Introduction
Intrahepatic cholangiocarcinoma (ICC), the second most common primary malignant tumor of the liver, originates from the intrahepatic bile duct’s epithelium [1]. Over the last four decades, both the incidence and mortality rates of ICC have witnessed a steady rise [2]. Currently, curative surgical resection is largely perceived as the sole method for curing ICC [3]. Yet, owing to the concealed clinical symptoms of ICC coupled with the absence of effective early screening techniques, only a limited 20–30% of ICC patients are eligible for curative surgical resection [4]. For patients with unresectable ICC, palliative treatment options available in clinical practice include chemotherapy (CT), radiotherapy (RT), and chemoradiotherapy [5–8]. Nevertheless, the relatively small number of ICC patients and the consequent lack of extensive research data pose a significant challenge. Many studies conducted to date have been small scale, retrospective, and with non-randomized design, and some have even included mixed studies featuring gallbladder and other bile duct tumors, thereby complicating the evaluation of the therapeutic value of palliative treatment for ICC [9].
The SEER database, covering cancer incidence, treatment methods, survival rates, etc., for about 30% of the U.S. population, can serve as a valuable resource for research on rare diseases like ICC that lack randomized controlled data [10, 11]. Recognizing the dearth of extensive comparative studies on palliative treatment methods for ICC, this study leveraged the SEER database to evaluate the survival benefits of different clinical management methods (such as chemotherapy, radiotherapy, chemoradiotherapy, and scenarios with no chemotherapy or radiotherapy) for patients with unresectable ICC.
Material and methods
Ethics statement
This study leveraged the publicly available SEER database, for which we obtained permission from the National Cancer Institute for research purposes. As the study did not involve human interaction or the use of personal identifying information, informed consent was not required. Given that the patient data from the database had already been de-identified and made available for research, the Ethics Committee of Jiangyin People’s Hospital granted an exemption for ethical approval for this study.
Search strategy and patient cohort
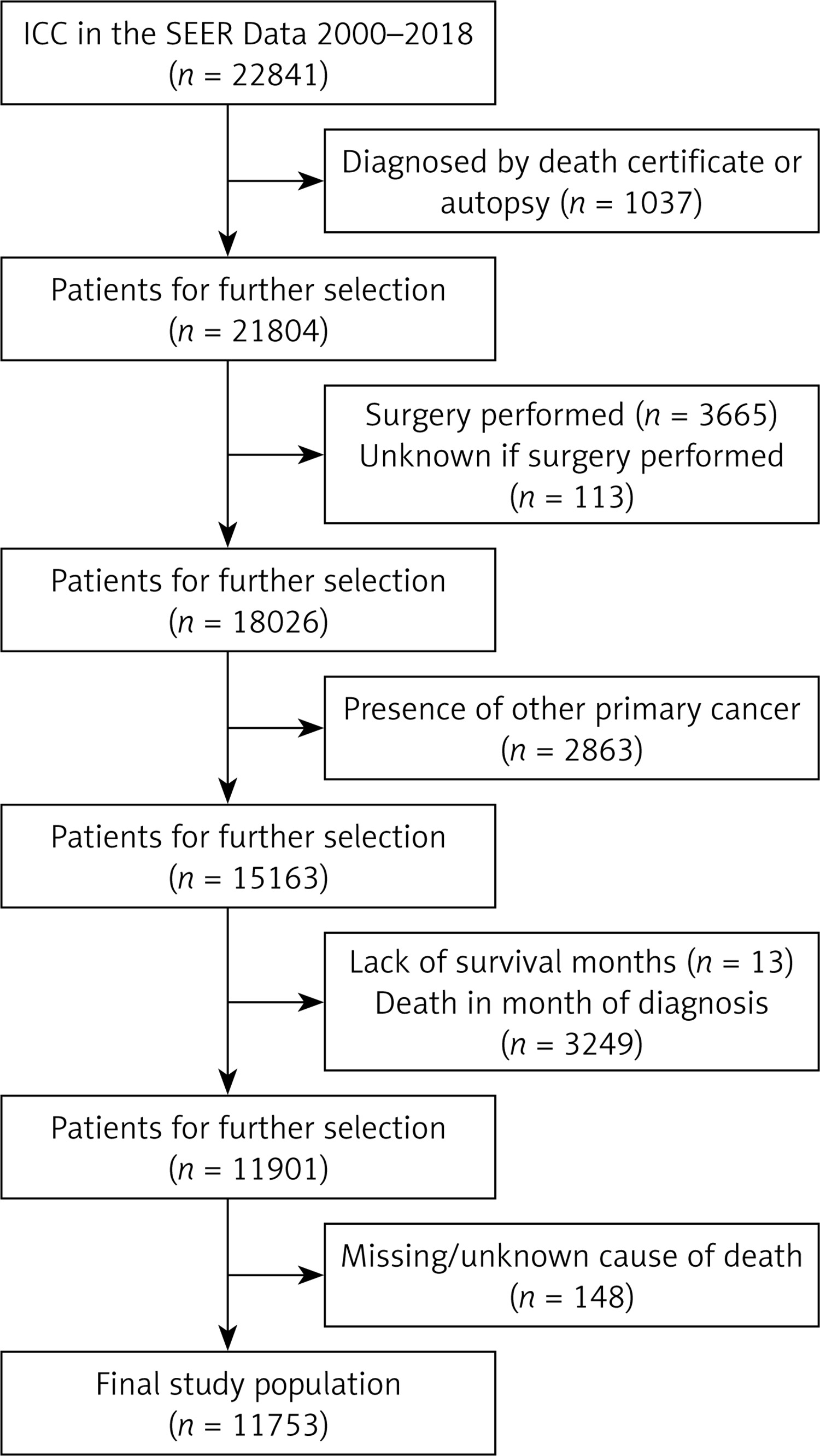
The Surveillance, Epidemiology and End Results (SEER) program’s official software, SEER*Stat (version 8.3.5), was used to select patient information related to confirmed diagnoses of ICC from the SEER database for the years 2000 to 2018. Ultimately, data from 11,753 ICC patients who met the criteria were obtained. The third edition of the International Classification of Diseases for Oncology (ICD-O-3) was used to identify ICC patients. ICC patients were selected based on ICD-O-3 site codes C22.1 (intrahepatic bile duct) or C22.0 (liver). ICD-O-3 histology codes 8010, 8020, 8040, 8070, 8041, 8140, 8144, 8160, 8161, 8162, 8163, 