Current issue
Archive
Manuscripts accepted
About the Journal
Editorial office
Editorial board
Section Editors
Abstracting and indexing
Subscription
Contact
Ethical standards and procedures
Most read articles
Instructions for authors
Article Processing Charge (APC)
Regulations of paying article processing charge (APC)
ONCOLOGY / RESEARCH PAPER
Serum TNF-α dynamics under chemoradiation and prognosis in high-grade glial tumors
1
Adana City Training and Research Hospital, Department of Radiation Oncology,, Turkey
2
. Department
of Biostatistics, Van Yüzüncü Yıl University Medical Faculty, Turkey
3
Department of Biotechnology, Faculty of Science, Mersin University, 33343,, Turkey
4
Adana City Training and Research Hospital, Department
of Neurosurgery, Turkey
5
Adana City Training and Research Hospital, Departmen of Medical Oncology., Turkey
6
Department of Microbiology. Çukurova University School of Medicine, Department of Microbiology, Turkey
Submission date: 2025-11-05
Final revision date: 2026-01-29
Acceptance date: 2026-02-25
Online publication date: 2026-06-04
Corresponding author
KEYWORDS
TOPICS
ABSTRACT
Introduction:
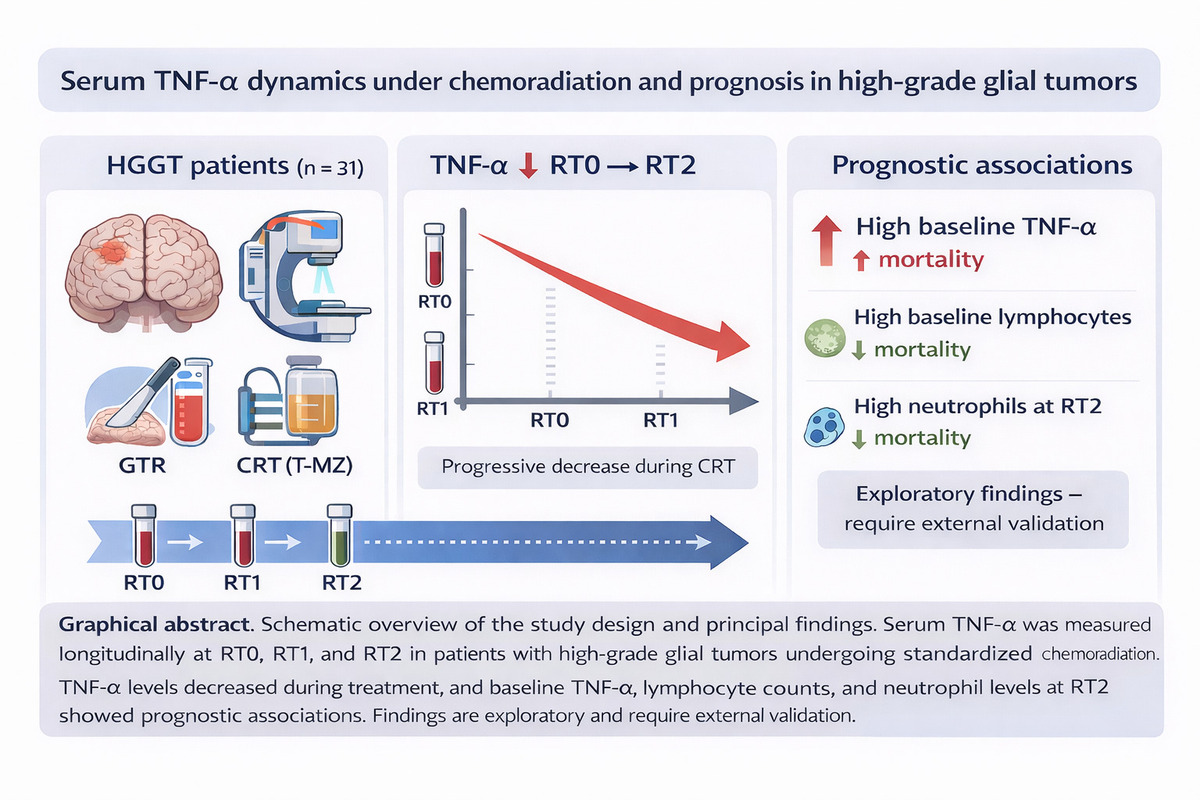
Tumor necrosis factor-alpha (TNF-α) is a mediator of cancer-related inflammation and may affect glioma biology. Clinical information on longitudinal TNF-α dynamics during chemoradiation (CRT) and their prognostic relevance in high-grade glial tumors (HGGT) is limited. This study examines serum TNF-α levels in patients with HGGT undergoing CRT.
