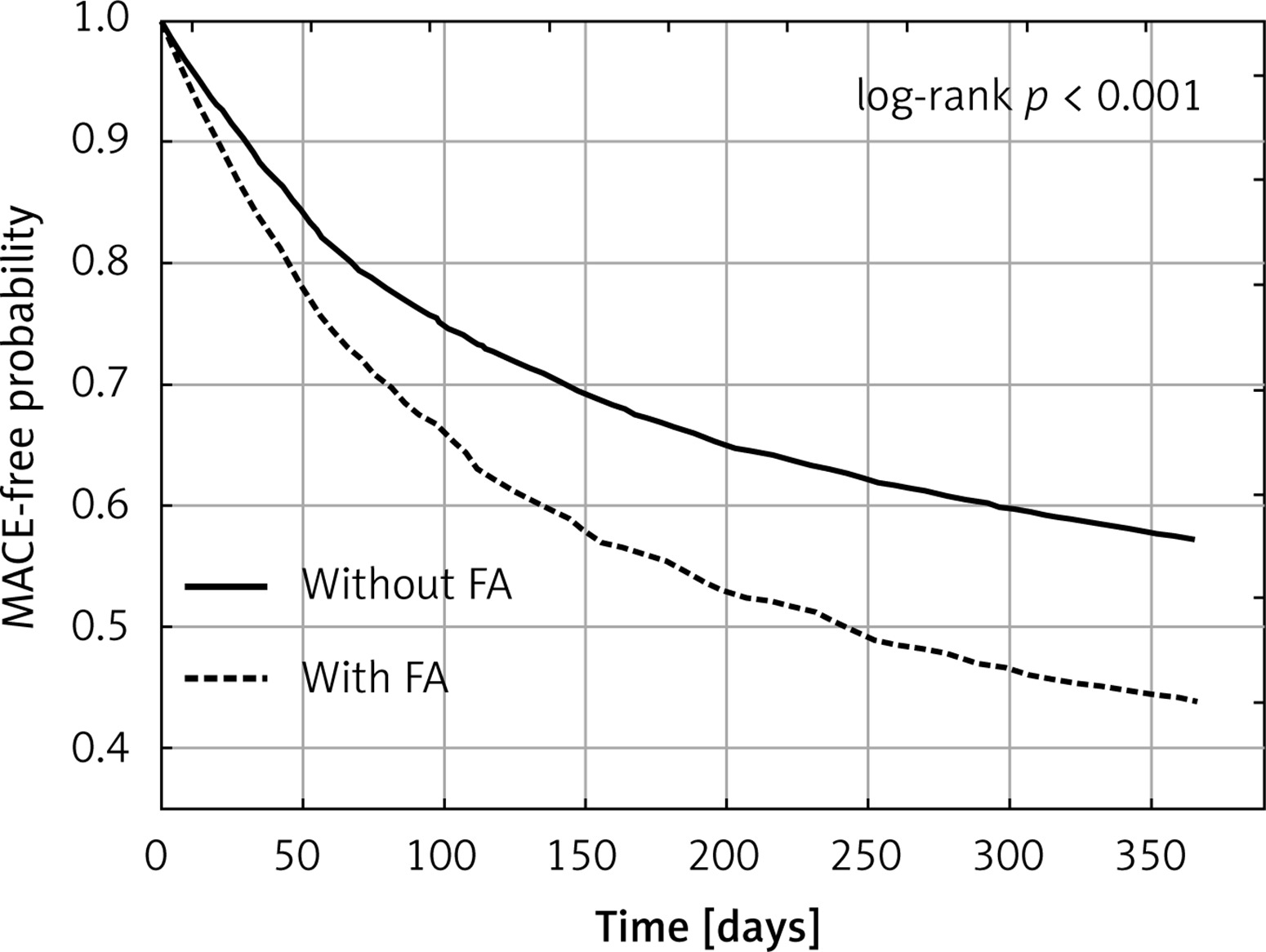
Table V
Multivariate analysis. All-cause mortality in 12-month follow-up after discharge
Table VI
Multivariate analysis. Major adverse cardiac events in 12-month follow-up after discharge
[i] MACE – major adverse cardiac events, OR – odds ratio, CI – confidence interval, NYHA – New York Heart Association, EF – ejection fraction, STEMI – ST-segment elevation myocardial infarction, NSTEMI – non-ST-segment elevation myocardial infarction, AF – atrial fibrillation, ACEI – angiotensin-converting enzyme inhibitor, ARB – angiotensin receptor blocker, ARNI – angiotensin receptor-neprilysin inhibitor.
Discussion
Patients after MI with LVEF under 40% with AF, compared to those without AF, showed inferior in-hospital clinical characteristics, were less frequently subjected to coronary angiography and PCI during hospitalization, and had worse 12-month outcomes.
Reduced LVEF in patients after MI is a predictor of poor prognosis [2]. The plurality of clinical characteristics and the long-term prognosis of patients after MI with LVEF < 40% is still unappreciated. The majority of randomized trials evaluating therapeutic or mechanical interventions have been restricted to patients with symptomatic congestive heart failure (CHF) and impaired left ventricular function [9, 15–17]. The number of papers assessing factors that affect the long-term prognosis in patients after MI with impaired left ventricular function is still insufficient. AF seems to be an underestimated factor. Patients with AF have more comorbidities and have a higher risk of complications [4, 18, 19].