8260, 8310, 8480, 8490, and 8560 were used to identify ICC patients. Klatskin tumors, classified as extrahepatic tumors, were excluded from this study. Other exclusions were patients diagnosed through autopsy or death certificate, those with missing or unclear causes of death, patients diagnosed within 1 month prior to death, patients who underwent surgical treatment, patients with concurrent primary tumors, and those lacking detailed survival data. The specific selection process and criteria are detailed in Figure 1. The data extracted included information on patients’ year of diagnosis, age at diagnosis, gender, race, marital status, grade classification, tumor diameter, treatment modality (radiotherapy, chemotherapy, radiotherapy + chemotherapy, etc.), cause of death, survival time, and survival status. The study defined overall survival (OS) as the time from initial treatment to death for any reason or the end of follow-up, and cancer-specific survival (CSS) as the time from initial treatment to death due to ICC or the end of follow-up. The follow-up end date was December 2018.
Statistical analysis
OS and CSS were regarded as the primary outcome measures for this study. Categorical variables were represented by frequencies (percentages) and compared using the χ2 test. Survival curves were plotted using the Kaplan-Meier method, and survival differences were compared using the log-rank test. To identify potential prognostic factors, Cox univariate analysis was initially employed, followed by the inclusion of variables with a p-value < 0.05 in the Cox multivariate analysis. The results were presented as hazard ratios (HR) with their corresponding 95% confidence intervals (CI). The significance level (α) for testing was set at 0.05. All analyses were conducted using R software, version 4.3.0.
Results
Demographic characteristics
The criteria detailed in the methods section led to the identification of 11,753 cases of advanced unresectable ICC from the SEER database, spanning the years 2000 to 2018. A majority of these patients, 60.2%, were diagnosed between 2010 and 2018, compared to 39.8% diagnosed from 2000 to 2009. Concerning age distribution, 60.8% of patients were over 65, while the remaining 39.2% were under 65. The gender split was relatively even, with males accounting for 51.7% and females 48.3%. In terms of ethnicity, 77.3% were Caucasian and 22.7% were non-Caucasian. When examining marital status, we found that 54.3% of patients were married, whereas 41.7% were either unmarried or divorced. A substantial proportion of cases, 94.5% (11,109 of 11,753), resulted in the patient’s death. Regarding treatment strategies for advanced unresectable ICC, 38.5% (4531 cases) received chemotherapy alone (CT Alone), 4.1% (482 cases) received radiotherapy alone (RT Alone), 8.5% (996 cases) underwent combined chemotherapy and radiotherapy (CT + RT), and 48.9% (5744 cases) did not receive either treatment (NCT + NRT). Table I provides a detailed breakdown of these baseline characteristics.
