Introduction
Biliary diseases, primarily gallstone disease (GSD), are common digestive surgical conditions [1]. GSD, the most prevalent digestive system disease requiring hospitalization, has a prevalence rate of 10–15% among adults in Western countries [2, 3]. The standard treatment for GSD and some functional biliary disorders is laparoscopic cholecystectomy [4]. Although this procedure is highly advanced, some patients still experience gastrointestinal discomfort, recurrence of gallstones, and other symptoms after surgery, significantly impacting their quality of life [5]. Furthermore, if GSD is not adequately managed and treated promptly, it can lead to life-threatening complications such as cholecystitis, cholangitis, and pancreatitis [6]. Numerous studies suggest that, while current treatment technologies for GSD may have reached a peak, the global incidence of GSD continues to rise, necessitating a focus on developing new preventive strategies [6, 7]. Thus, enhancing the prevention and screening of GSD and other biliary diseases is of paramount importance.
Physical activity (PA) offers numerous physiological and psychological benefits [8]. Studies have shown that PA plays a crucial role in the prevention and management of various diseases, such as preventing gynecological tumors, improving rheumatoid arthritis symptoms, and promoting brain development in children [9–11]. GSD is influenced by both genetic and environmental factors and is caused by abnormal transport of cholesterol-saturated bile [12]. The flow of bile is closely related to the liver, biliary tract, and pancreas, and PA can impact the hepato-biliary-intestinal axis, aiding in bile metabolism in the liver and biliary system [13]. Regular PA and a balanced diet are key to preventing GSD, as supported by numerous studies [14]. For instance, Storti et al. found that women with low levels of PA have a 59% higher risk of GSD compared to those with high levels of PA [15]. Qian et al. proposed a negative causal relationship between PA measured by accelerometers and the risk of GSD [16]. However, these studies often focus on the duration of PA rather than its type. In the fast-paced modern society, high work intensity and rapid living rhythms have led to increased risks of chronic diseases. Many people lack sufficient time for PA and can only engage in activities on weekends. According to the latest U.S. PA guidelines, physical exercise can be categorized into “weekend warrior” (engaging in exercise less than three times a week with ≥ 75 min of vigorous exercise or ≥ 150 min of moderate-intensity exercise) and “regular exerciser” (engaging in exercise three or more times a week with ≥ 75 min of vigorous exercise or ≥ 150 min of moderate-intensity exercise) [17]. Researchers have already conducted studies on these types of exercises for certain diseases, finding that both weekend warrior and regular exercise significantly reduce the risk of cardiovascular disease and depression [18, 19]. We aimed to explore the optimal type, intensity, frequency, and duration of PA for reducing the risk of GSD, providing personalized preventive guidance for individuals.
Mendelian randomization (MR) is an emerging method for conducting causal analyses between exposure and outcome using genome-wide association studies (GWAS) data. It relies on the principle that genetic variations determine phenotypes, employing single nucleotide polymorphisms (SNPs) that are highly correlated with the exposure as instrumental variables (IVs) to perform unidirectional causal analysis from exposure to outcome [20]. MR must satisfy three conditions: (1) the IVs are closely related to the exposure; (2) the IVs are independent of confounding factors; (3) the IVs influence the outcome only through the exposure [21]. The NHANES is an ongoing large-scale cohort population database that provides a nationally representative dataset widely used in epidemiological research [22]. Conducted on a biennial cycle, NHANES includes comprehensive demographic data, physical examinations, laboratory tests, and questionnaire information. We can utilize this dataset to obtain information on individuals’ PA patterns, GSD risk, and cholecystectomy risk, enabling effective and reliable correlation analysis results.
Our study combined two-sample MR analysis with NHANES (2017–2020.3) analysis to explore the potential association between PA and the risk of GSD from both cross-sectional and causal perspectives. To achieve more accurate biliary disease indicators, we included cholecystectomy and biliary diseases as supplements to GSD risk and examined their causal relationship with PA. Additionally, we incorporated different PA patterns into our study, aiming to elucidate the relationships between PA patterns and GSD, as well as cholecystectomy. This research may provide new insights into the prevention and management of GSD and other biliary diseases, and help the general population develop personalized GSD prevention strategies.
Material and methods
Obtaining GWAS data for two-sample MR
To evaluate the causal relationship between PA and the risks of GSD, cholecystectomy, and biliary diseases, we obtained SNPs related to PA from the set “vigorous exercise in the past 4 weeks” as the exposure. For the outcome, we obtained SNPs associated with the risk of GSD from the sets “cholelithiasis or gallstones”, “cholecystectomy”, and “Disorders of gallbladder, biliary tract and pancreas”. and included SNPs related to “gallstones” from the UK Biobank (UKB) database as a cross-validation. All data participants were of the same ethnicity and included both males and females, with detailed information available in Supplementary Table SI.
Due to the limited number of exposure-related SNPs when using a threshold of p < 5 × 10–8, which could lead to low statistical power and bias from weak instrumental variables, we used a threshold of p < 5 × 10–6. This is also a widely used and accepted standard threshold in MR studies [23]. Subsequently, we applied a linkage disequilibrium (LD) clumping criterion of r2 < 0.001 and kb = 10,000 to eliminate LD effects. PhenoScanner was used to remove SNPs associated with GSD risk factors, and the “harmonise_data” function was employed to align effect alleles for exposure and outcome, removing palindromic SNPs and those incompatible with the outcome. In addition, the F statistic is a key measure for assessing the strength of the association between SNPs and the exposure, and is used to identify strong IVs and avoid weak instrument bias. We calculated the F statistics for the IVs and excluded any SNPs with F values less than 10 [24].
