Stroke remains a leading cause of death and disability globally, accounting for approximately 11.6% of deaths, and a major contributor to global morbidity [1]. In Argentina, about 2% of adults older than 40 years have experienced a cerebrovascular event [2]. Recurrent cerebrovascular and cardiovascular events occur in 5–13% of survivors, further increasing disability and mortality risks [3].
Effective secondary prevention including control of vascular risk factors and pharmacotherapy reduces recurrent event risk [4]. However, success largely depends on patient adherence to medication regimens [5]. Real-world adherence in Latin America is poorly characterised, complicated by socioeconomic, cultural, and healthcare system differences [6–8]. Studies report variable adherence rates, ranging from approximately 65% in stroke survivors in Chile to significant discontinuation among Argentine patients on anticoagulation [9]. Adherence is influenced by education, economic factors, cognitive status, and healthcare access [10]. Recent systematic reviews and meta-analyses confirm persistent gaps in adherence across cardiovascular conditions and support the effectiveness of multicomponent and digital/mHealth strategies to improve adherence [11–14].
This study aims to evaluate medication adherence rates and associated factors among Argentine adults in primary (vascular risk without prior events) and secondary (post-vascular event) prevention groups, addressing critical gaps in regional adherence data.
Methods
Population and sampling
Two groups of participants were recruited. The Primary Prevention Group (PPG) included adults aged 18 years or older with hypertension, diabetes, overweight or obesity, and/or dyslipidaemia, but without a prior history of stroke or myocardial infarction. The Secondary Prevention Group (SPG) included adults aged 18 years or older with a documented clinical history of ischaemic or haemorrhagic stroke, transient ischaemic attack, or acute myocardial infarction. Participants in the SPG were recruited from an institutional ischaemic stroke cohort database and had been admitted between 2017 and 2020. Participants in the PPG were recruited through a consumer database provided by a leading national beverage distribution company, which distributes still and sparkling water across Argentina. We had previously collaborated with this company in survey-based projects and for the present study; they facilitated access to their mailing distribution platform, allowing us to reach a large number of individuals for inclusion in the primary prevention group. Group allocation was determined based on self-reported medical history.
Because these recruitment strategies represent distinct sampling frames (consumer mailing list vs. clinical registry), the PPG and SPG were not methodologically comparable. Therefore, any between-group differences should be interpreted as descriptive, unadjusted observations rather than comparative inference.
Survey instrument and administration
A 14-item anonymous online questionnaire collected data on demographics, medical history, medication use by drug class (antiplatelet agents, anticoagulants, antihypertensives, lipid-lowering agents, and oral hypoglycaemics), adherence (continuous use since last medical contact vs. discontinuation or missed doses), reasons for non-adherence, health insurance coverage, medication costs, and use of adherence support tools. The median completion time was approximately 5 min. All variables, including medication adherence, were self-reported. The questionnaire was developed for this study and was not a validated adherence instrument.
The full questionnaire is available as Supplementary Material.
Definitions and variables
Self-reported adherence was defined as the continuous use of prescribed vascular prevention medications without interruption since the last documented physician encounter. Reasons for non-adherence included forgetfulness, medical indication for discontinuation, treatment cost, adverse effects, and limited accessibility. Medication use was captured at the drug-class level (antiplatelet agents, anticoagulants, antihypertensives, lipid-lowering agents, and oral hypoglycaemics) and did not differentiate individual medications within each class. Demographic variables analysed included age, sex, educational attainment, household size, health insurance coverage, and out-of-pocket medication costs.
Statistical analysis
Data were summarised using descriptive statistics. Unadjusted between-group differences were reported for descriptive purposes, given the non-comparable sampling frames. P-values were presented as exploratory measures. Given the descriptive, exploratory nature of the survey and the limited set of self-reported covariates, we did not perform multivariable analyses. All analyses were conducted with IBM SPSS Statistics, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Participant characteristics
A total of 2069 respondents completed the survey: 1622 in the PPG and 447 in the SPG. Survey invitations were sent by e-mail to 1283 patients from the institutional stroke database, yielding 121 responses (response rate 9.4%). In addition, 111,150 invitations were distributed via the consumer database of the national water distribution company; of these, 41,060 e-mails were opened (open rate 37%), and 2730 responses were obtained (response rate 6.6%). Among these responses, 326 individuals reported a prior history of stroke or myocardial infarction and were included in the SPG (together with 121 institutional respondents, for a total of 447), while 1622 reported vascular risk factors without a history of stroke/MI and were included in the PPG.