Table I
Baseline characteristics according to treatment regimen
P-values computed from Pearson’s c2 test. CT – chemotherapy, RT – radiotherapy, NCT – non-chemotherapy, NRT – non-radiotherapy.
Survival analysis
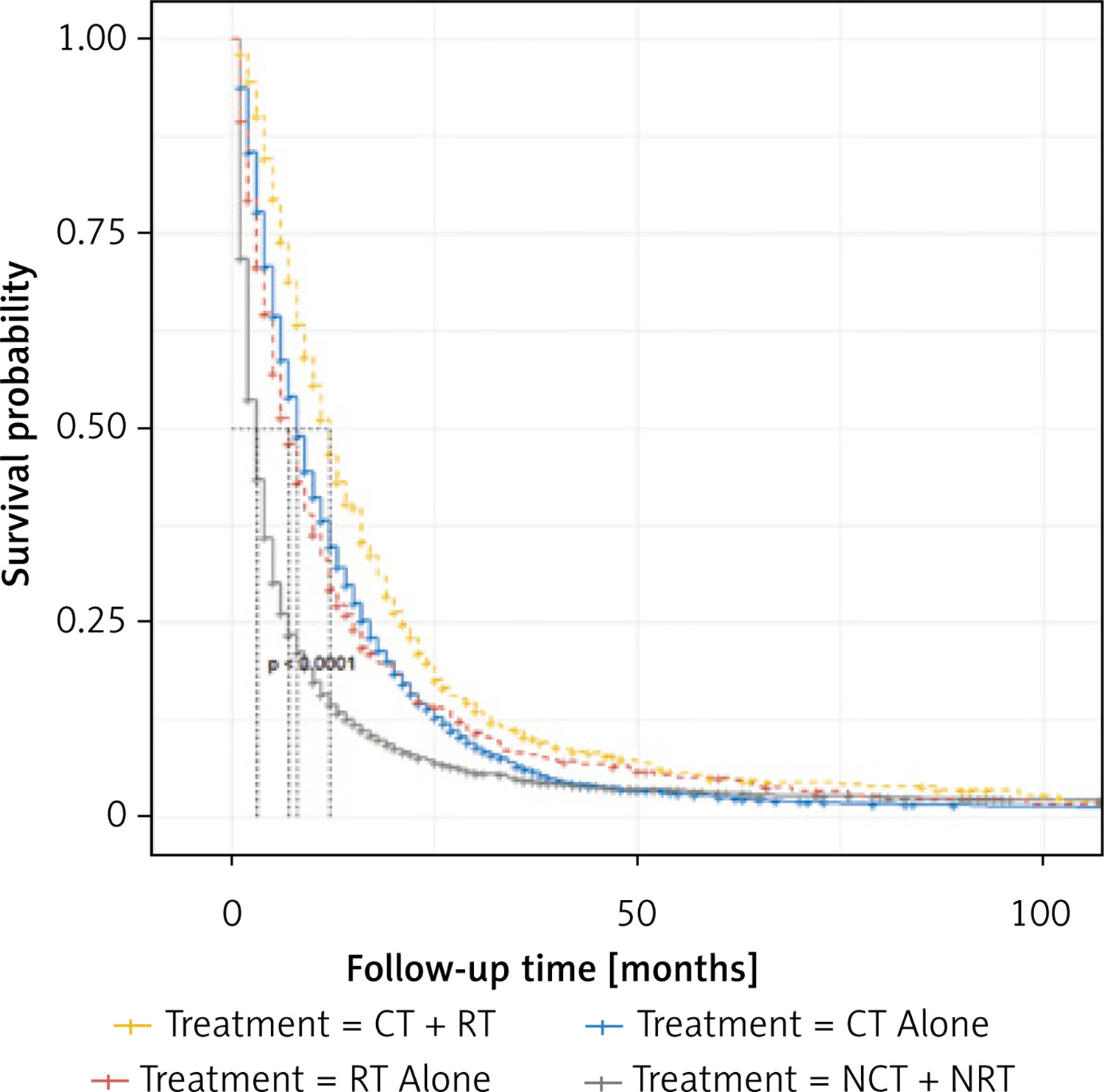
The survival analysis revealed that patients receiving combined chemotherapy and radiotherapy had a median OS of 12.00 months (95% CI: 11–13), superior to patients receiving either chemotherapy alone with a median OS of 8.00 months (95% CI: 8–9), or radiotherapy alone with a median OS of 7.00 months (95% CI: 6–8). The shortest OS of 3.00 months (95% CI: 3–3) was observed among patients who did not receive either treatment. The OS difference between the combined treatment group and the other three groups was statistically significant (p < 0.0001), whereas no significant difference was found between the chemotherapy alone and radiotherapy alone groups (p > 0.05). These OS trends are captured in the Kaplan-Meier curves in Figure 2.