Methods and sensitivity tests for MR
The research methods for the MR analysis adhere to the STROBE-MR checklist, as detailed in Supplementary Figure S5. In the two-sample MR analysis, we used IVW as the primary method, with MR-Egger and the weighted median as complementary methods. To enhance the reliability of our analysis results, we conducted rigorous sensitivity tests. Heterogeneity was tested using Cochran’s Q, applying random-effects IVW in the presence of heterogeneity and fixed-effects IVW otherwise. Both MR-Egger and MR-PRESSO were used to test for horizontal pleiotropy, and their results were cross-validated to obtain the most accurate outcomes. MR-PRESSO also provided outlier and distortion tests, helping to eliminate outlier SNPs and achieve more accurate MR results after removing outliers. Additionally, we performed leave-one-out analysis and funnel plot tests to examine whether individual SNPs introduced bias into the MR results.
Participants in the cross-sectional study
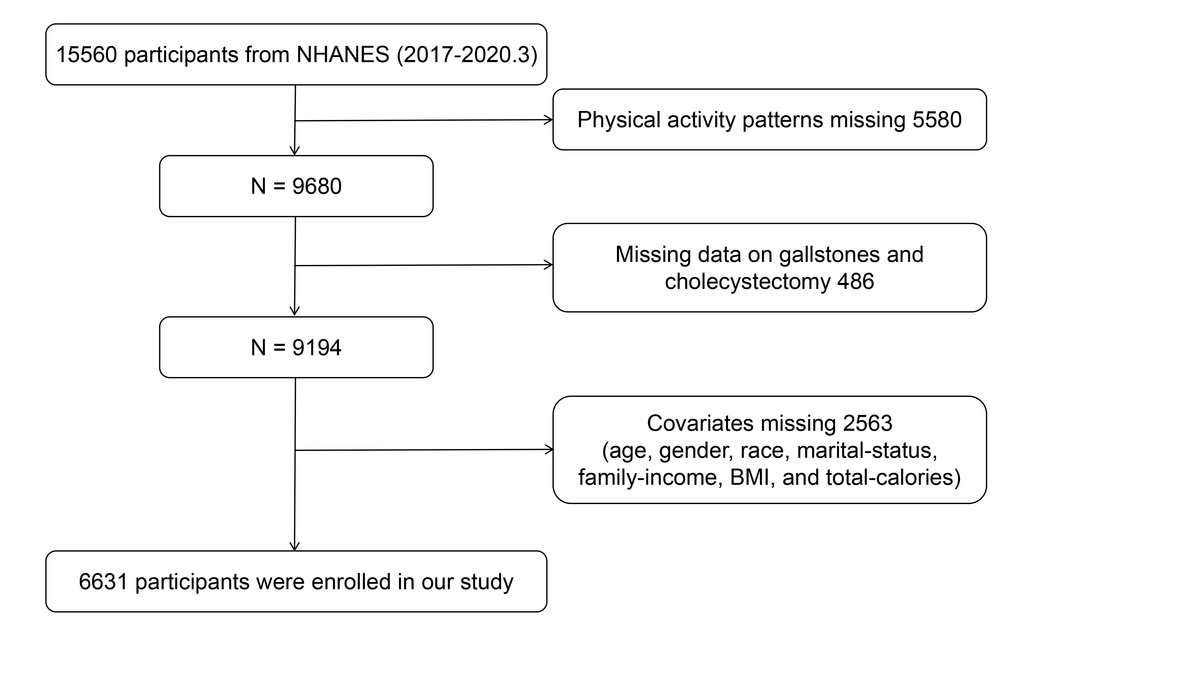
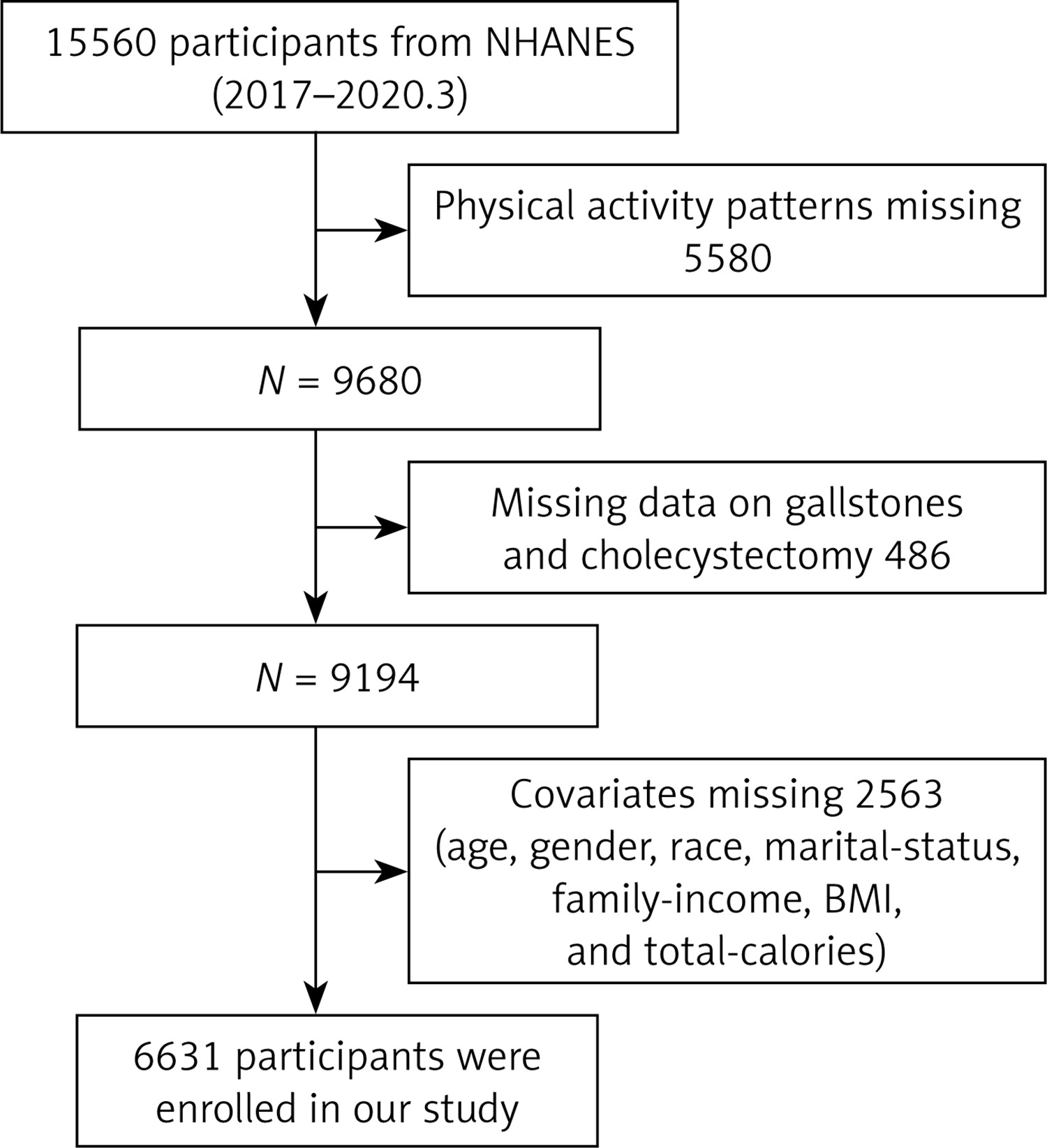
To validate the results of the MR analysis and assess the impact of different PA patterns on biliary health, we conducted a cross-sectional study. We used the presence of GSD and history of cholecystectomy as measures of biliary disease risk, including 15,560 participants from the NHANES (2017–2020) cycle. All participants signed informed consent forms from NCHS, ensuring no ethical issues. The inclusion criteria were as follows: (1) exclude participants with missing PA data (n = 5580); (2) exclude participants with missing data on GSD and cholecystectomy (n = 486); (3) exclude participants with missing covariate data on age, sex, race, marital status, poverty income ratio (PIR), BMI, and total calorie intake (n = 2563). Finally, 6631 participants were included in this study. Detailed selection steps are shown in Figure 1.
PA patterns, GSD, and cholecystectomy status
In NHANES, PA is assessed using the Global Physical Activity Questionnaire (GPAQ), which defines vigorous activities as those causing a significant increase in breathing or heart rate for at least 10 min per week (e.g., continuous running, basketball), and moderate-intensity activities as those causing a slight increase in breathing or heart rate for at least 10 min per week (e.g., brisk walking, cycling, swimming, volleyball). According to the latest PA guidelines, 1 min of