Material and methods:
In this prospective, single-center cohort, 31 adults with HGGT who underwent gross-total resection received standardized IMRT/VMAT with concomitant/adjuvant temozolomide. Serum TNF-α levels were assessed at three predetermined intervals: prior to radiotherapy (RT0), upon completion (RT1), and three months following radiotherapy (RT2). The principal outcome was the variation in TNF-α from RT0 to RT2.
Results:
The systemic inflammatory response decreased progressively, with TNF-α levels declining by 33% from RT0 to RT2. Multivariable analysis showed that elevated baseline TNF-α levels were associated with poorer overall survival (hazard ratio [HR] 1.50; 95% CI 1.04–2.16). Patients with elevated baseline lymphocyte counts (HR 0.10; 95% CI 0.03–0.32) and higher neutrophil counts at RT2 (HR 0.35; 95% CI 0.18–0.69) experienced lower mortality rates, within the constraints of sample size and event number.
Conclusions:
TNF-α decreases during CRT, and elevated baseline TNF-α levels are associated with increased mortality risk in HGGT. Higher baseline lymphocyte counts and higher neutrophil counts at RT2 are associated with better outcomes, although these findings are hypothesis-generating and require external validation. Any ROC-derived TNF-α cut-off is exploratory and should not be used for clinical decisions without independent validation.
Tumor necrosis factor-alpha (TNF-α) is a mediator of cancer-related inflammation and may affect glioma biology. Clinical information on longitudinal TNF-α dynamics during chemoradiation (CRT) and their prognostic relevance in high-grade glial tumors (HGGT) is limited. This study examines serum TNF-α levels in patients with HGGT undergoing CRT.
Material and methods:
In this prospective, single-center cohort, 31 adults with HGGT who underwent gross-total resection received standardized IMRT/VMAT with concomitant/adjuvant temozolomide. Serum TNF-α levels were assessed at three predetermined intervals: prior to radiotherapy (RT0), upon completion (RT1), and three months following radiotherapy (RT2). The principal outcome was the variation in TNF-α from RT0 to RT2.
Results:
The systemic inflammatory response decreased progressively, with TNF-α levels declining by 33% from RT0 to RT2. Multivariable analysis showed that elevated baseline TNF-α levels were associated with poorer overall survival (hazard ratio [HR] 1.50; 95% CI 1.04–2.16). Patients with elevated baseline lymphocyte counts (HR 0.10; 95% CI 0.03–0.32) and higher neutrophil counts at RT2 (HR 0.35; 95% CI 0.18–0.69) experienced lower mortality rates, within the constraints of sample size and event number.
Conclusions:
TNF-α decreases during CRT, and elevated baseline TNF-α levels are associated with increased mortality risk in HGGT. Higher baseline lymphocyte counts and higher neutrophil counts at RT2 are associated with better outcomes, although these findings are hypothesis-generating and require external validation. Any ROC-derived TNF-α cut-off is exploratory and should not be used for clinical decisions without independent validation.
| eISSN: | 1896-9151 |
| ISSN: | 1734-1922 |
We process personal data collected when visiting the website. The function of obtaining information about users and their behavior is carried out by voluntarily entered information in forms and saving cookies in end devices. Data, including cookies, are used to provide services, improve the user experience and to analyze the traffic in accordance with the Privacy policy. Data are also collected and processed by Google Analytics tool (more).
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.
You can change cookies settings in your browser. Restricted use of cookies in the browser configuration may affect some functionalities of the website.