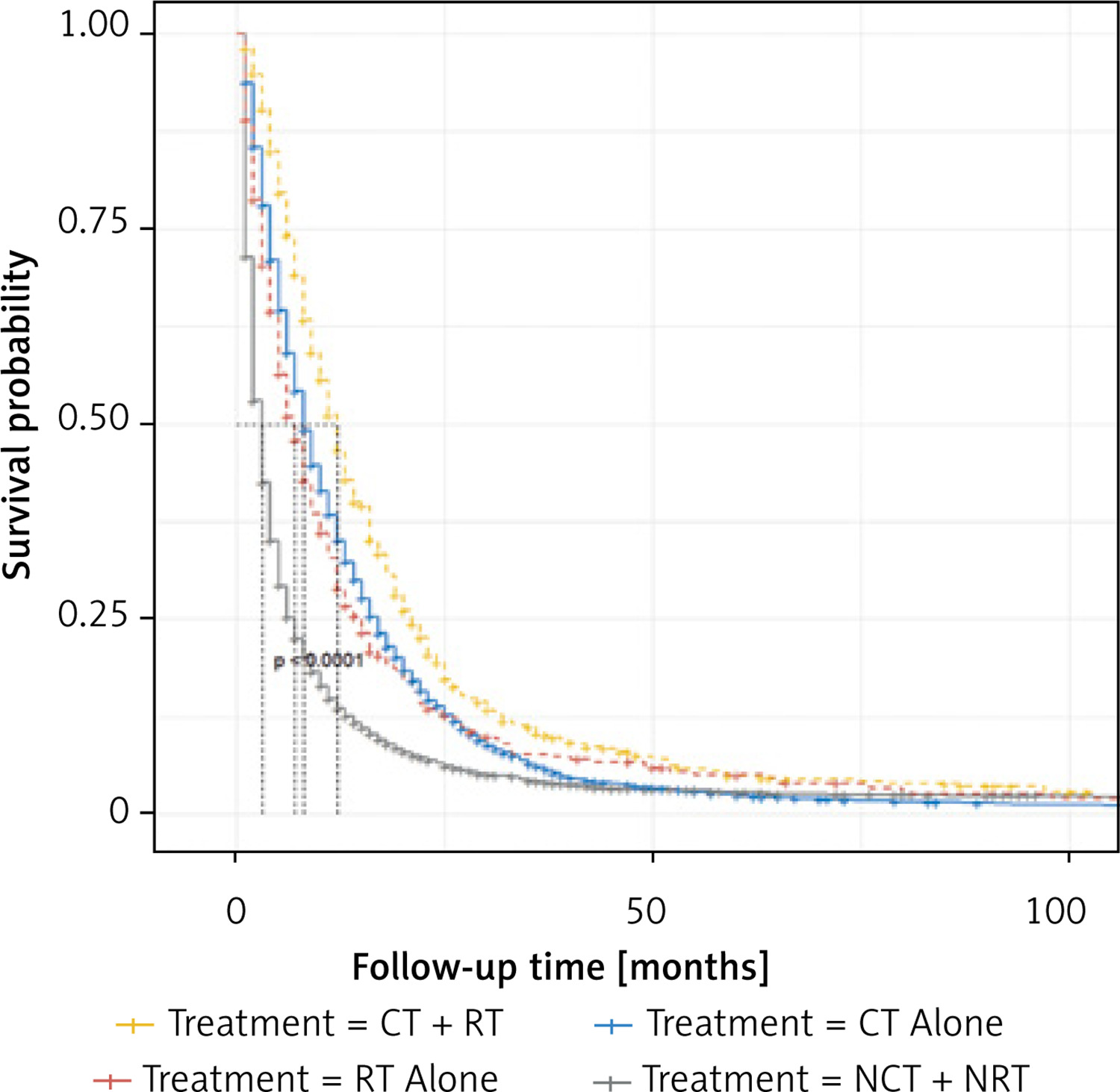
The CSS analysis echoed the OS analysis results. The median CSS for combined chemotherapy and radiotherapy was 12.00 months (95% CI: 11–13), for chemotherapy alone it was 8.00 months (95% CI: 8–9), for radiotherapy alone it was 7.00 months (95% CI: 6–8), and for those not receiving either treatment, it was 3.00 months (95% CI: 3–3). The CSS of the combined treatment group was significantly superior to the other groups (p < 0.0001), and the comparison between the chemotherapy alone and radiotherapy alone groups showed no statistically significant difference (p > 0.05). Figure 3 depicts the Kaplan-Meier curves for CSS.
