Introduction
Despite recent improvements in clinical management of encephalitis, the syndrome still remains challenging due to its potentially severe course and risk of mortality [1]. In more than 50% of cases, the etiologic factor of neuroinflammation remains undetermined due to the vast number of infectious and noninfectious causative agents, resulting in often time-consuming and complicated diagnostic procedures [2–5]. Moreover, different pathogens may generate similar clinical pictures, such as Lyme neuroborreliosis (LNB) and enteroviral (EV) encephalitis [6]. The leading causes of CNS inflammation are viral infections (45–69% of all cases), mostly triggered by human herpesvirus type 1 (HSV) and enteroviruses, which constitute up to 24% and 6–25% of confirmed encephalitis cases, respectively [5, 7, 8]. Up to 20% of encephalitis cases are immune-mediated, with the presence of anti-neuronal or anti-glial antibodies, in particular autoantibodies against N-methyl-d-aspartate receptor (anti-NMDAR) [9].
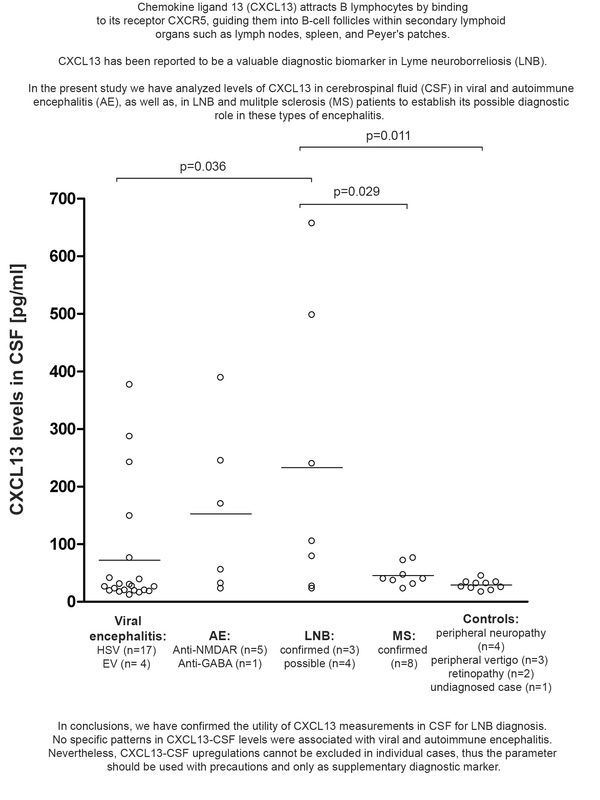
Due to the variety of encephalitis types, it is vital to develop new tests and biomarkers which will allow for early diagnosis and their differentiation. Chemokine (C-X-C motif) ligand 13 (CXCL13) seems to be a new and promising biomarker, as its utility has already been confirmed in LNB diagnostics [2, 10, 11]. High chemokine concentrations in cerebrospinal fluid (CSF) were found to be strongly associated with the early phase of acute LNB and correlated with changes of typical CSF neuroinflammation markers (e.g. pleocytosis and CSF protein levels) [12]. Changes in CXCL13-CSF concentrations were also suggested to serve as a prognostic biomarker for multiple sclerosis (MS) progression [13], while CXCL13 serum levels were found to be associated with treatment response in MS [14, 15]. Among other immune diseases, CXCL13 was proposed as a possible marker and future therapeutic target [16] in systemic lupus erythematosus [17], rheumatoid arthritis [18], Sjögren’s syndrome [19], myasthenia gravis [20], and inflammatory bowel disease (IBV) [21]. CXCL13-CSF levels as high as in LNB were also reported in neurosyphilis, and therefore it was proposed to use it as a diagnostic marker useful in patients also infected with human immunodeficiency virus (HIV), as the virus itself might trigger pleocytosis [22–24].
In this study, we analyzed CXCL13-CSF levels in viral and autoimmune encephalitis (AE), as well as in LNB and MS patients, to establish its possible diagnostic role in these types of encephalitis.
Material and methods
We analyzed 52 adult (≥ 18 years) patients who were admitted to two Warsaw hospitals: i) patients with encephalitis and LNB were hospitalized in the Hospital for Infectious Diseases in Warsaw; ii) MS patients and control subjects were hospitalized in the Department of Neurology, Medical University of Warsaw. Written informed consent was obtained from all study participants or from their relatives if the participant was unable to provide consent. The study was approved by the Internal Review Board of the Medical University of Warsaw.