The mean age was 56.0 ±13.5 years in the PPG and 58.0 ±14.5 years in the SPG (p = 0.02). Females comprised 67.0% of PPG and 52.6% of SPG participants (p < 0.0001). Approximately 45% in both groups had completed tertiary or university education. Health coverage was reported by approximately 91% of participants in both groups (Table I).
Table I
Demographic and clinical characteristics of primary prevention group (PPG) and secondary prevention group (SPG) participants. Summary of participant age, sex distribution, education level, health coverage, medication costs, and other relevant baseline characteristics for the 2 study groups
Medication use and adherence
A total of 77.6% of the PPG and 84.6% of the SPG were taking at least one medication. Antihypertensive and lipid-lowering agents were the most frequently used drugs. For all evaluated medications, medication use was reported more frequently in the SPG than in the PPG. Table II shows the medications received by patients in both groups.
Table II
Medication use rates by group and therapeutic class. Proportion of participants reporting use of vascular prevention medications (antihypertensives, lipid-lowering agents, oral hypoglycaemics, antiplatelets, anticoagulants) within each group
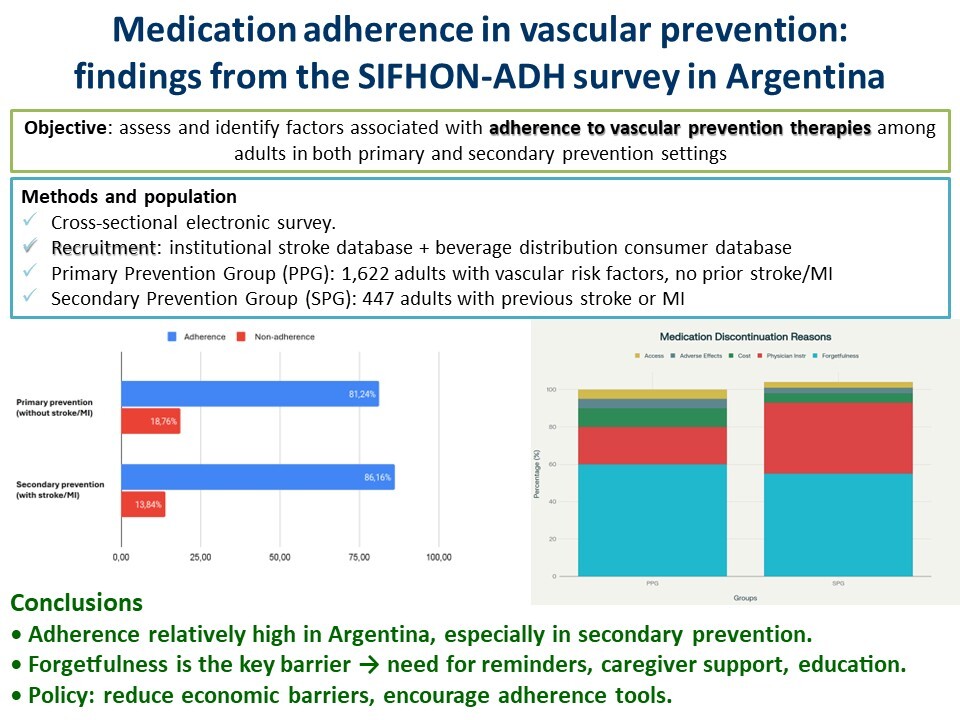
Self-reported adherence to vascular prevention medication was 86.2% in the SPG and 81.2% in the PPG. Antihypertensive therapy showed the highest reported adherence in both groups (90.2% and 86.4%, respectively). The second most adherent pharmacological group was oral hypoglycaemic agents (87.7% and 84.5%, respectively). Regarding antithrombotic therapy, only patients under secondary prevention were considered, given the non-standardised indication of antiplatelet therapy for primary prevention. In this group, adherence rates were 82.8% for antiplatelet agents and 87.2% for anticoagulants.
Reasons for non-adherence and discontinuation
Forgetfulness was the most commonly reported reason for non-adherence, accounting for 52.1% to 70.2% of participants across medication classes. Physician-advised discontinuation was notably frequent among SPG patients, especially for antiplatelet (39.6%) and antihypertensive (37.0%) medications. In both groups, lipid-lowering agents showed the highest discontinuation rates (14.9% and 24.4%, respectively), with consistently higher discontinuation observed in the PPG. Economic cost, limited access, and adverse effects were less commonly cited.
