Introduction
Stress is a common issue among the general population and is inversely related to health outcomes. This necessitates new and more efficient strategies of stress management in daily life [1, 2].
Traditional approaches to stress management include exposure to nature, progressive muscle relaxation, breathing exercises, meditation, and mindfulness-based and traditional cognitive behavioural therapy. Despite a large body of evidence that supports the utility and efficacy of relaxation techniques [3–5], they have significant limitations. Most of them are hard to learn and implicate in daily life, and they require repetitive practice and a lot of training time or even co-work with a psychotherapeutic professional [6]. Traditional relaxation practices are based on advanced concentration and imagination skills [7].
Emerging technologies like virtual reality (VR) have been extensively studied for recreational and medical purposes for two decades [8]. In particular, VR demonstrates a promising opportunity to facilitate the relaxation process and to make it easily applicable for non-trained subjects [9]. A three-dimensional, computer-generated environment viewed through a head-mounted display provides a more vivid experience than that most people can have using their own imagination or different media resources [10]. Users can practice relaxation techniques at their own pace and as many times as required at home, at work, while travelling, etc. Developers have progressed in making VR devices more reliable, cost effective, and acceptable for everyday use. Positive visual and audial stimuli associated with recreation have been successfully reproduced in VR for relaxation purposes [11, 12], and controlled studies show that VR technology increases the efficiency of traditional relaxation techniques [13, 14].
At the same time, neurofunctional studies provide better understanding of the mechanisms underlying the benefits of different approaches to relaxation in people affected by stress. The autonomic nervous system (ANS), composed of two primary branches: the sympathetic nervous system (SNS) and the parasympathetic nervous system (PNS), plays a crucial role in stress response as well as in post-stress relaxation and recovery [15]. Some modalities of meditation [16, 17], sedative music (at or below a resting heart rate of 60 beats per minute) [18], as well as exposure to nature [19], have been shown to be helpful in stress release via decrease of cortisol and catecholamine levels and downregulation of the SNS.
Heart rate variability (HRV) is one of the most used and well described approaches towards studying both sympathetic (SNS) and PNS influences [20]. Due to adoptive reactions, there are always some changes occurring in time intervals between consecutive heartbeats, which can be studied using electrocardiography (ECG). The high-frequency (HF) and low-frequency (LF) components of HRV allow tracking of SNS and PNS activity under controlled conditions. The power of high frequency is generally associated with PNS activity, while LF, proportional to HF, measures the state of autonomic balance in the heart [21, 22]. Both are yielded using a 5-minute ECG [23]. HRV, as an important marker of the ANS balance, is also useful for analysis of some neurogenic disorders [24].
Among different factors influencing ANS, binaural beats are a very important phenomenon. Binaural beats are an auditory illusion perceived when two pure tones with a slight difference in their frequency are presented to each ear separately. Numerous studies report on binaural-beat exposure reducing anxiety levels and entailing other psychophysiological changes, as shown by meta-analysis [25]. Also, binaural-beat listening resulted in greater self-reported relaxation relative to the placebo condition [26].
Thus, activation of PNS and sympathetic withdrawal appear to be key factors providing relaxation and restoration processes, and according to current evidence, they can be achieved in different ways. This study hypothesises that, unlike conventional VR only, a positive virtual environment introducing a combination of additional stimuli to ANS (e.g. meditation modalities, binaural effect, audio-visual sequence synchronised with the tract of respiratory movements and the frequency of heart rate) provides a faster and greater shift in the autonomic balance toward vagal activation and relaxation after stressors. This study aims to assess the effect of modified VR intervention on short-term heart rate variability (HRV) and perceived anxiety level in healthy volunteers affected by moderate stress. Pure Purr Tech is a highly developed innovative company specialising in hardware and software solutions for relaxation and stress management. Both types of software (investigated and sham) were developed by Pure Purr Tech, and the software of the investigational device was selected from around 30 different versions based on the significance of the influence on ANS. Levels of anxiety were measured before and after VR sessions using the State-Trait Anxiety Inventory (STAI) to find possible correlations with physiological parameters.
Material and methods
Study design
This randomised, sham-controlled, crossover, investigator-blinded clinical trial (NCT03532152 on ClinicalTrials.gov) was conducted in a single clinical centre (Kyiv, Ukraine) from August to September 2018 in accordance with the Declaration of Helsinki and Good Clinical Practice.
