
Among the chronic diseases currently affecting society, diabetes mellitus is one of the most worrying. Its global prevalence is growing rapidly, and by 2045, the International Diabetes Federation (IDF) predicts that approximately 783 million adults will be living with diabetes, resulting in greater life-threatening health complications and hospitalizations, and reduced life expectancy [1]. Over 90% of people with diabetes have type 2 diabetes (T2DM), with the key contributors being the ageing population, sedentary lifestyle, increasing prevalence of overweight and obesity, and growing urbanization. The condition often remains asymptomatic for many years; however, early detection of increased blood glucose concentration, followed by a successful reduction of modifiable risks, can significantly delay or inhibit the development of full-blown T2DM and its complications [2]. A key role in such preventive strategies may be played by community pharmacists, who are often the first point of contact between patients and the healthcare system [3–7].
The paper presents the results of a pilot national screening program for T2DM introduced to Polish community pharmacies by the professional body, i.e. the Pharmacists’ Chamber (Naczelna Izba Aptekarska). During the program, pharmacists interviewed patients according to the FINnish Diabetes RIsk SCore questionnaire (FINDRISC) intended for patients at high risk of T2DM. They also performed capillary blood glycaemia measurements, together with further interventions such as education or referral to a general practitioner, depending on the result. The pharmacist-led interventions were carried out according to a new algorithm on taking blood glucose measurements in community pharmacy; this was introduced very recently as a joint strategy by diabetologists and pharmacists (i.e. the co-authors of the current study) [8].
Methods
The research was awarded approval/was approved by the Ethics Committee of the Poznan University of Medical Sciences (KB 137/25) as an open, retrospective study. For details, see Supplementary data.
Results
A total of 195 community pharmacies and 1813 subjects participated in the screening, with a mean number of nine subjects per location. Complete data was obtained for 1153 subjects; their general characteristics are provided in Supplementary Table SI. Of these, 1092 subjects (94.7%) reported no history of diabetes or use of insulin/oral hypoglycemic medications, and these patients were included into screening for T2DM. Most were women (n = 756, 69.2%), and between the ages of 45 and 64 years (n = 359, 32.9%). Fasting and random blood glucose values demonstrated significant variation according to sex and age (Supplementary Table SI, Supplementary Figures S1 and S2).
FINDRISC questionnaire
The enrolled subjects were predominantly characterized with a slightly elevated risk of diabetes according to FINDRISC (N = 395, 36.2%). Of the 1092 subjects, 183 (16.7%) had a score exceeding 15 points, corresponding to a high to very high risk of T2DM over 10 years.
Capillary blood glucose
In the subgroup of patients indicating fasting glycaemia (N = 180/1092), 64 (35.5%) subjects exhibited/had capillary blood glucose values between 5.6 and 6.9 mmol/l and 21 (11.8%) patients had a result exceeding 6.9 mmol/l. The total number of pharmacist-led referrals to general practitioners (GPs) was 85 (47.3%).
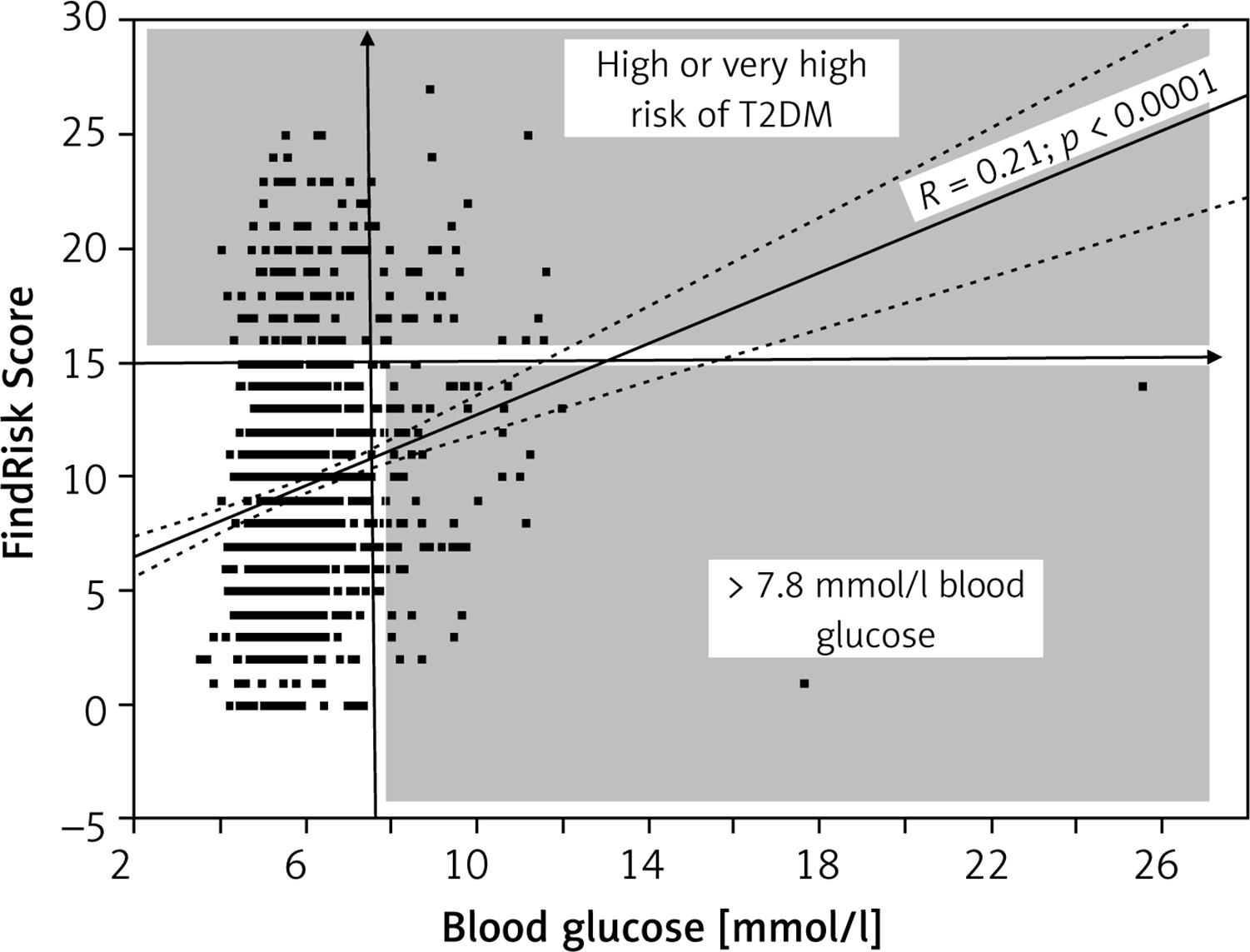