Discussion
This study describes self-reported medication adherence patterns among Argentine adults in primary and secondary vascular prevention drawn from two distinct recruitment frames. In this sample, self-reported adherence was 81.2% in the PPG and 86.2% in the SPG; however, due to the non-comparable sampling strategies and potential confounding, these figures should be interpreted as descriptive observations rather than comparative inference.
There is limited literature on this topic in our region. A study conducted in Chile, with telephone follow-up of 156 patients diagnosed with ischaemic stroke and TIA, reported a marked decline in long-term adherence to anticoagulant therapy, with no significant changes in adherence to statins, antihypertensives, or hypoglycaemic agents, which remained above 65% [9]. Studies in acute myocardial infarction, diabetes, and hypertension have shown that educational level influences adherence to both pharmacological and non-pharmacological measures [8, 15, 16]. In Argentina, a study following patients on anticoagulation after hospital discharge for atrial fibrillation found that, after 1 year, 3 out of 10 had discontinued treatment [17].
Antihypertensives exhibited the highest adherence, consistent with their pivotal role in controlling vascular risk. Non-adherence to antihypertensive medication is the most important cause of uncontrolled blood pressure and is influenced by multiple interrelating factors [18]. High adherence to oral hypoglycaemics further reflects growing awareness of diabetes as a major vascular risk factor. Medication use and adherence were captured at the drug-class level; therefore, we could not differentiate adherence to specific lipid-lowering agents (e.g. statins vs. other therapies) or specific glucose-lowering medications (e.g. GLP-1 receptor agonists or SGLT2 inhibitors).
Forgetfulness emerged as the most common reason for non-adherence among participants in both prevention groups (47.9% in PPG and 33.9% in SPG). This aligns with published evidence showing that unintentional non-adherence and disruptions in daily routines are frequent barriers in cardiovascular prevention [10, 19]. Interventions such as reminders and simplified routines have shown promise in improving adherence, including SMS/app-based reminders, electronic pillboxes, caregiver support, and patient education [12, 13]. From an implementation perspective, barriers like forgetfulness are potentially amenable to digital interventions, whereas cost- and access-related barriers generally require system-level solutions (e.g. coverage policies, copayment reduction, and ensuring a reliable medication supply).
Physician-directed medication discontinuations represent a potentially impactful and underexplored finding. While discontinuation can be clinically appropriate (e.g., adverse effects or deprescribing), it may also reflect gaps in shared decision-making, misconceptions about long-term therapies (including statins), treatment burden, or fragmented follow-up [20, 21]. Structured medication reconciliation and clear, guideline-based documentation of indications for continuation/discontinuation (particularly at transitions of care) may help distinguish appropriate discontinuation from avoidable interruption and reduce preventable recurrent vascular events [22, 23]. Because this information was self-reported and we did not capture the clinical context or documentation, we cannot determine appropriateness, indications, or temporality. Future studies linking patient-reported data with medical records and pharmacy dispensing information are needed to distinguish appropriate deprescribing from avoidable interruptions and to better understand the drivers of discontinuation.
This study has several limitations. All data were self-reported and susceptible to recall and social desirability biases. Participation was voluntary and relied on 2 non-comparable sampling frames (a consumer mailing list for PPG and a clinical registry for SPG), which is likely to have introduced socioeconomic selection biases and limits representativeness. Response rates were low, and responders may be more health-conscious, digitally engaged, and adherent than non-responders, potentially inflating adherence estimates. The questionnaire was developed for this study and was not a validated adherence tool. Adherence was operationalised as self-reported continuous use without interruption since the last encounter with a physician; we did not assess dose timing, persistence over time, or refill behaviour. Medication use was recorded by drug class, and we did not differentiate individual agents within classes. We did not collect detailed comorbidities (e.g. chronic kidney disease) or clinical severity measures that could influence adherence. Finally, given the limited set of covariates and the non-comparable recruitment strategy, between-group differences should be interpreted as descriptive and unadjusted.
As strengths, this survey achieved a large sample size and provides exploratory, real-world information on self-reported adherence patterns and barriers in Argentina, a region with limited published data. The study also captured multiple patient- and system-level factors, including reasons for discontinuation and the use of adherence support tools, which can inform hypotheses and future targeted interventions.
In conclusion, our survey provides exploratory, descriptive evidence on self-reported medication adherence among Argentine adults in vascular prevention. Barriers included forgetfulness, medication costs/access, and self-reported physician-advised discontinuation. Future work should use representative sampling, validated adherence instruments, objective verification, and adjusted analyses to better quantify adherence and guide interventions.