vigorous activity is considered equivalent to 2 min of moderate-intensity activity. We integrated frequency (number of times per week) and duration (duration per session) using the formula “2 * vigorous activity + moderate-intensity activity” to calculate total PA time (minutes per week). Following the U.S. PA guidelines, PA was categorized into four patterns: 1. Inactive – total PA time of 0 min per week; 2. Insufficiently active – total PA time < 150 min per week; 3. Weekend warrior – active 1 or 2 times per week with total PA time ≥ 150 min; 4. Regular exerciser – active more than 2 times per week with total PA time ≥ 150 min.
Data on GSD status were obtained from participants over 20 years old, who were asked during interviews whether a doctor or other health professional had ever told them they had gallstones. Answering “yes” defined them as having gallstones, while “no” defined them as not having gallstones. Data on cholecystectomy status were also collected from participants over 20 years old, asking them the age at which they first underwent gallbladder removal surgery. Participants reporting a valid age (between 20 and 150) were classified as having undergone cholecystectomy, while ages outside this range were treated as indicating no history of cholecystectomy.
Covariates
To eliminate the influence of confounding factors, we included covariates such as age (≥ 60 years, < 60 years), sex, race (Mexican American, non-Hispanic White, non-Hispanic Black, other races), marital status (cohabitating or married, single), PIR (PIR ≥ 1, PIR < 1), BMI (underweight < 18.5, normal and overweight ≥ 18.5), and total calorie intake.
Correlation between PA patterns and the risk of GSD and cholecystectomy
In the NHANES data analysis, we treated GSD status and cholecystectomy status as binary categorical variables and used survey-weighted logistic regression to assess the correlation between different PA patterns and the risks of GSD and cholecystectomy. We designed two models: Model 1 with no covariate adjustments, and Model 2 adjusted for age, sex, race/ethnicity, income, marital status, BMI, and total calorie intake. Restricted cubic splines (RCS) were used to evaluate potential nonlinear relationships between total weekly PA duration (minutes) and weekly PA frequency (days) with the risks of GSD and cholecystectomy. Additionally, we explored potential interactions between different PA patterns and covariates.
