Mantle cell lymphoma (MCL) accounts for approximately 6% of all non-Hodgkin lymphomas and represents a subtype of B-cell lymphoma associated with poor prognosis. Nearly all patients relapse after first-line chemotherapy [1, 2]. The introduction of Bruton’s tyrosine kinase (BTK) inhibitors has significantly improved outcomes in relapsed/refractory (r/r) MCL, with overall response rates (ORRs) of 68–80% and median progression-free survival (PFS) around 13 months overall and 25 months when used in the second line [3]. BTK inhibitors are now the standard of care in the second-line setting. However, prognosis remains poor for patients who are refractory to or relapse after BTK inhibitors, with ORRs for next-line treatments in the range 25–42% and median overall survival (OS) of only 6–10 months [4–6].
In 2020, based on the results of the ZUMA-2 trial, the first autologous chimeric antigen receptor (CAR) T-cell therapy – brexucabtagene autoleucel (brexu-cel) – was approved for r/r MCL following BTK inhibitor therapy [7]. In 2023, Poland introduced national reimbursement for brexu-cel for this indication.
Here, we present the first Polish single-center real-world experience with this innovative therapy in r/r MCL.
Methods
We retrospectively analyzed data from patients with r/r MCL treated with brexu-cel at our department between November 2023 and June 2025. All patients were enrolled according to the National Health Fund therapeutic program criteria. Following enrollment, leukapheresis was performed and autologous lymphocytes were sent for manufacturing, which lasted approximately 4 weeks. Treatment response was assessed using positron emission tomography–computed tomography (PET-CT) at 1 month and subsequently at 2, 3, 6, 9, and 12 months after infusion. OS was measured from brexu-cel infusion. Cytokine release syndrome (CRS) and immune effector cell-associated neurotoxicity syndrome (ICANS) were graded using American Society of Transplant and Cellular Therapy grading criteria [8]. Stata 19.5 BE (StataCorp, College Station, TX, USA) was used for the calculations; the Clopper–Pearson method was applied to determine the 95% confidence intervals (CI). Ethics approval was not required.
Results
A total of 18 patients (9 female, 9 male), median age 67 years (range: 52–75) received brexu-cel. All had prior BTK inhibitor exposure. The median number of previous treatment lines was 3 (range: 2–4). Six patients had undergone autologous and one allogeneic stem cell transplantation. The median time from MCL diagnosis to CAR T-cell therapy enrollment was 3 years (range: 1–10). Due to the long time since the initial diagnosis in some cases, it was not possible to retrieve initial complete clinical data or calculate individual risk scores for all patients. Comorbidities were common, including cardiac arrhythmias (3 patients) and prior breast cancer (1).
The median interval from leukapheresis to infusion was 45 days (32–67). All but 2 patients required bridging therapy during the manufacturing period due to progressive disease. As lymphodepletion, all patients received standard dose fludarabine and cyclophosphamide chemotherapy.
Within 3 months, 14 (77.8%) patients achieved complete remission (CR), and, as of August 2025, all remain in remission without the need for further therapy. No relapses have been observed to date. One patient died early, on post-infusion day 16, from treatment-related complications before response assessment. ORR among 17 evaluable patients was 82.4% (95% CI: 59.7–96.6%) and 77.8% (95% CI: 52.4–93.6%) for the entire cohort.
Three (16.7%) patients failed to achieve remission. Two of them died (3 and 7 months after infusion), and 1 remains in partial remission under ongoing treatment.
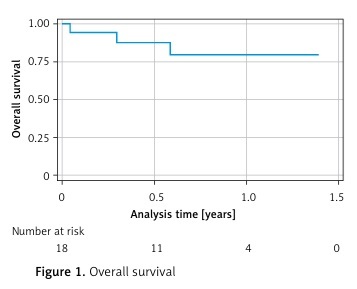
With a median follow-up of 12 months (range: 0–20), 15 (83.3%) patients are alive (Figure 1). Three deaths (16.7%) occurred: 2 due to disease progression, as mentioned above, and 1 (5.6%) from infection 16 days after infusion. Median OS and PFS were not reached (Table I).
