A 51-year-old man presented to the rheumatology department with 30 years of progressive bilateral enlargement of the palms, forearms, and ankles and 10 years of limited knee motion. He had a previous history of diabetes mellitus and no family history of similar symptoms. On examination, finger and toe clubbing were observed (Figure 1 A). Restricted knee motion was observed on palpation, and enlargement of the forearms and lower legs was also observed. There was no hyperhidrosis or skin thickening. Radiographs of the forearm, knee and lower leg showed increased periosteal bone formation (Figures 1 B, C). Serum laboratory tests including thyroid function tests and echocardiogram were normal. Whole-body positron emission tomography-computed tomography showed osteophytes at multiple sites throughout the body showing increased FDG uptake changes (Figure 1 D). 99mTc-MDP bone scintigraphy was performed, which showed diffusely symmetrical increased tracer uptake in the large joint areas of the extremities, suggesting hypertrophic osteoarthropathy (Figure 1 E) [1]. The patient was diagnosed with hypertrophic osteoarthropathy, characterized by periosteal bone proliferation, clubbing, hyperhidrosis and facial skin thickening, in the absence of systemic disease. The patient was initially treated with nonsteroidal anti-inflammatory drugs for 1 week and an intra-articular injection of sodium hyaluronate into the knee. Subsequent follow-up was followed for symptom resolution.
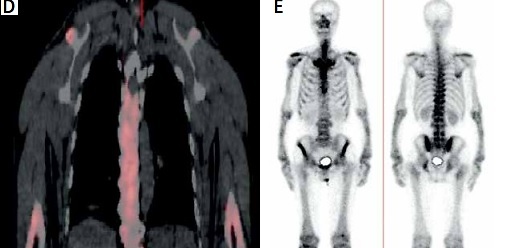
Figure 1
A – Finger clubbing. B, C – Radiographs of the forearm, knee and lower leg showed increased periosteal bone formation. D – Whole-body positron emission tomography-computed tomography showed increased FDG uptake changes. E – 99mTc-MDP bone scintigraphy showed diffusely symmetrical increased tracer uptake in the large joint areas of the extremities

Hypertrophic osteoarthropathy is a syndrome clinically characterized by abnormal skin and periosteal proliferation of the distal extremities [2]. Most cases of this disease are associated with neoplastic disease, most commonly lung cancer, while primary hypertrophic osteoarthropathy is a rare autosomal recessive inherited multisystemic disease [2]. The pathogenesis of the disease involves increased circulation to distal peripheries and the release of growth factors, leading to an increase in osteoblast activity and fibroblasts, which leads to a clinical triad of digital clubbing, usually distal and symmetrically distributed osteochondritis and arthritis [3, 4]. Treatment options for this disease include NSAIDs, bisphosphonates, and octreotide, which can be effective in treating bone pain [5]. In addition, trunk vagotomy has shown relief in refractory patients [6], and in some cases, aspiration of knee fluid and intra-articular injections for pain have been found to be effective.