Statistical analysis
All statistical analyses were conducted using R version 4.2.2. A two-tailed test was used for p-values, with p < 0.05 considered significant. The independent samples t-test was used for continuous variables with normal distribution, and Spearman correlation analysis was used for the correlation of continuous variables.
Results
Correlation between PA and biliary health in MR analysis
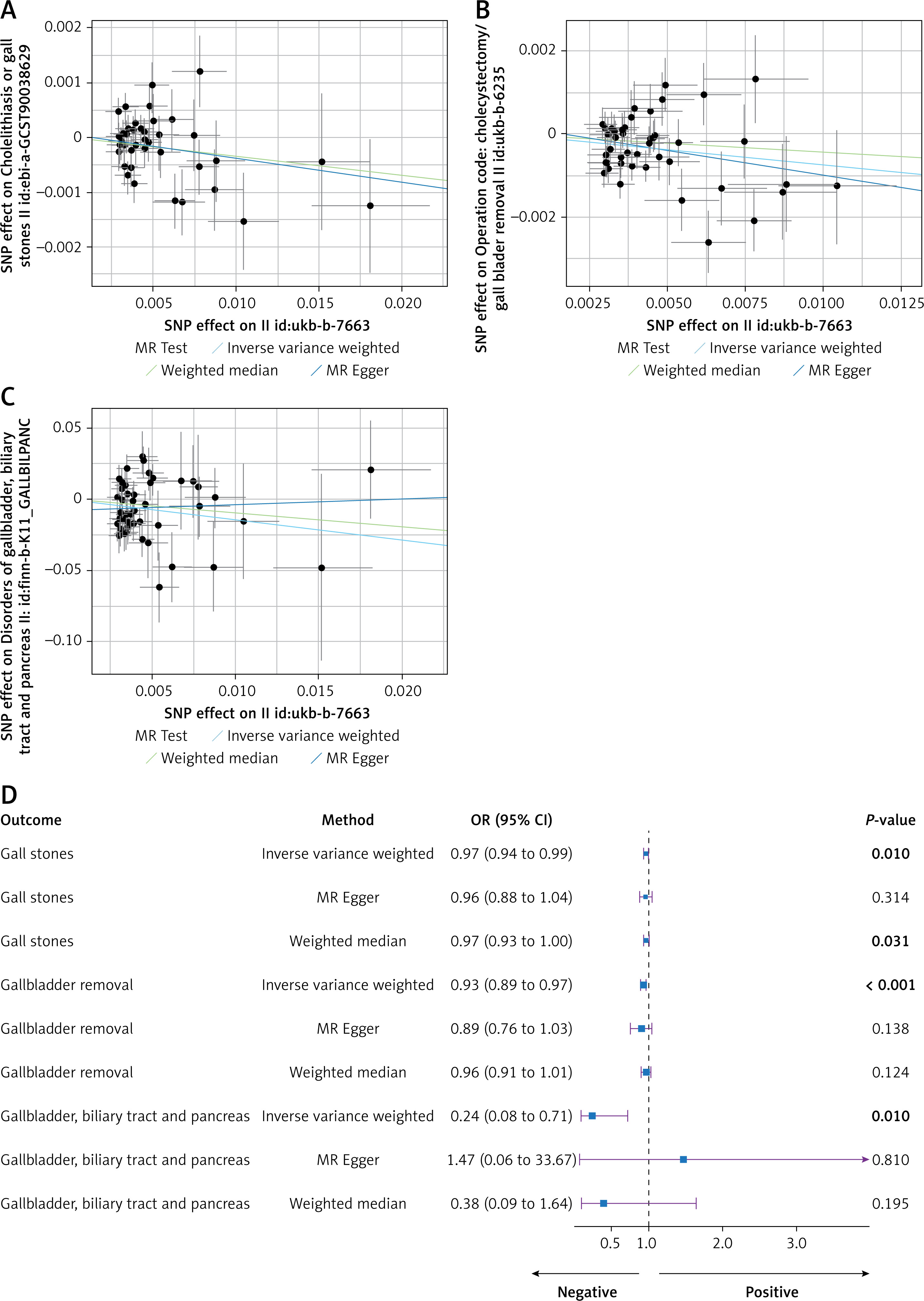
We conducted a two-sample MR analysis using GWAS data on PA and biliary health. The results showed a significant causal relationship between PA and GSD (OR = 0.97, 95% CI = 0.94–0.99, p = 0.01), cholecystectomy (OR = 0.93, 95% CI = 0.89–0.97, p < 0.001), and gallbladder/biliary/pancreatic diseases (OR = 0.24, 95% CI = 0.08–0.71, p = 0.01) (Figure 2 D). Notably, the odds ratios (OR) for all three outcomes were < 1, indicating that PA is a protective factor for biliary diseases and that the risk of these conditions may decrease with increased PA (Figures 2 A–C). In addition, the analysis of UKB gallstones data yielded consistent results (OR = 0.95, 95% CI = 0.92–0.98, p = 0.001) (Supplementary Figures S1 A, B).