The available reports assessing the influence of AF on the long-term outcomes in patients with LVEF < 40% are restricted to those with HFrEF [20–23]. The published data come mainly from scanty HF registries. The HF Long-Term Registry of the ESC includes data collected in 21 countries from 12,440 patients. Over 40% of them were hospitalized with acute HF and nearly 60% were outpatients with chronic HF [24]. The Swedish Heart Failure Registry (Swede-HF) is a prospective, ongoing registry that records data at discharge from hospitals or after outpatient clinic visits [22]. The Korean Acute Heart Failure Registry (KorAHF) was a prospective registry that enrolled patients hospitalized with acute HF at tertiary university hospitals [23, 25, 26].
In patients with HFrEF, the prevalence of AF ranges from < 10% to 53% [22, 27, 28]. The prognostic impact of AF, according to different types of HF, especially HFrEF, has not been fully evaluated. In a population of 14,964 patients included in the ESC-HF long-term registry, Zafrir et al. found that all-cause death and HF hospitalization rates were higher in patients with AF compared to those with sinus rhythm (SR) in each of the three EF groups [20]. In the KorAHF registry, AF was found to be associated with increased mortality only in patients with HFpEF, but not in those with HFrEF and HFmrEF [23]. In a cohort of 41,446 patients enrolled in the Swede-HF registry, patients with AF compared to those with SR in each of the three EF groups had an increased risk of death, HF hospitalization, and stroke [22]. Similarly, in our analysis, patients with AF had a higher incidence of all-cause mortality, HF hospitalization, stroke, and MACE during the 12-month follow-up period.
Unfavorable long-term outcomes of AF patients require an explanation. Patients with AF compared to those with SR are older, have a higher rate of previous HF hospitalizations and inferior clinical characteristics [20, 22]. In the ESC-HF long-term registry, after a multivariable adjustment, AF was associated in each of the three HF subtypes with older age, reduced functional capacity, previous HF hospitalizations, higher heart rates, and more significant signs of congestion [20]. In the Swede-HF registry, patients with AF compared to those with SR were older and were characterized by a longer duration and more severe HF, lower creatinine clearance, and more frequent hypertension, TIA, or stroke. These patterns were similar in all three HF groups [22]. In our study, patients with LVEF < 40% and concomitant AF were older, had a higher rate of previous MI, revascularization procedures, CKD, and HF hospitalizations. Due to inclusive criteria used by our registry, as well as the cited ones, the study groups were heterogeneous. Therefore, the comparisons of patients with and without AF might be methodically questionable. In spite of that, a common feature of all the registries is the older age of patients with AF and the differences in basal characteristics of patients with and without AF. The long-term results are not analogous. Both in the HF Long-Term Registry and the Swede-HF Registry, patients with AF had higher mortality and worse long-term outcomes. In the KorAHF Registry, patients differed in the stroke rate, without a significant difference in the mortality rate in the long-term follow-up period.
Surprisingly, less than 40% of patients with AF were prescribed anticoagulants at discharge. Moreover, only 17.1% were recommended to be treated with vitamin K antagonists (VKA), 7.1% with new oral anticoagulants, and 18.5% with low molecular weight heparin. Our analysis involved patients enrolled in the Registry from 2003. The advantages of the anticoagulant therapy were less evident at that time. Low molecular weight heparins were not infrequently prescribed as the bridge therapy in patients treated ultimately with VKA.
Our multivariate analysis revealed AF to be an independent predictor of death and MACE incidence after discharge. However, whether AF is associated with less favorable outcomes in HFrEF patients remains controversial [22]. In the ESC-HF long-term registry, AF in patients with HFpEF and HFmrEF was correlated with inferior cardiovascular outcomes, including death, though this was not true in the case of patients with HFrEF [20]. In the Framingham Heart Study, AF was associated with a similar risk of death in the incident HFpEF and HFrEF [29]. In the CHARM study, AF was associated with a relatively greater risk of the major outcomes in patients with a preserved EF than in patients with a low EF [30]. In the Swede-HF registry, the association of AF with outcomes and hazard ratios ranging from 1.11 to 1.29 for the three EF groups was similar [22]. A multivariate analysis showed protective effects of hypercholesterolemia and PCI performed in myocardial infarction from the radial artery access, and a better prognosis of patients with STEMI compared to those with NSTEMI. Patients undergoing surgery using the radial artery access are exposed to fewer hemorrhagic complications, which is particularly important in patients with AF treated with chronic anticoagulation. Patients with STEMI infarction are generally younger, have fewer associated diseases, and the identification of the vessel responsible for the infarction is generally more unambiguous in their case.
The study has strengths and limitations. The analysis involved only surviving patients, excluding those who died during the index hospitalization. Some other limitations are typical for registry-based cohort studies. Firstly, the treatment and in-hospital events may be underreported, probably due to incomplete records in the database. For example, LVEF was available for 76.5% of patients with MI. Secondly, as reporting to the registry was not obligatory, not all patients with MI in Poland were reported. A detailed follow-up was also available only for a limited number of patients. Thirdly, as our research is an observational study, some bias related to the lack of possibility of adjusting all variables might influence the final results. The causality of the results cannot be confirmed, as the study was retrospective. For these reasons, all results should be interpreted with caution. The subject still requires a further investigation, preferably in the form of a prospective study.
Our study also has some strengths. The PL-ACS Registry provides an opportunity to investigate, in a reliable manner, the treatment and outcomes of patients encountered in general practice. Among them, a longitudinal observation of a large number of patients, as well as detailed data on the medical history, treatment at discharge, and events within the follow-up period, can be highlighted. Moreover, the study showed the natural history of MI patients in real world settings. Finally, our research provided a hypothesis for further studies.
In conclusion, patients after MI with LVEF < 40% with AF, compared to those without AF, had inferior clinical characteristics, were less frequently subjected to coronary angiography and PCI during hospitalization, and – finally – had significantly less favorable 12-month outcomes, with higher rates of death and MACE.