Participants
This study involved healthy adults, of both sexes, aged 20 to 60 years, without history of cardiovascular diseases or essential abnormalities on ECG, and with normal or moderate levels of situational anxiety on the STAI scale. All participants in the study signed an informed consent form. The sample size was calculated based on the following parameters: size of the clinically important differences – 0.1; limiting probability of type I error – 0.05; study power – 95%. Thus, the estimated sample size was 36.
Exclusion criteria were: intolerance to the VR technology; heart rate (HR) > 110 bpm or < 50 bpm; respiratory rate > 23 per minute; abuse of psychotropic substances; smoking more than 100 cigarettes per week; administration of drugs for the treatment of cardiovascular and neurological diseases 3 days prior to participation in the study; drinking tonics and energy drinks for at least 2 h prior to participation in the study; severe or acute forms of respiratory, urogenital, gastrointestinal, haematological, metabolic, endocrine, or neurological diseases; mental disorders that, in the opinion of the investigator, might have distorted the results of the study; pregnancy; and any disease of the thyroid gland. Participants were recruited through an Internet advertisement and among outpatients of a single medical centre at the time of their visits to the clinic for different medical reasons.
Intervention
Pure Purr technology
The Pure Purr technology, a medical hardware with pre-installed software for parasympathetic neurostimulation, consists of a commercially available BoboVR X1 headset with sufficient resolution display (IPS 5.5 TFT, 1920 x 1080 pixels, frame refresh rate 60 Hz), built-in processor and memory, and extended-range stereo speakers. In the active arm (investigational device or headset A), the VR audio-visual sequence is modified by adding a binaural effect and is synchronised with the tract of respiratory movements and the frequency of heart rate.
The virtual environment consists of a beach scene with some objects to view, such as sea waves, and a cat walking around (Figure 1 A). The cat is used as the main object to maintain attention during the session. The walking pace of the cat is synchronised with a resting heart rate of 60 beats per min.

The audio sequence consists of a slow musical composition modified by adding a binaural effect. The background sound of a cat purring was slowed down and also modified in the same way. Purring is a unique form of vocalisation in the feline family and is usually associated with an animal’s contentment and the state of rest. In the active VR audio-visual sequence, the modified cat purring acts as additional stimulus that activates PNS.
Sham technology
The sham technology (headset B or sham arm) consisted of an identical VR headset with a similar audio-visual sequence (Figure 1 B). The key difference was that the audio-visual sequence was neither modified with the binaural effect nor synchronised with the tract of respiratory movements and HR. The software for the shame technology was also a product of Pure Purr Tech.
The psychological stressors in this study were mental arithmetic (MA) tasks, which produced significant increases in heart rate (HR) and HRV [27]. The MA task featured consecutive adding of three-digit numbers. The set of numbers was identical for all participants.
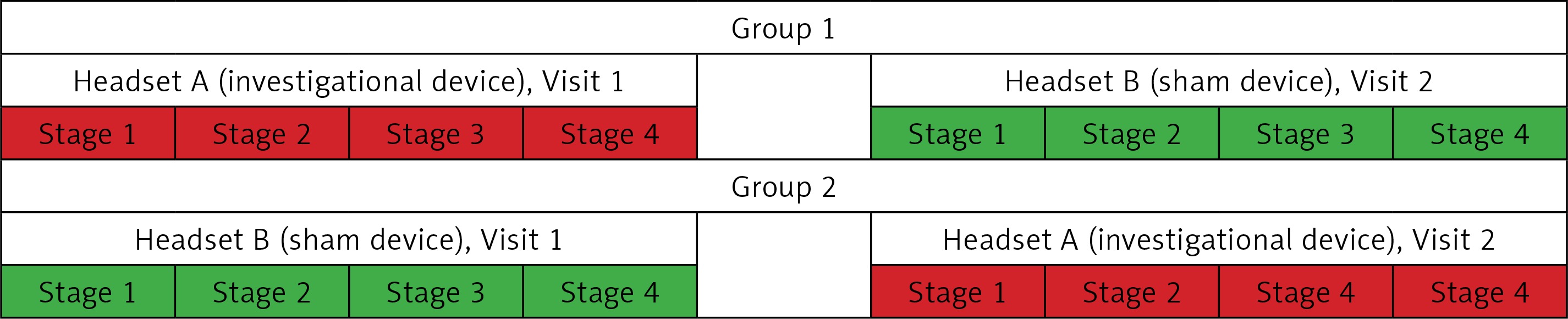
Healthy volunteers were sorted in two equal randomised groups to receive 5-minute VR sessions with active or sham investigational sequences in two visits (Figure 2). All sessions in each group followed a stress-producing MA task. The length of time between the two visit dates was at least 1 day but no more than 7 days. Groups were randomly assigned to receive different devices during visits.