Figure 2
Scatter and forest plots of MR analysis: A – Scatter plot of the relationship between PA and gallstones. B – Scatter plot of the relationship between PA and cholecystectomy. C – Scatter plot of the relationship between PA and gallbladder/biliary/pancreatic diseases. D – Forest plot of the two-sample MR analysis for PA and the risks of gallstones, cholecystectomy, and gallbladder/biliary/pancreatic diseases. P < 0.05 is highlighted in bold
Sensitivity tests in MR analysis
To assess the reliability of the causal relationships, we conducted a series of sensitivity tests. The p-values from Cochran’s Q test for IVW (p-gallstones = 0.067, p-cholecystectomy = 0.071, p-gallbladder/biliary/pancreatic diseases = 0.079) indicated no heterogeneity. The heterogeneity p-value for UKB gallstones data was 0.043, indicating the presence of heterogeneity. Therefore, we applied the random-effects IVW method to ensure the accuracy of the results. MR-PRESSO did not reveal evidence of intercept presence (p-gallstones = 0.828, p-cholecystectomy = 0.575, p-gallbladder/biliary/pancreatic diseases = 0.232, p-UKB gallstones = 0.860), and MR-pleiotropy detected no pleiotropy (p-gallstones = 0.091, p-cholecystectomy = 0.091, p-gallbladder/biliary/pancreatic diseases = 0.092, p-UKB gallstones = 0.077) (Supplementary Table SII). The leave-one-out analysis did not identify any single SNP that might bias the results. Additionally, the funnel plots were symmetrical (Supplementary Figures S1 C, D, S2).
Participants from NHANES
As shown in Table I, all participants were categorized into two groups: those with GSD and those without GSD. Among individuals with GSD, there was a higher proportion of those over 60 years old, females, and non-Hispanic Whites. Their total calorie intake was lower, and their total PA duration and PA frequency per week were significantly lower than those of non-GSD participants. Interestingly, the proportion of cholecystectomy among GSD patients was as high as 78%, compared to only 3.7% among non-GSD patients. Additionally, there were significant differences in the four PA patterns between the two groups. Compared to non-GSD participants, a higher proportion of individuals with GSD were inactive (53% vs. 43%) or insufficiently active (17% vs. 15%), while a lower proportion were weekend warriors (1.8% vs. 4.1%) or regular exercisers (28% vs. 37%), suggesting a potential correlation between PA and the development of GSD. Notably, the most significant difference between GSD and non-GSD participants was in the proportion of weekend warriors, indicating that weekend exercise may have an important impact on the incidence of GSD.
Table I
Basic information of the included population, classified by gallstone and non-gallstone
| Characteristic | Gallstone | P-value2 | |
|---|---|---|---|
| No, N = 5909 (89%)1 | Yes, N = 722 (11%)1 | ||
| Age group | < 0.001 | ||
| < 60 | 3,895 (73%) | 355 (50%) | |
| ≥ 60 | 2,014 (27%) | 367 (50%) | |
| Sex | < 0.001 | ||
| Female | 2,906 (49%) | 519 (73%) | |
| Male | 3,003 (51%) | 203 (27%) | |
| Race | 0.027 | ||
| Mexican American | 662 (8.3%) | 82 (6.7%) | |
| Other | 1,510 (17%) | 177 (18%) | |
| Non-Hispanic white | 2,157 (63%) | 322 (68%) | |
| Non-Hispanic black | 1,580 (11%) | 141 (7.2%) | |
| PIR | 0.8 | ||
| < 1 | 1,118 (13%) | 121 (13%) | |
| ≥ 1 | 4,791 (87%) | 601 (87%) | |
| Marital status | 0.5 | ||
| Living alone | 2,452 (37%) | 295 (39%) | |
| Married or living with partner | 3,457 (63%) | 427 (61%) | |
| BMI group | 0.085 | ||
| Normal and overweight | 5,646 (95%) | 706 (98%) | |
| Underweight | 263 (4.9%) | 16 (2.2%) | |
| Total calories | 1,958 (1,506, 2,544) | 1,786 (1,374, 2,315) | < 0.001 |
| PA duration [min] | 75 (0, 360) | 0 (0, 180) | < 0.001 |
| PA frequency [days] | 2.00 (0.00, 5.00) | 0.00 (0.00, 4.00) | < 0.001 |
| PA type | 0.002 | ||
| Inactive | 3,026 (43%) | 439 (53%) | |
| Insufficiently active | 842 (15%) | 102 (17%) | |
| Weekend warrior | 215 (4.1%) | 15 (1.8%) | |
| Regular exercise | 1,826 (37%) | 166 (28%) | |
| Surgery | 199 (3.7%) | 539 (78%) | < 0.001 |
Risk of GSD
We used adjusted survey-weighted logistic regression to assess the relationship between different PA patterns and the risk of GSD. Using inactive as the reference, the results show that weekend warrior (OR = 0.57, 95% CI = 0.35–0.94, p = 0.03) and regular exercise (OR = 0.74, 95% CI = 0.56–1.00, p = 0.047) were significantly negatively associated with GSD risk (Table II). Using regular exercise as the reference, inactive (OR = 1.34, 95% CI = 1.01–1.79, p = 0.047) showed a significant positive association with GSD risk, while weekend warrior (OR = 0.77, 95% CI = 0.43–1.37, p = 0.3) showed no significant association with GSD risk (Table III). This indicates that both weekend warrior and regular exercise can significantly reduce the risk of GSD, and there appears to be no substantial difference between the two PA patterns in terms of risk reduction. However, compared to regular exercise, inactive is associated with a significantly increased risk of GSD.