Regarding the random blood glucose results, 66/912 (7.2%) subjects demonstrated/had capillary blood glucose values between 7.8 and 11.0 mmol/l and eight (0.9%) exceeded 11.0 mmol/l; the total number of pharmacist-led referrals to GP was 74 (8.1%) (Supplementary Table SII). In addition, 14 of the 95 patients with fasting blood glucose below 5.6 mmol/l, and 126 of the 838 patients with random blood glucose below 7.8 mmol/l, obtained high to very high FINDRISC scores (Supplementary Table SIII). These subgroups of patients were candidates for additional pharmacist-led education about life style modification to prevent T2DM. A modest but significant (p < 0.0001) correlation was noted between increased capillary blood glucose and FINDRISC score (Figure 1). While four of the 1092 subjects (0.4%) demonstrated/had capillary blood glucose < 3.9 mmol/l, these values were not accompanied by additional clinical signs that could suggest hypoglycemia.
Figure 1
Correlation between increased capillary blood glucose and FINnish Diabetes RIsk SCore. R(Spearman) = 0.25 (p < 0.00001), N = 1092 subjects. The patterned field shows study participants – candidates for further education and consultation with a GP
Patients referred to their GP were informed that if they were diagnosed with diabetes and prescribed a new medication, they could contact the pharmacist again to be covered by the New Medicine Service [8] (Supplementary Figures S1 and S2).
Discussion
Our findings highlight the important role played by community pharmacists in diabetes screening and prevention, specifically in the context of the national screening program for type 2 diabetes (T2DM). This retrospective study included 1813 participants from 195 community pharmacies, with 1153 subjects fully completing the study. While blood pressure measurements had already been performed during MMM (May Measure Month) [9] or as part of local screenings in community pharmacies [10, 11], this was the first initiative intended specifically for diabetes patients. The use of the algorithm in the present study ensured consistency in procedures and educational activities among pharmacists, while allowing them to adapt their approach to each participant with official educational materials [8].
The group of participants in the present study was strongly represented by women and individuals aged 45‒64 years. This is consistent with the existing literature showing that these groups are at higher risk of developing T2DM. Previous studies indicate that women, particularly during menopause, experience increased risk of T2DM due to hormonal changes and associated metabolic shifts [12]. Moreover the predominance of female participants in our survey might be supported by the evidence indicating that women are more likely than men to engage in preventive health behaviors, including attending routine medical checkups and undergoing screening procedures [13]. Regular screenings in pharmacies could help in targeting these high-risk groups and could potentially mitigate the risk of diabetes. Additionally, older patients often exhibit various metabolic changes that increase the likelihood of developing T2DM, such as decreasing insulin sensitivity.
Community pharmacies are often the first point of contact for patients, and as such, the pharmacist is in an ideal position to implement risk assessment tools such as FINDRISC. Our findings indicate that 36.2% of participants had a slightly elevated risk of T2DM, and 16.7% were at high to very high risk. The identification of high-risk individuals allows pharmacists to take the next step in patient care; this can take the form of referral to GPs or offering personalized educational support concerning T2DM following diagnosis, such as the New Medicine Service. By using tools like FINDRISC, pharmacists are able to target those who may benefit most from additional support and ensure that they receive timely medical intervention [14].