Encephalitis
Viral encephalitis patients consisted of subjects from a previously described surveillance study focused on the etiology of encephalitis [8]. Encephalitis was defined by the presence of an altered mental status, decreased level of consciousness, seizures or focal neurological signs, together with at least one abnormality in the cerebrospinal fluid (CSF): white blood cell count ≥ 4 cells/mm2 and/or protein level ≥ 40 mg/dl [8]. Only patients with confirmed encephalitis caused by HSV and EV were included in the study. Viral etiology was determined based on positive viral detection performed in CSF using non-commercial PCRs [25, 26].
Lyme neuroborreliosis
Patients with LNB were part of a previously described study in which CXCL13-CSF levels were measured [6]; however, for the purpose of normalization, these measurements were performed once again in the same run with other samples analyzed in the present study.
LNB was diagnosed according to the guidelines recommended by the European Federation of Neurological Societies (EFNS) [27]. Besides clinical criteria, B. burgdorferi s.l. specific antibodies were detected in paired sera and CSF samples using Borrelia IgM/IgG ELISA tests (Biomedica, Vienna, Austria). Positive ELISA detections were confirmed by Western blot (recomLine Borrelia IgM and recomLine Borrelia IgG; Mikrogen Diagnostik, Neuried, Germany).
PCR detecting the Borrelia flagellin gene (flaB) was employed as described previously [28]. In short, DNA was extracted from 200 µl of serum and CSF samples with the DNeasy Blood & Tissue Kit (Qiagen, Hilden, Germany) and then subjected to amplification using GeneProof Borrelia PCR Kit IVD (GeneProof, Brno, Czech Republic) with the following PCR conditions: initial denaturation at 95°C for 5 min followed by 35 cycles of denaturation at 95°C for 30 s, annealing at 52°C for 30 s, elongation at 72°C for 80 s, and a final elongation at 72°C for 7 min. The second round of PCR included 35 cycles of denaturation at 95°C for 20 s, followed by annealing at 55°C for 20 s, and elongation at 72°C for 60 s. Amplification was visualized on 1.5% agarose gel and, if positive, products were commercially sequenced and analyzed using MEGA ver.11 [29].
Among 7 patients with LNB included in the study, three were classified as confirmed and four as possible LNB based on the combination of clinical and diagnostics results described previously [6].
Autoimmune encephalitis
The study group included previously described subjects tested for the presence of AE autoantibodies in CSF: NMDAR, contactin-associated protein 2 (CASPR2), glutamate receptors (type AMPA1/2), leucine-rich glioma-inactivated protein 1 (LGI1), dipeptidyl aminopeptidase-like protein 6 (DPPX) and GABA B receptor [30]. Antibodies were identified using the Autoimmune Encephalitis Mosaic 6 diagnostic kit (Euroimmun, Germany) supported by the Nikon Eclipse 80i (Nikon, Japan) microscope, employed to read fluorescence under the magnifications of ×20 and ×40.
Autoimmune-triggered encephalitis was confirmed in 6 patients. In 5 (83.33%) of them, antibodies against NMDAR were detected in CSF, whereas one had anti-GABA.
Multiple sclerosis and control patients
Eighty-three patients admitted to the hospital with initial diagnosis of MS after further examination were divided into two groups: patients with confirmed MS and the control group defined as subjects without CNS inflammation. MS patients were diagnosed according to the revised McDonald criteria introduced in 2017 [31], with lumbar puncture being performed as part of their routine diagnostics.
Eight patients were diagnosed with MS and 10 were classified as controls in the study. Among control patients, one remained undiagnosed, while 4 cases had peripheral neuropathy, 3 had peripheral vertigo, and 2 patients had retinopathy.
CXCL13 measurements
CXCL13 in CSF was measured according to the instructions provided by the manufacturer using CXCL13 ELISA (Euroimmun, Lübeck, Germany). Optical density (OD) was analyzed on a Multiskan FC (Thermo Fisher Scientific, Waltham, MA, USA) photometer. Based on the manufacturer’s recommendations, the following levels of CXCL13-CSF corresponded to a specific interpretation: < 20 pg/ml – normal values, values from 20 to 29 pg/ml – borderline range, values 30– 100 pg/ml – elevated, and >100 pg/ml – LNB if corresponding clinical symptoms are present. Statistical comparisons between groups were performed using analysis of variance (ANOVA), while potential correlations were evaluated using Pearson’s test.