Table II
Associations between types of PA and GSD risk, using inactivity as the reference
| Characteristic | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR1 | 95% CI1 | P-value | OR1 | 95% CI1 | P-value | |
| PA type | ||||||
| Inactive | – | – | – | – | ||
| Insufficiently active | 0.90 | 0.65, 1.25 | 0.5 | 0.94 | 0.67, 1.31 | 0.7 |
| Weekend warrior | 0.36 | 0.22, 0.60 | < 0.001 | 0.57 | 0.35, 0.94 | 0.030 |
| Regular exercise | 0.61 | 0.45, 0.83 | 0.003 | 0.74 | 0.56, 1.0 | 0.047 |
Table III
Associations between types of PA and GSD risk, using regular exercise as the reference
| Characteristic | Model 1 | Model 2 | ||||
|---|---|---|---|---|---|---|
| OR1 | 95% CI1 | P-value | OR1 | 95% CI1 | P-value | |
| PA type | ||||||
| Regular exercise | – | – | – | – | ||
| Inactive | 1.63 | 1.20, 2.21 | 0.003 | 1.34 | 1.01, 1.79 | 0.047 |
| Insufficiently active | 1.47 | 0.93, 2.32 | 0.10 | 1.26 | 0.79, 2.03 | 0.3 |
| Weekend warrior | 0.58 | 0.32, 1.08 | 0.085 | 0.77 | 0.43, 1.37 | 0.3 |
Risk of cholecystectomy
Similarly, we explored the relationship between PA patterns and the risk of cholecystectomy. Analysis using inactive as the reference showed that weekend warrior (OR = 0.51, 95% CI = 0.28–0.95, p = 0.036) and regular exercise (OR = 0.70, 95% CI = 0.59–0.82, p < 0.001) were significantly negatively associated with the risk of cholecystectomy (Supplementary Table SIII). Analysis using regular exercise as the reference showed that inactive (OR = 1.43, 95% CI = 1.21–1.69, p < 0.001) was significantly positively associated with the risk of cholecystectomy, while weekend warrior (OR = 0.73, 95% CI = 0.41–1.32, p = 0.3) showed no significant association with the risk of cholecystectomy (Supplementary Table SIV). We obtained consistent results with the analysis of GSD risk, further validating the inverse causal relationship between PA and biliary disease risk observed in the MR analysis.
Nonlinear relationship between PA duration, frequency, and biliary diseases
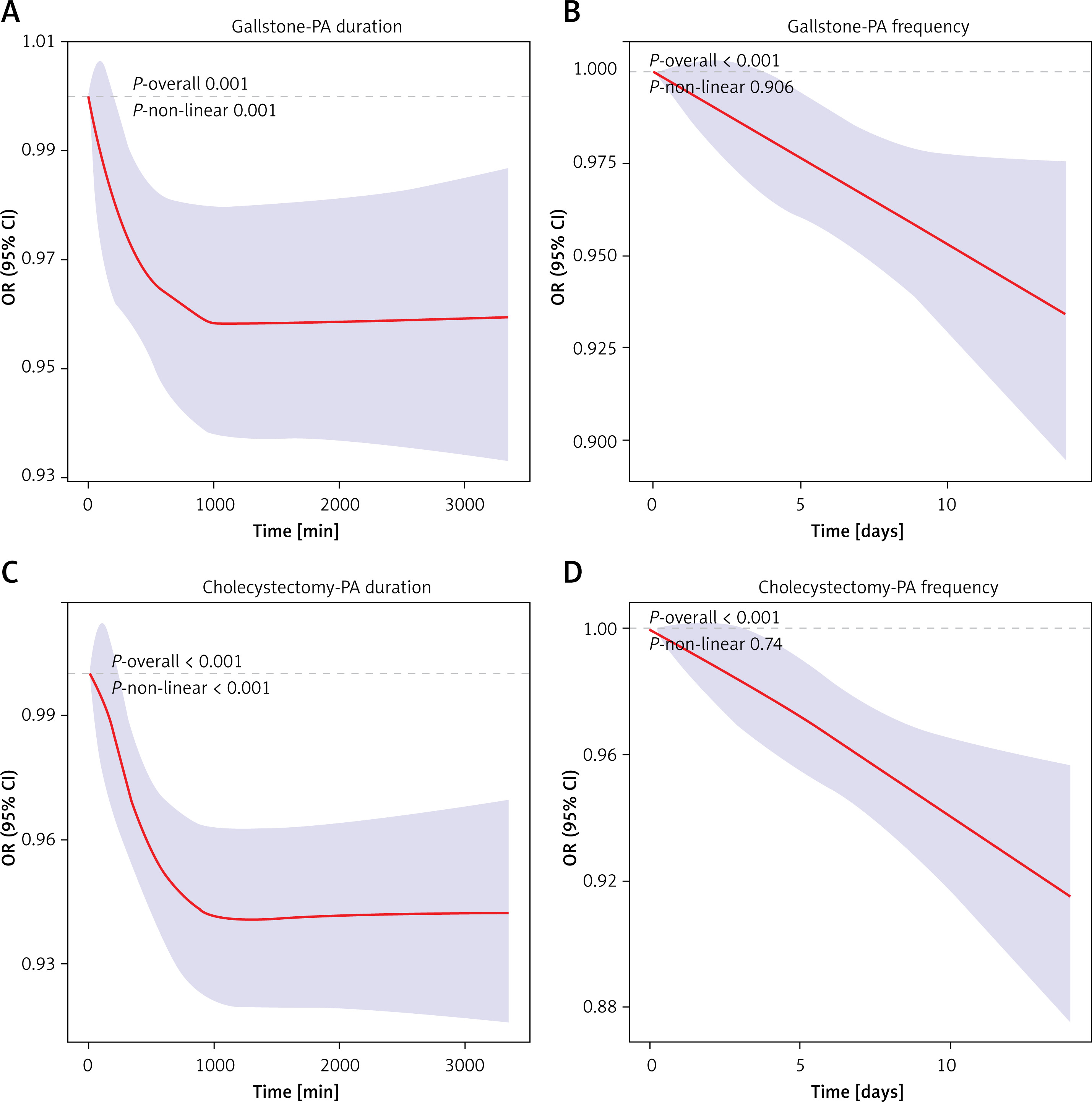
To further elucidate the impact of PA on biliary tract health, we employed RCS to explore the potential nonlinear relationships between weekly total PA duration, weekly PA frequency, and the risks of GSD incidence and cholecystectomy. The results indicate significant nonlinear relationships (P for non-linearity < 0.05) between weekly total PA duration and the risks of GSD and cholecystectomy. The odds ratios (ORs) for both outcomes decrease curvilinearly with increasing weekly total PA duration, approaching linearity after 1000 min per week (Figures 3 A, C). Conversely, weekly PA frequency shows a significant negative linear relationship (P for overall < 0.05) with both outcomes, where the corresponding ORs decrease linearly with increasing weekly PA days (Figures 3 B, D). This suggests that increasing the frequency of weekly PA may effectively reduce the risk of GSD. Increasing weekly PA duration has a similar effect, but its significant protective effect against GSD may diminish beyond 1000 min per week.