Figure 2
Study protocol. Visit 1 goals: select and randomise participants; obtain informed consent; STAI assessment; 5-min ECG at rest (stage 1); 5 min of moderate stress by mental arithmetic with second ECG (stage 2); 5-min VR session 1 (active or sham) with third ECG (stage 3); 5-min ECG after VR intervention, STAI assessment (stage 4). At least 1 day and night after visit 1 (a night’s sleep was mandatory). Visit 2 goals: check exclusion criteria; 5-min ECG at rest (stage 1); 5 min of moderate stress by mental arithmetic with second ECG (stage 2); 5-min VR session 2 (active or sham, different to the one received during Visit 1) with third ECG (stage 3); 5-min ECG after VR intervention, STAI assessment (stage 4)
Measurements
The 5-min ECG recordings of HRV were performed four times on each visit: before the MA task, during MA, during the VR session, and after the VR session. The HRV was chosen as a sensitive method for evaluating changes in SNS and PNS activity within the time scale of one clinical visit [28]. Electrocardiogram readings were taken using a calibrated 12-channel CONTEC 8000G ECG Workstation (CONTECTM, China).
Participants were also asked to fill out the State-Trait Anxiety Inventory (STAI) form before and after the 5-min VR exposure. The STAI was developed by the psychologist Charles Spielberger. This is a psychological inventory consisting of 40 questions on a self-report basis. Analysis of the results is based on a Likert scale. Higher scores are positively correlated with higher levels of anxiety. State anxiety, i.e. anxiety about an event, can be distinguished from trait anxiety, i.e. anxiety level as a personal characteristic [29].
The primary outcome measure was a high frequency (HF) power after a 5-min exposure to the VR audio-visual sequence. Secondary outcomes in HRV analysis included the square root of the mean squared differences of successive R-R intervals (RMSSD), LF/HF power ratio, standard deviations in NN intervals (SDNN), total power, HR, systolic and diastolic blood pressure, and STAI scores after a 5-min exposure to the investigational VR. A safety outcome included vital signs and the incidence of adverse events.
Statistical analysis
Statistical analysis was performed using Med-Calc v. 18.11.3 (MedCalc Software Inc., Broekstraat, Belgium). Quantitative variables were: (1) the arithmetic mean (M) and standard deviation (± SD) for normally distributed data; (2) median (Me) and interquartile range (QI ÷ QIII) for non-normally distributed data. Normality in statistics was checked via Shapiro-Wilk test. Categorical variables were summarised using frequencies and proportions (%). The 95% confidence intervals (95% CI) were found for all parameters.
For independent groups, comparative analysis of quantitative variables was performed using t-test (for normally distributed data) or Mann-Whitney test (for non-normally distributed data). Paired samples were analysed using the paired t-test (for normally distributed data) or T Wilcoxon test (for non-normally distributed data). Additionally, the Hodges-Lehmann median difference was calculated alongside its 95% CI. After-data (data after VR) were compared with before-data (in %) and the baseline. Fisher’s exact test was used to compare qualitative variables (for independent groups), and the McNemar test was used to test the differences between paired proportions.
Mixed three-way ANOVA was applied to analyse VR performance through changes in HF-HRV (ΔHF-HRV [Stress after VR]). Fixed factors were the “exposure sequence” or sequence in which volunteers used the headsets (levels: “headset A – headset B” and “headset B – headset A”) and the “headset” (levels: “headset A” and “headset B”), while the “subject” factor was a random effects factor. The sequence of immersion events (levels: “Visit 1” and “Visit 2”) was considered an interaction effect between fixed factors. The residues were not normally distributed (p < 0.001); therefore, the rank transformation [30] was involved. On analysis of measurement the same variables for different time points Friedman test and post-hoc (according to Conover, [31]) was used.