Univariate and multivariate Cox regression analysis of OS
The univariate Cox proportional hazards regression model for OS highlighted the year of diagnosis, patient age, gender, marital status, grade classification, tumor diameter, and treatment modality as significant prognostic factors for unresectable advanced ICC patients (p < 0.05, Table II, Supplementary Figure S1). The multivariate model corroborated these results, further emphasizing patient age, gender, grade classification, tumor diameter, and treatment modality as independent prognostic factors (p < 0.05, Table II, Supplementary Figure S1). The multivariate analysis revealed the following associations: an increased risk of death with increasing age (HR = 1.204; 95% CI: 1.157–1.254, p < 0.001); a higher risk of death for male patients compared to female patients (HR = 1.117; 95% CI: 1.075–1.162, p < 0.001); an elevated risk of death for patients with Grade classification III–IV compared to those with Grade classification I–II (HR = 1.364; 95% CI: 1.273–1.462, p < 0.001). Moreover, patients with a tumor diameter ≤ 5 cm experienced significantly higher survival rates compared to those with a diameter > 5 cm (HR = 0.869; 95% CI: 0.816–0.925, p < 0.001). Finally, patients in the combined chemotherapy and radiotherapy group had a significantly lower risk of death compared to the chemotherapy alone group (used as reference) (HR = 0.779; 95% CI: 0.723–0.840, p < 0.001). Compared to the chemotherapy alone group, the radiotherapy alone group did not show a significantly higher risk of death (HR = 1.061; 95% CI: 0.960–1.174, p = 0.247), whereas patients who did not undergo either chemotherapy or radiotherapy had a significantly higher risk of death (HR = 1.785; 95% CI: 1.708–1.865, p < 0.001).
Table II
Predictors for overall survival of unresectable ICC patients
Univariate and multivariate Cox regression analysis of CSS
The univariate and multivariate Cox proportional hazards regression models for CSS produced results similar to those for OS. Both models identified the year of diagnosis, patient age, gender, marital status, grade classification, tumor diameter, and treatment modality as significant prognostic factors for unresectable advanced ICC patients (p < 0.05; Table III, Supplementary Figure S2). The multivariate model also depicted patient age, gender, marital status, grade classification, tumor diameter, and treatment modality as independent prognostic factors (p < 0.05, Table III, Supplementary Figure S2). The CSS multivariate Cox regression analysis identified several associations: an increased risk of death with increasing age (HR = 1.203; 95% CI: 1.154–1.254, p < 0.001); a higher risk of death for male patients, compared to female patients (HR = 1.112; 95% CI: 1.068–1.158, p < 0.001); a higher risk of death for patients with grade classification III–IV, compared to those with grade classification I–II (HR = 1.356; 95% CI: 1.263–1.456, p < 0.001). Unmarried or divorced patients also showed a higher risk of death compared to their married counterparts (HR = 1.044; 95% CI: 1.001–1.089, p = 0.044). Furthermore, patients with a tumor diameter ≤ 5 cm had a significantly higher survival rate compared to those with a diameter > 5 cm (HR = 0.861; 95% CI: 0.807–0.919, p < 0.001). Lastly, compared to the chemotherapy alone group (used as reference), patients in the combined chemotherapy and radiotherapy group exhibited a significantly lower risk of death (HR = 0.775; 95% CI: 0.718–0.837, p < 0.001). Compared to the chemotherapy alone group, the radiotherapy alone group did not show a significantly higher risk of death (HR = 1.070; 95% CI: 0.963–1.188, p = 0.207), while patients who did not receive either chemotherapy or radiotherapy had a significantly higher risk of death (HR = 1.824; 95% CI: 1.744–1.908, p < 0.001).