Figure 3
Nonlinear relationship between PA duration and frequency and GSD: A – RCS for weekly total PA time and GSD risk. B – RCS for weekly total PA days and GSD risk. C – RCS for weekly total PA time and cholecystectomy risk. D – RCS for weekly total PA days and cholecystectomy risk. P non-linear < 0.05 indicates a significant nonlinear relationship
Interaction between PA patterns and risk of GSD and cholecystectomy
To better assess the association between PA patterns and GSD, we conducted stratified interaction analyses considering age, sex, race, PIR, marital status, BMI, and total calorie intake. The results revealed interactions between weekend warrior with age and BMI, and regular exercise with total calorie intake, while no significant interactions were observed for other covariates (Supplementary Figure S3). Individuals with younger age and lower BMI engaging in weekend warrior, and those with higher total energy intake engaging in regular exercise, showed a more significant reduction in GSD risk. This suggests that younger individuals may effectively prevent GSD by exercising only on weekends, whereas those with higher energy intake need to exercise more frequently to effectively prevent GSD.
In the analysis of cholecystectomy risk, a significant interaction was observed only between weekend warrior and BMI. Individuals with lower BMI engaging in weekend warrior showed a more pronounced reduction in cholecystectomy risk, while no significant interactions were noted for other covariates (Supplementary Figure S4). This is similar to the findings for GSD risk, suggesting that the benefits of weekend warrior might be more pronounced in individuals with lower BMI, potentially due to their lower body weight and body fat. Further mechanistic studies and cohort research are needed to substantiate these observations.
Discussion
This study employed two-sample MR analysis to explore the causal relationships between PA and the risks of GSD, cholecystectomy, and biliary tract diseases. Additionally, we defined PA into four patterns (inactive, insufficiently active, weekend warrior, and regular exercise) and, for the first time, examined the effects of these PA patterns on GSD and cholecystectomy risks in a large NHANES cohort. Interestingly, compared to inactive and insufficiently active, both weekend warrior and regular exercise provided the same protective effects against GSD and cholecystectomy risks.
Given the close association between PA and the risks of GSD, cholecystectomy, and biliary tract diseases, many researchers have explored this area. Qian et al. identified a negative causal relationship between PA and GSD risk through MR analysis [16]. However, their study used PA measured by accelerometers as the exposure, which might have introduced bias due to instrument limitations. To achieve more accurate results, we used more comprehensive PA data, including vigorous exercise and heavy physical labor. We obtained consistent results, confirming the robust negative causal relationship between PA and GSD. Additionally, numerous researchers have found that PA can effectively reduce the risk of cholecystectomy [25, 26]. However, their studies were observational and could not establish causality. We validated the negative causal relationship between PA and cholecystectomy risk through two-sample MR analysis. Finally, to explore the relationship between PA and biliary health more comprehensively, we also included gallbladder/biliary/pancreatic diseases in our MR analysis. The results demonstrated negative causal relationships between PA and the risks of GSD, cholecystectomy, and biliary tract diseases, which were confirmed by rigorous sensitivity analyses. This suggests that increasing PA might be beneficial in the clinical management of individuals at risk for biliary tract diseases.
As modern lifestyles evolve, the weekend warrior pattern has increasingly become the preferred PA choice for many people [27]. Its benefits, such as reducing cardiovascular disease risk and visceral fat obesity, and extending lifespan, have been well documented [28–30]. However, previous studies have seldom focused on the impact of PA patterns on GSD risk. They primarily emphasized PA duration and found PA to be a protective factor against GSD [31]. We explored the relationship between PA patterns and GSD risk using survey-weighted logistic regression with NHANES data. The results show that both weekend warrior and regular exercise provide similar protective effects against GSD risk, even after adjusting for covariates. This suggests that, given a total PA time of over 150 min, the frequency of PA might not significantly impact GSD risk. To clarify the effects of total PA time and PA frequency on GSD risk, we analyzed the potential nonlinear relationships between weekly total PA time, weekly PA frequency, and GSD risk using RCS. The results indicated a significant nonlinear relationship between weekly total PA time and GSD risk, while a significant negative linear relationship was found between weekly PA frequency and GSD risk. Interestingly, the RCS curve for total PA time resembles an elbow plot: the OR for GSD decreases with increasing PA time until it smooths out after 1000 min per week. This suggests that when weekly PA time is less than 1000 min, the OR decreases with increased PA time, but this decreasing trend diminishes. Beyond 1000 min per week, additional PA time may not affect the OR significantly. We speculate that excessive PA might damage the liver and gallbladder, inhibiting hepatic cholesterol clearance [32, 33]. Combining these findings with the logistic regression results, we conclude that the weekend warrior approach can effectively prevent GSD without necessitating excessively long exercise durations. More observational and mechanistic studies are needed to further investigate the relationship between PA and GSD.