The significance level was 0.01 for Shapiro-Wilk test and 0.05 for other tests.
Results
Group homogeneity analysis
The group homogeneity analysis of demographic and anthropometric variables revealed no statistically significant differences (p > 0.05) between randomisation groups (Table I). There were also no statistically significant differences (p > 0.05) in physiological variables (Table II).
Table I
Demographic and anthropometric data for randomisation groups
| Variable | Group A–B (n = 56) | Group B–A (n = 38) | Total (n = 94) | P-value |
|---|---|---|---|---|
| Age [years] | 40.3 ± 9.2 [23.9 to 59.0] | 37.4 ± 9.6 [19.5 to 59.7] | 39.1 ± 9.4 [19.5 to 59.7] | 0.155a |
| Weight [kg] | 79.6 ± 16.0 [48 to 113] | 79.1 ± 17.7 [46 to 118] | 79.4 ± 16.6 [46 to 118] | 0.899a |
| Height [cm] | 173.1 ± 8.3 [157 to 193] | 173.9 ± 8.3 [159 to 192] | 173.4 ± 8.2 [157 to 193] | 0.655a |
| Gender, n (%): | ||||
| Male | 31 (55.4) | 25 (65.8) | 56 (59.6) | 0.393b |
| Female | 25 (44.6) | 13 (34.2) | 38 (40.4) | |
Table II
Physiological data for randomisation groups at Visit 1
| Variable | Group A–B (n = 56) | Group B–A (n = 38) | Total (n = 94) | P-value |
|---|---|---|---|---|
| SBP [mm Hg] | 120 (120; 130) [90 to 140] | 120 (120; 120) [90 to 140] | 120 (120; 130) [90 to 140] | 0.458b |
| DBP [mm Hg] | 80 (80; 80) [50 to 100] | 80 (75; 80) [60 to 95] | 80 (80; 80) [50 to 100] | 0.746b |
| Respiratory rate [1/min] | 18 (17; 18) [15 to 20] | 18 (17; 18) [15 to 19] | 18 (17; 18) [15 to 20] | 0.581b |
| Pulse [1/min] | 71.8 ± 7.9 [50 to 100] | 70.4 ± 10.3 [60 to 95] | 71.2 ± 8.9 [50 to 100] | 0.462a |
| Temperature [°C] | 36.6 (36.6; 36.6) [36.1 to 36.7] | 36.6 (36.6; 36.6) [36.4 to 36.8] | 36.6 (36.6; 36.6) [36.1 to 36.8] | 0.614b |
Physical examinations revealed no clinical deviations in both groups at first and second visits. One person had chronic tonsillitis (incidence rate 1.1%), but other participants did not have any disease in their history. Volunteers did not receive concomitant therapy at the time of investigation.