A key part of the study was the performance of capillary blood glucose testing within the designed algorithm. The findings indicate that 35.5% of participants had impaired fasting glucose (IFG) levels between 5.6 and 6.9 mmol/l, while 11.8% had levels above 6.9 mmol/l, indicating undiagnosed diabetes. As a result, 47.3% of these individuals were referred by pharmacists to their GPs for further evaluation and diagnosis. The study also found that 7.2% of participants had elevated random glucose levels (7.8‒11.0 mmol/l), and 0.9% had levels above 11.0 mmol/l; both are indicative of diabetes. This again highlights the critical role community pharmacists can play in diabetes management by facilitating early detection and timely referrals. Recent studies confirm that pharmacist-led diabetes screening and referrals can significantly improve early diagnosis and management. By assessing blood glucose levels and referring patients promptly to physicians, pharmacists contribute to reducing the risk of diabetes-related complications and improving long-term health outcomes [15].
The use of lifestyle modifications such as changes in diet, physical activity and weight management is a key intervention for preventing or delaying T2DM. Pharmacists are well-positioned to deliver lifestyle education and counseling, a role increasingly recognized in the literature. By offering individualized guidance, pharmacists help high-risk individuals make informed decisions to reduce their risk of developing diabetes [16]. Evidence indicates that proactive screening of individuals at high risk may lead to the diagnosis of diabetes approximately three years earlier compared to scenarios in which no screening is conducted [17]. Moreover, such an initiative provides an opportunity to introduce a novel service for patients, thereby demonstrating the added value of community pharmacies and underscoring their broader role in public health promotion. However, adaptations at both the pharmacy level and within the broader healthcare system are essential to ensure the efficacy of such a service and to facilitate its successful long-term and large-scale implementation. Firstly, the implementation of an electronic health record system is crucial to enable pharmacists to share patient data with general practitioners. This would ensure that individuals with suspected prediabetes or T2DM, as well as those presenting relevant risk factors, are referred to their GPs for diagnostic evaluation and receive appropriate recommendations regarding lifestyle modifications and/or pharmacological treatment. Subsequently, the patient would be referred back to the same pharmacy to participate in the New Medicine Service, thereby receiving continued support from the pharmacist in managing newly prescribed medications and implementing non-pharmacological interventions. Secondly, there is a need to establish the reimbursement of the service from the state budget in order to maintain financial profitability by the pharmacies. For example in a pilot study by Rondeaux et al. in Belgium, the pharmacists were remunerated at a rate of EUR 30.00 per patient [18]. In the United Kingdom the estimated cost of £18.83 was seen as representing good value, to provide the service nationally [7]. For comparison, in Poland, vaccinations – currently the only service financed through public funds – are reimbursed at a rate of EUR 9.00 per patient. Comparable studies investigating the role of community pharmacies in health promotion and disease prevention have been carried out in Eastern European countries, including Slovakia and southern Croatia, concluding that such involvement may contribute to reducing healthcare costs [19, 20].
In present study, individuals with high FINDRISC scores and abnormal glucose levels were educated on lifestyle changes by pharmacists, reinforcing the importance of this intervention. Further research could explore the long-term impact of pharmacist-led lifestyle education on the prevention of diabetes and other metabolic disorders.
This study has some limitations. It is at risk of some potential selection bias due to the involvement of pharmacies already participating in a national screening program: these community pharmacies may have been more motivated or experienced in diabetes screening, which could affect the generalizability of the results. Additionally, the short duration (8 weeks) of the study limits the ability to assess the long-term outcomes of pharmacist-led interventions. The assessment of the present study’s effectiveness – due to fragmented healthcare system, undoubtedly limits the current survey. Additionally, some recent studies have shown that follow-up with physicians regarding referral outcomes for at-risk participants could not be assessed, or that a substantial proportion of referred high-risk patients failed to attend follow-up medical consultations [18, 21, 22]. Given the exploratory nature of this pilot study, which aimed to assess the prevalence and basic characteristics of abnormal glucose levels and elevated FINDRISC scores, extended analyses involving multivariable modeling were not conducted at this stage. Future studies should examine the long-term effects of such interventions on reducing the incidence of T2DM; these studies would also benefit from including more diverse populations and the diagnosis given by the physician/GP after referral.
In conclusion, our findings underscore the significant role that can be played by community pharmacists in the early detection of type 2 diabetes, its prevention and the referral of patients to GPs. By using tools like the FINDRISC and conducting blood glucose testing, pharmacists can identify individuals at high risk of T2DM and provide essential referrals and lifestyle education. As the global burden of diabetes rises, integrating pharmacists into public health strategies is a valuable step in improving early detection and reducing its long-term impact.