Cholecystectomy has long been the standard treatment for symptomatic GSD, providing timely and effective outcomes [34]. However, cholecystectomy carries significant risks. Studies have indicated that cholecystectomy may increase the risks of kidney cancer and non-alcoholic fatty liver disease (NAFLD), and it may be an independent risk factor for metabolic syndrome [35–37]. Therefore, cholecystectomy requires careful consideration. Our analysis of the relationship between PA patterns and cholecystectomy risk revealed that both weekend warrior and regular exercise significantly reduce the risk of cholecystectomy, consistent with the results of GSD analysis. We encourage people to maintain regular exercise habits to reduce unnecessary cholecystectomy procedures, which may help preserve biliary health.
GSD is a multifactorial condition, with increased incidence associated with age, sex, metabolic circulation, dyslipidemia, and insulin resistance [38]. Evidence suggests that metabolic syndrome can increase the risk of GSD, while high levels of PA can alleviate the inflammatory state in patients with metabolic syndrome, thereby providing protection against GSD [39, 40]. The impact of PA on hepatobiliary diseases has been extensively studied, with the primary mechanism likely involving cholecystokinin (CCK), a hormone released from the upper gastrointestinal tract [41]. Acute vigorous exercise can elevate CCK levels, enhancing gallbladder emptying and refilling by promoting smooth muscle contraction, which aids in the release of bile into the intestine and facilitates lipid digestion and absorption [42, 43]. Studies indicate that PA may improve bile acid excretion and circulation, promoting enterohepatic circulation, which dilutes bile cholesterol concentration and effectively prevents GSD [44, 45]. Additionally, regular PA can increase vagal tone, potentially triggering neurohormonal mechanisms of gallbladder emptying mediated by the vagus nerve before exercise [46, 47]. Thus, PA can effectively mitigate risk factors such as cholesterol accumulation in bile and gallbladder motility disorders, inhibiting the formation of biliary stones and reducing the risk of GSD.
In subgroup interaction analysis, we found interactions between weekend warrior and age and BMI, with younger age and lower BMI corresponding to better preventive effects. Additionally, individuals with higher energy intake who engage in regular exercise have a lower risk of GSD. Interestingly, due to work schedules, most individuals who exercise on weekends are under 60 years old. Our study may provide new guidance for young individuals with tight schedules on preventing GSD. On the other hand, obesity and overnutrition are risk factors for GSD, and lifestyle changes are fundamental to primary prevention [6]. However, the relationship between energy intake and GSD is not absolute. Studies have shown that low-calorie intake during weight loss increases the risk of GSD, and this risk is proportional to pre-weight-loss body weight and the rate of weight loss [48]. Long-term low-calorie intake can inhibit gallbladder contraction and emptying function, promoting GSD formation, necessitating regular intake of small amounts of high-calorie food to prevent GSD. It is important to note that rapid weight loss is not a typical condition, and such conclusions may only apply to specific populations. Therefore, we cannot yet clarify the association between PA patterns and BMI and diet. Further cohort studies and mechanistic research are needed to elucidate these potential relationships.
Our study explored the association between PA and GSD through MR analysis and validated the findings using NHANES data. We were the first to compare the differential effects of various PA patterns on the risks of GSD and cholecystectomy, identifying a significant role for weekend warrior pattern in preventing these conditions. Compared to previous studies, our research has several strengths: (1) It was an MR analysis, based on genetic variations, exploring associations between phenotypes without being affected by confounding factors or reverse causation. (2) The national representativeness of the NHANES database provides reliable analytical results. (3) We used two complementary analyses to validate each other and investigated the role of the weekend warrior pattern in GSD prevention. However, our study also has limitations. First, we used a p-value threshold of 5 × 10–6 for SNP selection, which may introduce potential bias. Second, we did not have access to GWAS data on PA patterns, so we could not verify the causal relationship between PA patterns and GSD, cholecystectomy, or other biliary diseases. Third, due to missing data for many covariates in the NHANES (2017–2020) cycle, despite our efforts to adjust for relevant confounding factors in the models, we cannot rule out the potential influence of unknown factors such as hyperlipidemia and metabolic syndrome. Fourth, we did not obtain precise data on gallbladder or bile duct stones (intra- or extrahepatic bile duct stones, common bile duct stones), which, although within the scope of GSD, have different specific diagnoses, clinical features, and treatments, possibly introducing bias. Fifth, since the NHANES analysis is observational in nature, further cohort studies are needed to confirm causality. Sixth, our study was limited to populations from the U.S. and Europe; therefore, additional studies involving other racial and ethnic groups are necessary to validate the broader applicability of our findings.
Through MR analysis and NHANES data analysis, we found a negative causal relationship between PA and GSD, with both weekend warrior and regular exercise effectively reducing the risk of GSD. Given the contemporary societal context, weekend warrior as a mode of PA is gradually becoming mainstream. Our findings provide reference and guidance for GSD prevention among the population.