Results
Overall, 52 patients were included in the study, consisting of 18 women and 34 men with a mean age of 39 years. Subjects were divided into two major groups: patients with neuroinflammation (42 patients) and controls – 10 subjects without neuroinflammation, neuroinfection, or demyelination.
Among 42 cases of patients with neuroinflammation, 21 were classified as viral encephalitis; in 17 (81%) and in 4 (19%), the causative agent of inflammation was determined to be HSV and EV, respectively. Viral loads of HSV in CSF ranged from 60 to 341 copies per milliliter and were higher than those found for EV (12–60 copies/ml) (Table I). In 1 patient with confirmed LNB, EV was detected with viral load of 220 copies/ml.
Table I
Clinical and laboratory data in patients with viral encephalitis
Among all analyzed subgroups, LNB patients had the highest mean values of cytosis (116 cells/µl) and protein (102 mg/dl) in CSF, as well as the percentage of detected lymphocytes (93%). Based on routine CSF analysis, the mean cytosis was 7 and 2 cells/µl in the MS group and controls, respectively.
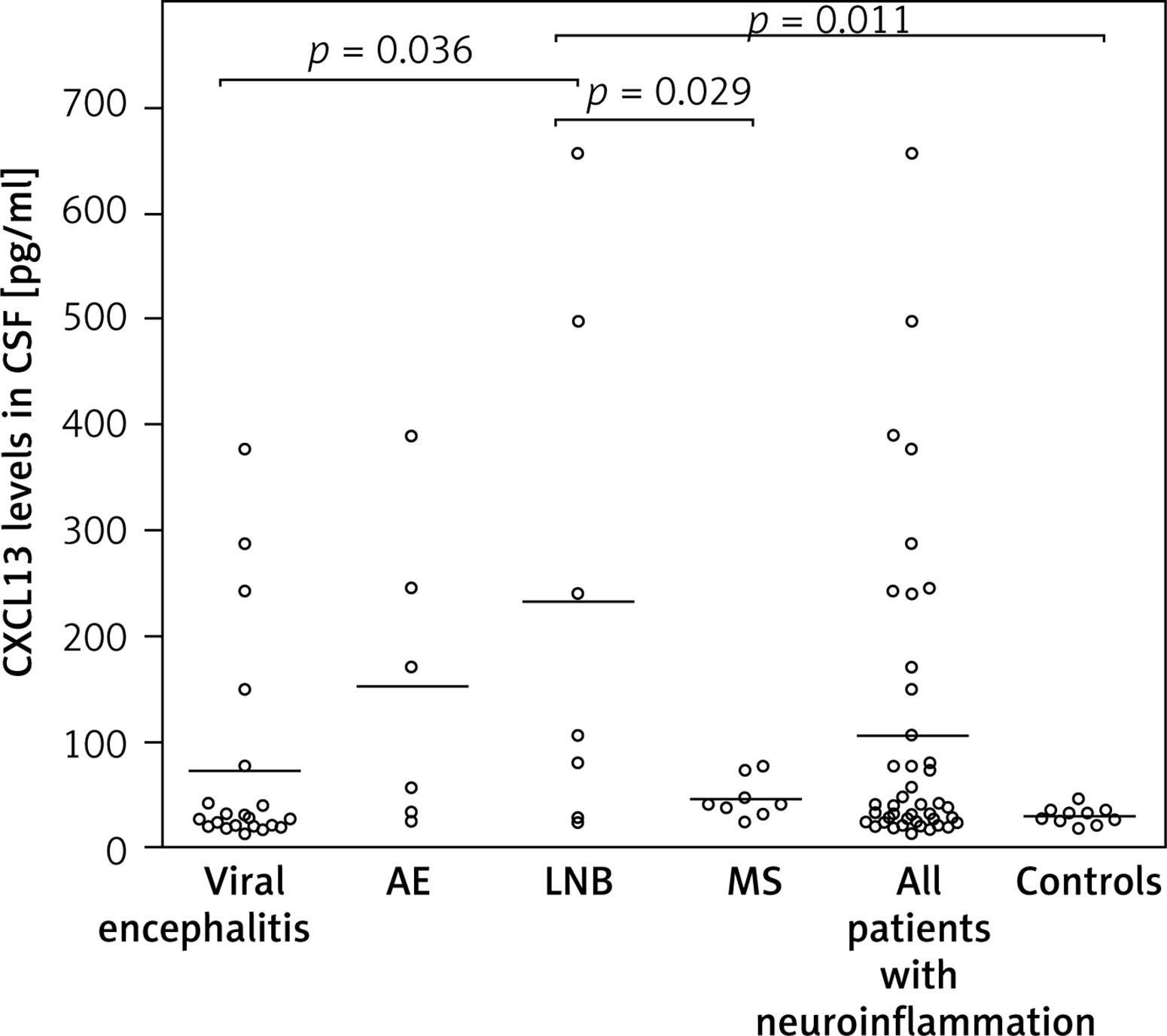
Patients with neuroinflammation had a mean level of CXCL13-CSF of 105 pg/ml compared to a value of 29 pg/ml in controls (Table I). The highest mean level of CXCL13 in CSF was detected in LNB patients (233 pg/ml), followed by AE (153 pg/ml), viral encephalitis cases (72 pg/ml), patients with MS (46 pg/ml), and controls (29 pg/ml).