Table III
Predictors for cancer-specific survival of unresectable ICC patients
Discussion
Liver cancer ranks as one of the most prevalent tumors globally, with the incidence of new cases and associated deaths placing it sixth and third, respectively, among all malignant tumors [12, 13]. ICC is a rare but highly invasive primary liver malignancy, responsible for 10–15% of all primary liver cancers and approximately 10–20% of cholangiocarcinomas [14, 15]. Its prognosis is often poor, with an overall 5-year survival rate of about 8% [15]. Recent years have witnessed an upward trend in both the incidence and mortality of ICC [16]. However, its rarity has limited large-scale studies, resulting in a lack of concrete treatment conclusions for ICC patients [17]. Commonly employed clinical interventions encompass chemotherapy, radiotherapy, and combination therapy, but the comparative efficacy of these treatments lacks a unified study. To fill this gap, we used the SEER database to analyze the effectiveness of several treatment methods for unresectable ICC patients.
Our study encompasses 11,753 advanced unresectable ICC cases. The patients were treated with either CT alone, RT alone, CT + RT, or NCT + NRT. Median OS time was 12.00 months (95% CI: 11–13) for CT + RT patients, 8.00 months (95% CI: 8–9) for CT alone, 7.00 months (95% CI: 6–8) for RT alone, and 3 months (95% CI: 3–3) for NCT + NRT. The OS for the CT + RT group was notably higher than the other groups (p < 0.0001). No statistically significant difference was observed between the OS of the CT alone and RT alone groups (p > 0.05). The lowest OS was among those who did not receive either chemotherapy or radiotherapy (p < 0.0001). The results from the CSS survival analysis mirrored those from the OS survival analysis.
Univariate and multivariate Cox regression analyses indicated that age, gender, grade classification, tumor diameter, and treatment method were independent prognostic factors for advanced unresectable ICC patients (p < 0.05, Table II, Supplementary Figure S1). An increase in age correlated with a higher risk of mortality (HR = 1.204; 95% CI: 1.157–1.254, p < 0.001), which aligns with previous studies on the SEER database (18–34 years, 5-year mortality rate was 69.90%; 35–49 years, 5-year mortality rate was 77.86%; 50–64 years, 5-year mortality rate was 83.02%; ≥ 65 years, 5-year mortality rate was 91.41%; p < 0.0001) [18]. We speculate that this could be due to a higher incidence of comorbidities and poorer PS scores among the elderly. Male patients exhibited a greater risk of mortality (HR = 1.117; 95% CI: 1.075–1.162, p < 0.001). A study on the National Center for Health Statistics (NCHS) database [19] suggests that a higher mortality rate in male cholangiocarcinoma patients could be due to a higher incidence of concurrent cirrhosis and primary sclerosing cholangitis (PSC). Epidemiological data indicate a 27-fold increase in the risk of developing cholangiocarcinoma in cirrhosis patients and a 1560-fold increase in PSC patients. Additionally, men were found to have a higher risk of chronic liver disease and PSC compared to women [20–22].
Patients with a Grade III–IV classification, compared to those with Grade I–II, had a higher risk of death (HR = 1.364; 95% CI: 1.273–1.462, p < 0.001), possibly due to the increased malignancy, stronger invasion, metastasis ability, and poorer tissue differentiation associated with Grade III–IV tumors.