Change in high-frequency-heart rate variability after a 5-minute exposure to the virtual reality audio-visual sequence
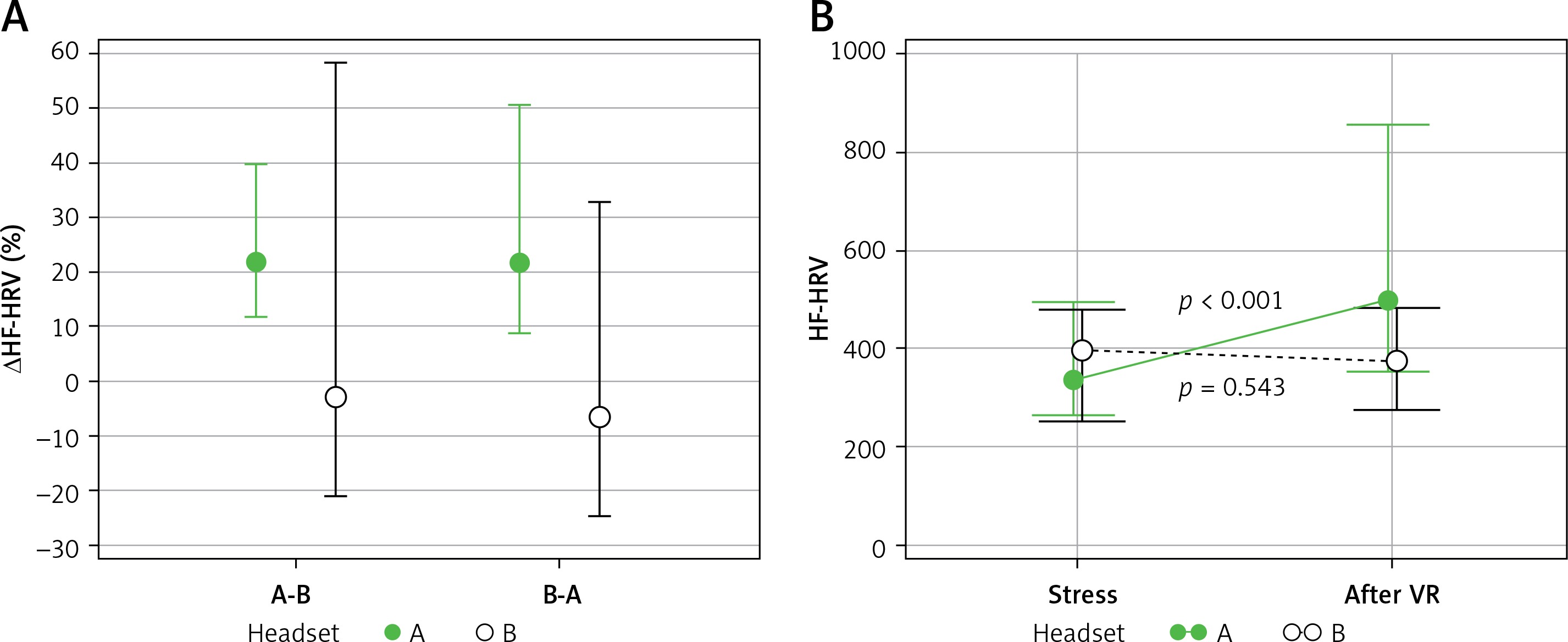
Change in HF-HRV after a 5-minute exposure to the VR audio-visual sequence was a primary outcome measure in this study. The findings show a significant increase in parasympathetic activity after a 5-minute exposure to the investigational device compared to stress, as shown by HF-HRV (499.8 ms2 and 340.5 ms2, p < 0.001). There were no changes in HF-HRV after a 5-minute exposure to headset B (sham device). The relative change of HF (ΔHF, calculated as the difference between HF after stress and after VR, divided by HF after stress) was 21.8% [13.0% to 38.7%] for headset A. The difference between two headsets was 30.6% [11.4% to 48.3%], which is statistically significant (p < 0.05). Note that the exposure sequence and the sequence of immersion events do not influence ΔHF-HRV (p = 0.558, p = 0.523, respectively), as shown by mixed three-way ANOVA (Figure 3). Therefore, headset A (investigational device) was more effective in decreasing HF (p < 0.05) than headset B (sham device).