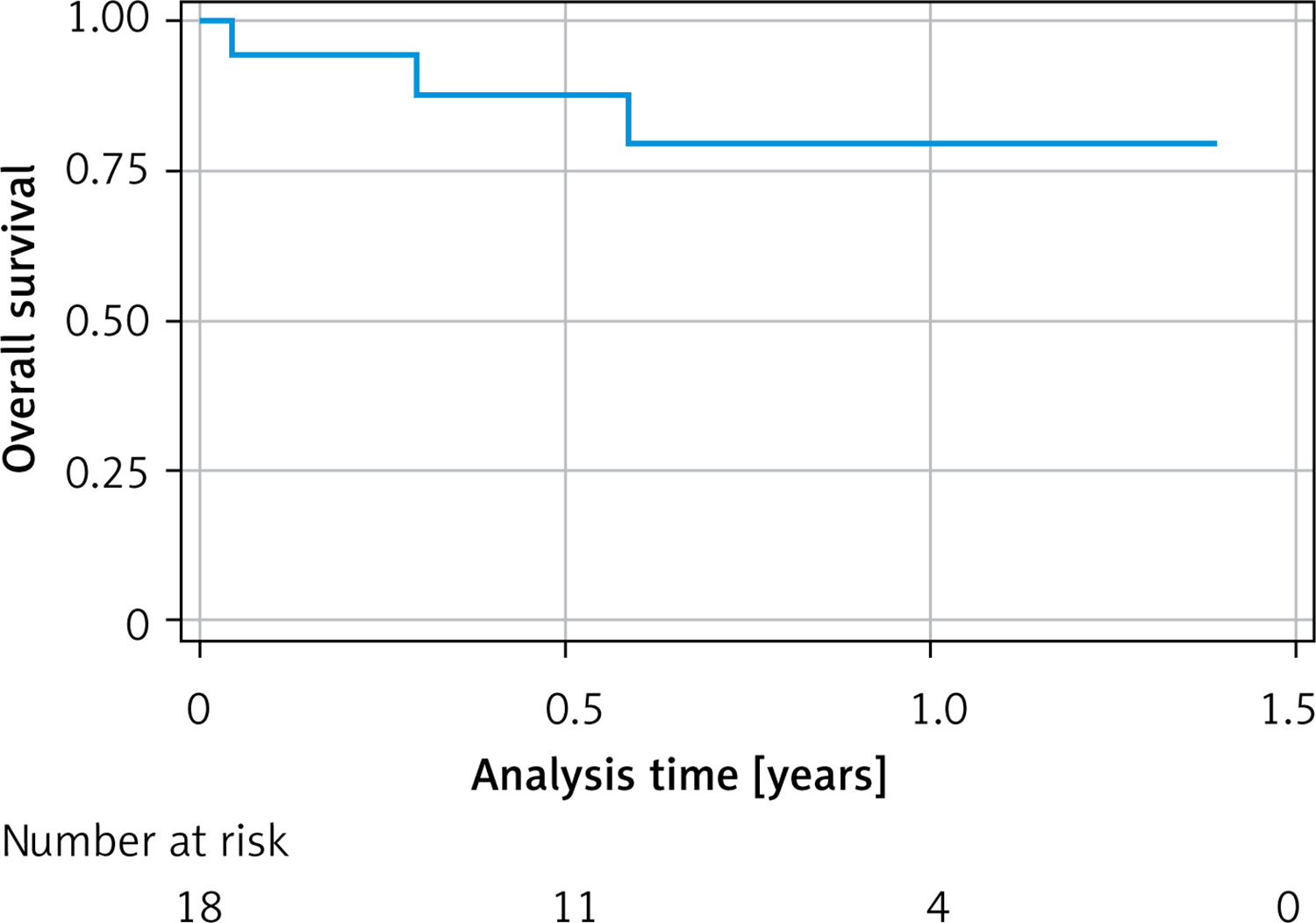
Table I
Key outcomes after brexu-cel therapy in MCL patients
CRS occurred in all patients, with Grade ≥ 3 toxicity in 4 (22.2%). All patients received tocilizumab and all but 1 also received corticosteroids.
ICANS occurred in 4 (22.3%) patients, including 2 of Grade 4 (11.1%). Two patients required admission to the intensive care unit (ICU), and 1 required mechanical ventilation. All patients with ICANS were treated with corticosteroids, and 2 also received anakinra.
Non-relapse mortality (NRM) was 5.6% (95% CI: 0.1–27.3%), i.e. 1 patient. This patient had a high disease burden at baseline, including pleural effusion and obstructive uropathy requiring placement of a DJ stent before lymphodepletion chemotherapy. Following infusion, she developed Grade 4 CRS and ICANS, required ICU admission and mechanical ventilation. Her course was further complicated by severe infection leading to septic shock and multiple-organ failure.
Other clinically relevant complications included: infections (4 patients), cardiac arrhythmias (5), and prolonged cytopenia (1).
All arrhythmia cases occurred concurrently with CRS symptoms. In 2 patients, supraventricular arrhythmias had been documented in their prior medical history, and 3 cases had no history of arrhythmias. One of these patients developed atrial fibrillation, followed by bradycardia; ultimately, sick sinus syndrome was diagnosed, and she required pacemaker implantation.