The threshold criterion of > 100 pg/ml for the chemokine in CSF was met for four LNB and viral encephalitis patients each, as well as in three AE cases. Significant (p < 0.05) upregulation of CXCL13-CSF levels in LNB patients was observed in comparison to viral encephalitis and MS patients as well as controls (Figure 1).
Figure 1
Concentration of CXCL13 in CSF (pg/ml) in patients with neuroinflammation (n = 42) and controls (10 subjects without neuroinflammation). Patients were divided into the following groups: viral encephalitis (n = 21), autoimmune encephalitis (AE; n = 6), Lyme neuroborreliosis (LNB; n = 7), and multiple sclerosis (MS; n = 8) cases. ANOVA (p = 0.0093) was used to analyze the differences between the groups, and all significant results are shown (p < 0.05 in Tukey-Kramer test). Horizontal lines indicate mean CXCL13-CSF levels in each group
A positive correlation between elevated chemokine levels and cell count in CSF was found in all patients (r = 0.6496; p < 0.0001), as well as in the LNB group when tested alone (r = 0.8428; p = 0.0173). Similar results were obtained when CXCL13 levels were analyzed together with CSF protein levels. A positive correlation was observed in all patients (r = 0.7216; p < 0.0001), and separately in LNB (r = 0.8573; p = 0.0137) and AE patients (r = 0.8885; p = 0.0180) (Table I).
Discussion
CXCL13, previously known as B cell attracting chemokine 1 (BCA-1) [32] is constitutively expressed by dendritic cells (DC), monocytes, macrophages, and stromal cells in secondary lymphoid organs such as spleen, lymph nodes, and Peyer’s patches [33, 34]. The chemokine acts via the cognate CXCR5 receptor (Burkitt’s lymphoma receptor; CD185), which is expressed on mature B lymphocytes, DC, and T follicular helper cells (Tfh) [35]. CXCL13 plays a primary role in the development and organization of lymphoid tissues, as it regulates migrations of B cells and subsets of T cells to lymphoid follicles [36]. Furthermore, the CXCL13/CXCR5 axis seems to play a role in the formation of ectopic lymphoid tissues within the CNS, and therefore it is involved in the development of neuroinflammation [10].
In the present study we analyzed the CXCL13-CSF level in patients with viral and autoimmune encephalitis, as well as in those with LNB and MS in whom they were previously reported to be elevated, to verify its diagnostic utility for these types of neuroinflammation.
The highest chemokine levels in CSF have been detected in LNB patients but widely ranged from 23 to 657 pg/ml. Although elevated, CXCL13-CSF concentrations found in our study were lower than those described for untreated acute LNB (mean value of 15,149 pg/ml) [37] or observed by Erhart et al., where the median CXCL13 level was 3,920 pg/ml [38]. The most likely explanation is that CXCL13 levels are high when tested immediately after sample collection and they decrease with the CSF storage time [22, 37].