Figure 3
Between-subject interaction effects from the ANOVA output. A – Exposure sequence and the sequence of immersion events did not influence ∆HF-HRV; B – significant increase in parasympathetic activity after a 5-minute exposure to investigational device (headset A) but not sham device (headset B) compared to stress, as shown by HF-HRV
Changes in situational anxiety levels after a 5-minute virtual reality exposure for each headset
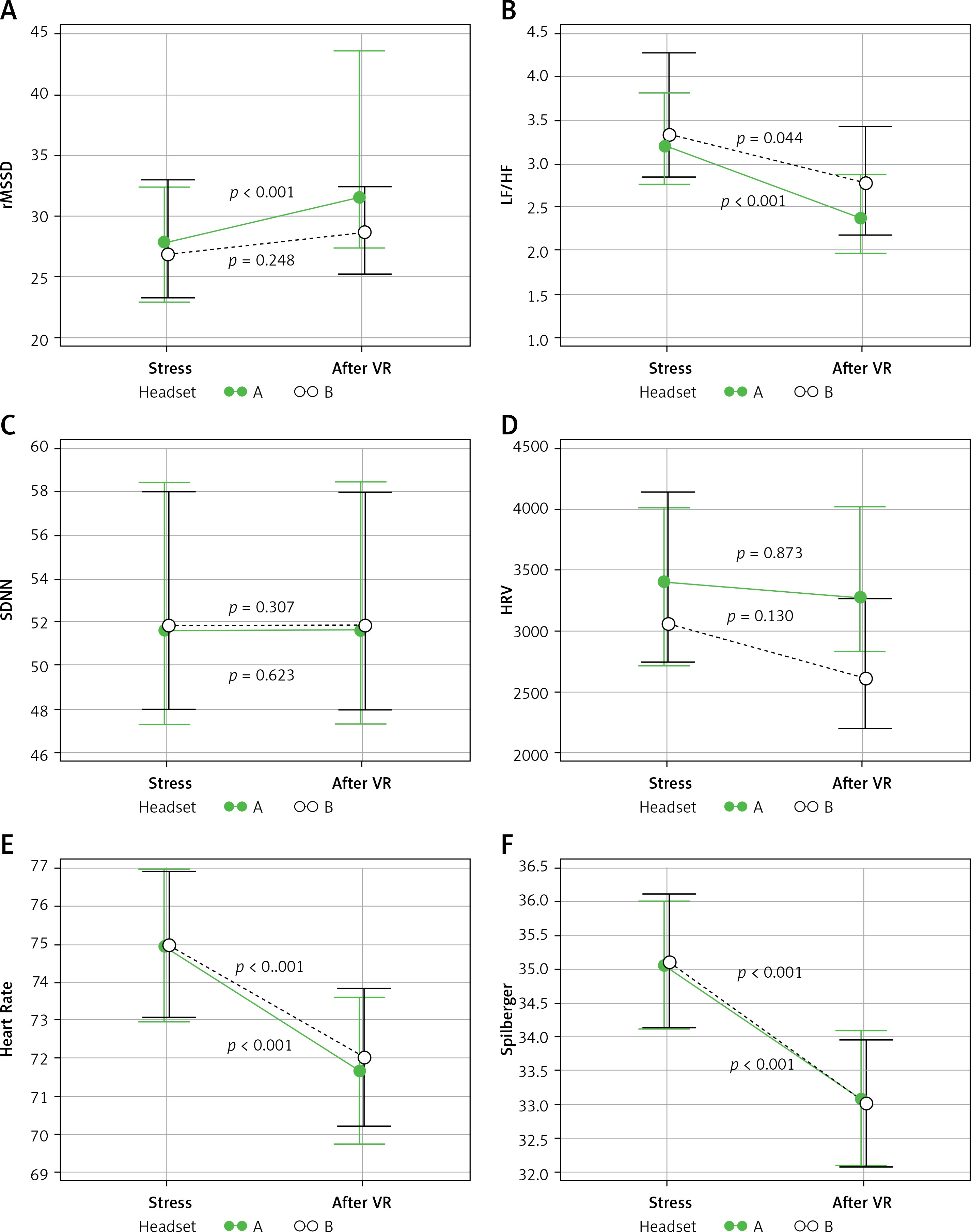
Secondary outcomes demonstrate that the investigational device (headset A) was also better than the sham device (headset B) in increasing rMSDD (difference of 12.3% [2.6% to 23.1%], p = 0.02) and in decreasing the LF/HF ratio (difference of –14.5% [–27.7% to –1.0], p = 0.04). Both these changes represent shifts of ANS activity toward the parasympathetic branch (Figure 4). At the same time, there were no differences between investigational and sham device in their ability to induce changes in SDNN (p = 0.307) and HRV (p = 0.873). The average meaning of STAI score among participants of the trial was 35.1 at the start of each visit, and was decreased after a 5-minute exposure to VR to 33.2 in the case of the sham device and to 33.1 in the case of the investigational device (p < 0.001). The STAI score decreased after a 5-minute VR exposure to either of the headsets (p < 0.001) (Figure 4). Changes that occurred in the levels of situational anxiety after a 5-minute VR exposure demonstrate that the exposure sequence and the sequence of immersion events did not influence the rMSSD (p = 0.487), LF/HF (p = 0.299), SDNN (p = 0.36), HRV (p = 0.357), or HR (p = 0.849). However, the visit date is crucial to the ΔSTAI score (p = 0.048).