All but 1 patient developed CTCAE grade ≥ 3 neutropenia during the post-infusion period. According to the EHA/EBMT consensus grading of immune effector cell-associated hematotoxicity (ICAHT) [9], early neutropenia (days 0–30) was classified as grade 1 in 1 patient, grade 2 in eleven, grade 3 in 3 and grade 4 in 2 patients. Most patients experienced two or more episodes of late neutropenia (after day 30); however, grade 3 late neutropenia occurred in only 2 cases. All episodes of late neutropenia were intermittent and responded to G-CSF. CTCAE grade ≥ 3 thrombocytopenia was observed in only 5 patients. According to ICAHT grading, early thrombocytopenia was classified as grade 3 in 4 patients and grade 4 in 1 [10]. This patient also developed grade 4 late thrombocytopenia and, 5 months after CAR T-cell therapy, remains dependent on platelet transfusions and intermittently receives G-CSF.
Discussion
Brexu-cel was approved for MCL based on the phase-2 ZUMA-2 trial, which included a relatively small cohort of 68 patients [7]. As with other CAR T-cell products, approval was relatively quick and justified by the high response rates observed in patients with a poor prognosis and limited treatment options. This accelerated regulatory and reimbursement process has enabled patients to access potentially life-saving therapy.
However, the long-term outcomes and safety profile still require further investigation, especially because patients treated in routine clinical practice often differ significantly from those enrolled in clinical trials. In our experience, almost 40% of patients would not have met ZUMA-2 eligibility criteria due to comorbidities, history of allogeneic stem cell transplantation, or presence of an indwelling catheter.
There are only a few real-world analyses of the efficacy and safety of brexu-cel in MCL [11–13], most of them with relatively short follow-up. The treatment response rate is high and comparable to that achieved in the ZUMA-2 trial; however, the rates of complications, particularly infectious complications, appear to be higher in real-world experience.
Our observation confirms the excellent results observed in the clinical trial, with ORR 77.8%, 1-year OS 80.8% and median OS and PFS not reached after a median follow-up of 12 months. No patient relapsed during the observation period. In comparison with the ZUMA-2 trial, in 3-year analysis the ORR was 91% (95% CI: 81.8–96.7%), with 68% achieving CR (95% CI: 55.2–78.5%), and 37% remaining in remission [14]. The median duration of response was 28.2 months and the median PFS was 25.8 months, suggesting that our observation is probably too short to evaluate the long-term efficacy. However, based on these data, this therapy appears to be the best option nowadays for patients with r/r MCL. It is worth emphasizing that almost all (94.4%) of our patients required bridging compared with 37% in the ZUMA-2 trial, which indicates that a greater proportion had a more aggressive course of disease [7].
Brexu-cel is generally a safe treatment option for patients with r/r MCL. Although most patients experienced complications, they were usually mild and without serious consequences. Compared with the ZUMA-2 trial, our patients had similar rates of CRS, but a lower rate of ICANS. Significantly more patients received steroids for treatment of CRS in our group (94.4% vs 22% in the ZUMA-2 trial), and this may be the reason for the lower incidence of ICANS.
Of note is the relatively high incidence of cardiac arrhythmias (27.8%). Arrhythmias, most commonly atrial fibrillation, appear to be among the more frequent complications following this type of therapy, with reported rates ranging from 5% to 18% [15–17]. A prior history of arrhythmia seems to be the strongest risk factor for this complication [17]. Cardiotoxicity associated with CAR T-cell therapy can manifest in several forms, including acute coronary syndrome, heart failure, arrhythmias, and pericarditis/myocarditis. The mechanism underlying post-CAR T-cell cardiotoxicity appears to be complex. In most patients, they occur during the cytokine release phase, suggesting a direct effect of inflammatory cytokines; however, a direct cross-reactivity with an antigen expressed on myocardial cells may also play a role [15, 17]. Although cardiac arrhythmias are often clinically significant and require intervention, they do not appear to adversely affect treatment effectiveness or OS [17]. However, the long-term effects remain largely unknown [15].
Among the significant complications, the case of prolonged cytopenia deserves attention. In registration trials and real-world studies, prolonged cytopenia has been reported with varying frequency. In our cohort, although observed in only 1 patient, it represents a serious clinical problem, as the patient is 75 years old and not eligible for allogeneic stem cell transplantation. The patient remains in remission from lymphoma but continues to be dependent on platelet transfusions.
In conclusion, our analysis confirms that brexu-cel is effective in patients with r/r MCL and is associated with a low rate of serious complications. We seem to have learned how to manage the typical complications associated with this therapy; however, we must remain vigilant for rarer adverse events and continue to monitor them closely.
This study has some limitations, including the relatively small cohort size, which reflects the rarity of the disease, as well as the relatively short follow-up period. Nevertheless, we plan to conduct an updated analysis in the future as more patients are treated and longer-term data become available.