Although higher CXCL13-CSF mean concentrations were found in 42 patients with neuroinflammation compared to controls, the difference was not significant. However, significant differences in CXCL13-CSF levels were observed between LNB patients and controls, MS patients, and viral encephalitis patients. Our data are consistent with the results published by other research groups [37, 39–41], and confirm the utility of CXCL13-CSF testing as a valuable biomarker of LNB. Our results also support the claim that CXCL13-CSF can be helpful to differentiate LNB from other types of neuroinflammation, at the same time showing that its upregulation cannot be ruled out in case of single encephalitis patients [38]. Furthermore, we observed that the CSF chemokine levels were above recommended thresholds in 19% and 50% of viral and autoimmune encephalitis cases, respectively.
Viral encephalitis subjects included in the study encompassed patients with confirmed HSV and EV neuroinfection. Only a few previous studies have analyzed CXCL13-CSF in viral encephalitis cases separately; most have instead combined viral and bacterial cases together as “infectious encephalitis” [42].
Current data on CXCL13 activity in CNS in viral encephalitis are inconsistent. In our study, CXCL13-CSF levels did not significantly differ from controls. In contrast, Smíšková et al. reported that median CSF levels of the chemokine were significantly higher in patients with viral encephalitis, including HSV, EV, and tick-borne encephalitis (TBE) cases, compared to controls [43]. In another study, significantly higher CXCL13-CSF levels were also reported in patients with encephalitis caused by HSV and varicella zoster virus (VZV) than in controls consisting of subjects with non-inflammatory neurological diseases [38]. In contrast, viral encephalitis patients infected by human herpesvirus 6, VZV, EV, and HSV were found to have similar CXCL13-CSF levels as controls [44].
A high proportion (50%) of AE patients had CXCL13-CSF upregulation; however, chemokine concentrations did not significantly differ from those in controls, which could be explained by the small AE sample size used in the study. In one of the largest retrospective studies (conducted on 167 patients with anti-NMDAR encephalitis), elevated (p < 0.001) CXCL13 levels in CSF were reported when compared to 25 patients with non-inflammatory disorders [45]. Significant upregulation was also described by Kothur et al. in pediatric patients with anti-NMDAR encephalitis, acute disseminated encephalomyelitis (ADEM), or EV encephalitis in comparison to 20 non-inflammatory neurological controls mostly consisting of cases with cerebral palsy monogenic movement disorders [46]. It was found that CXCL13 levels in CSF were the highest at an early stage of anti-NMDAR encephalitis and they gradually decreased over time, which could explain the outcome of our investigation, as some of our patients had chronic AE [47].
Although specific diagnostic patterns were not identified in our study, the previously reported characteristic changes of CXCL13-CSF levels in autoimmune and viral encephalitis may indicate a meaningful marker of CNS immune activation, still warranting continued research [46, 48]. In AE, this could help identify patients experiencing immunologically active phases of disease and potentially guide decisions regarding immunotherapy [9, 49]. Similarly, in viral encephalitis, early CXCL13 increase in serum/CSF may assist in confirming a robust inflammatory response and help monitor the resolution of infection, though the overlap in levels across conditions underscores the need for cautious interpretation and combination with other diagnostic modalities [50, 51].
Finally, in our study have observed a strong positive correlation between pleocytosis and CXCL13-CSF levels, both in LNB patients and in all analyzed patients with neuroinflammation, which is similar to other data [38, 43, 44]. No such association was present in viral and autoimmune encephalitis, while these were reported in some other studies [38, 48]. On the other hand, a positive correlation was found between CXCL13 and protein levels in CSF when all patients were analyzed, as well as in LNB and AE cases separately. This correlation was reported in the past in relation to LNB; however, to our knowledge, there have been no such reports for AE [12].
The major limitation of the study is the relatively small study group. However, all analyzed patients are clinically well defined and represent diverse types of different neuroinflammation. A strength of the study is the well-selected control group, which includes a comprehensive set of general CSF analysis results. The small sample size also makes it challenging to reliably interpret CXCL13 levels in CSF, especially given the lack of disease specificity, absence of standardized cut-off values, variability in testing methods, and overlap with other neuroinflammatory or non-inflammatory conditions [22, 38, 52]. Addressing these limitations in the future will require larger studies and efforts to standardize assays and diagnostic thresholds.
In conclusion, we have confirmed the utility of CXCL13 measurements in CSF for LNB diagnosis. No specific patterns in CXCL13-CSF levels were associated with viral and autoimmune encephalitis. Nevertheless, CXCL13-CSF upregulation cannot be excluded in individual cases. Therefore the parameter should be used with caution and only as a supplementary diagnostic marker.