Figure 4
Changes in situational anxiety levels after a 5-minute VR exposure for the investigational device (headset A) and the sham device (headset B): A – changes of root mean square of successive differences between normal heartbeats (RMSSD), ms, B – changes of low-frequency to high-frequency (LF/HF) HRV components, C – changes of the standard deviation of the IBI of normal sinus beats (SDNN), ms, D – total power of HRV, ms2, E – changes of the heart rate, F – changes of the STAI scores
Safety results
In both groups, investigational and sham, there were no negative side effects detected after VR. The risk of a negative reaction was 1% [0% to 2.0%]. There was no difference in tolerability (p = 0.714) between the groups. Tolerability evaluations for the investigational device ranged between “good” and “very good”.
Discussion
So far, VR technologies are a subject of recreational and medical studies [8]. Virtual reality demonstrates a promising opportunity to facilitate the relaxation process and is easily applicable for non-trained subjects [9]. Valtchanov et al. showed that immersion in a virtual nature setting has similar beneficial effects as exposure to surrogate nature (a slideshow of abstract paintings), as shown by HR and skin conductance levels [11]. Villani et al. compared three interactive experiences: VR, video, and audio, with a narrative to progressive muscle relaxation and breathing exercises. Results showed the efficacy of all three interactive experiences in inducing positive emotions and integrating different approaches to managing stress. In particular, VR showed better improvements related to the psycho-physiological changes [12]. Plante et al. showed that VR enhances the positive psychological and stress-management benefits of aerobic exercise [13, 14].
McConnell et al. established a restorative effect of “wide-band” theta-frequency binaural beats, mediated by a combination of sympathetic withdrawal and parasympathetic activation, as inferred through high-frequency (HF) and low-frequency (LF) components of HRV [26].
This study explores the potential for Pure Purr VR technology to be used in a medical setting, for parasympathetic neurostimulation, stress resolution, and relaxation. This software and hardware solution consists of a commercially available BoboVR X1 headset with Pure Purr modification (i.e. binaural effect and synchronisation with the tract of respiratory movements and the frequency of heart rate). Because ANS balance plays a prominent role in recovering after stress, short-term HRV via ECG was chosen as a measure for SNS or PNS activity under controlled conditions.
Findings indicate that Pure Purr VR is a very effective way to stimulate PNS. In particular, HF-HRV is increased significantly after a 5-minute exposure to VR audio-visual content, in comparison to stress. A significant decrease in the LF/HF ratio supports the claims of Pure Purr regarding stress release and relaxation, by providing evidence on the ability of this technology to increase PNS activity and to support stress resolution. The self-reported measure of situational anxiety alongside short-term HRV values indicates a decrease in the level of anxiety and in SNS activity after a 5-minute exposure to Pure Purr VR. Finally, this study demonstrates that the Pure Purr VR technology is a safe option for relaxation and can be assigned to healthy volunteers affected by moderate stress.
One of the interesting observations of this study is the decrease of heart rate in both groups of volunteers, which was not dependent on the type of device applied. The reduction of heart rates in both groups of volunteers (Figure 4 E) can be explained by the recumbent position of the patient during each ECG and VR session. Thus, a decrease in heart rate is due to the rest position and does not depend on the type of applied device.
The increase of HF-HRV observed only after application of the investigational Pure Purr medical device (Figures 3 B and 4 D) supports the main hypothesis of this research that Pure Purr intervention strongly modulates ANS balance toward parasympathetic activation. It is also important that during Visit 2 people received intervention that was different to that received during the first visit. The effect on heart rate reduction was the same, but the increase of HF-HRV was dependent only on the device used.
Possible limitations of Pure Purr medical device usage include psychiatric disorders, intolerability to VR technology, and acute forms of cardiovascular, neurological, and cerebrovascular diseases.
Thus, it can be argued that the Pure Purr medical device for parasympathetic neurostimulation has a restorative effect on the autonomic nervous system in healthy volunteers affected by moderate stress. This article offers clinically relevant evidence on the significant relaxing effect of Pure Purr on volunteers.
Safety and tolerability data show that the Pure Purr technology is an absolutely safe option and can be recommended for medical and recreational applications.