While the 7th edition of the AJCC TNM staging system for ICC considers factors such as the number of tumors, vascular invasion, intrahepatic metastasis, and invasion of adjacent organs, it does not include tumor size. The 8th edition, however, introduces a 5 cm threshold to differentiate between stages T1a and T1b [23]. Studies by Hwang et al. [24] and Spolverato et al. [25] revealed that a tumor diameter greater than 5 cm was an independent risk factor for tumor recurrence and patient survival, and was significantly associated with microvascular invasion and poorer tumor differentiation. Our study found that patients with a tumor diameter of ≤ 5 cm had a significantly improved survival period compared to those with a diameter > 5 cm (HR = 0.861; 95% CI: 0.807–0.919, p < 0.001), underscoring the prognostic value of tumor long diameter.
Though ICC has a relatively low incidence, most previous studies have focused on biliary tract cancer (BTC), with ICC being a subtype where no specialized treatment or chemotherapy regimen currently exists. Research has suggested that combined chemotherapy regimens are the main first-line treatment for advanced BTC. The phase III randomized controlled study ABC-02 [5] compared the efficacy of using gemcitabine alone versus the combination of gemcitabine and cisplatin for unresectable BTC. The median survival time (MST) in the combination therapy group (n = 204) was significantly better than that in the gemcitabine monotherapy group (n = 206) (MST: 11.7 months vs. 8.1 months; HR = 0.64; 95% CI: 0.52–0.80, p < 0.001). This study included 410 patients, including 80 (19.5%) ICC patients. Another controlled study on BTC conducted by Okusaka et al. [26] in Japan reported similar results, with ICC patients accounting for approximately 33.3% (28/84). The results showed that the combination therapy group was superior to the gemcitabine monotherapy group (MST: 11.2 months vs. 7.7 months, HR = 0.69; 95% CI: 0.42–1.13, p = 0.139). Another phase III randomized controlled trial involving BTC demonstrated that gemcitabine and cisplatin combined with S-1 (GCS) for unresectable BTC was superior to gemcitabine combined with cisplatin (GC) (median OS 13.5 months vs. 12.6 months; HR = 0.79; 90% CI: 0.628–0.996, p = 0.046) [27]. In this study, ICC patients accounted for approximately 31.7% (78/246). For unresectable ICC patients, although chemotherapy is recommended as a first-line treatment option, its efficacy is not ideal, and therefore more effective treatment methods are still needed. For ICC patients with symptoms related to local lesions and no distant metastasis, radiotherapy serves as a local treatment option. This study included various radiotherapy methods such as external beam radiotherapy, brachytherapy, combined external beam and brachytherapy, and radioactive isotope therapy. The advent of advanced external beam radiation therapy techniques has brought about potential benefits in treating biliary tract cancer [28–30].
Stereotactic body radiation therapy (SBRT) [6], a new form of radiation therapy, uses CT imaging and synchronized respiratory tracking technology to reduce errors caused by respiratory motion. This method ensures an adequate dose to the tumor while minimizing the radiation dose to normal liver tissue, thereby maximizing anti-tumor effects and reducing adverse events. Zhang et al. [6] studied 43 patients with unresectable ICC who received SBRT. The median treatment dose was 24–50 Gy (with a median dose of 40 Gy), and the median survival time was 12 months. The 1-year, 2-year, and 3-year overall survival rates were 51.2%, 32.6%, and 23.3%, respectively. Progression-free survival rates were 37.2%, 11.6%, and 4.7%, respectively, highlighting the potential benefit of this treatment modality.
Brachytherapy (BT) [7], a form of radiation therapy administered at close range, is able to deliver higher doses of radiation to a local tumor while sparing surrounding tissues, thus minimizing radiation-induced liver damage. Additionally, a meta-analysis [31] showed that transcatheter arterial yttrium-90 radioembolization (TRAE) facilitated downstaging for potential surgical resection in 11% of unresectable ICC cases. Furthermore, survival rate analysis revealed a combined median overall survival of 12.7 months, demonstrating the potential of these therapies.
In recent years, there has been an exploratory shift towards the combined use of radiotherapy and chemotherapy in treating ICC. Retrospective studies [32, 33] have suggested that this combined approach significantly outperforms either radiotherapy or chemotherapy alone in terms of tolerance, side effects, local control rate, progression-free survival (PFS), and OS. A study based on the SEER database [34] showed that the survival benefits of the group receiving combined radiotherapy and chemotherapy were higher than those of the group receiving radiotherapy alone. Furthermore, clinical phase II trial results for 41 cases of locally advanced ICC treated with radioembolization (SIRT) plus chemotherapy demonstrated an objective response rate of 39% at 3 months, a median progression-free survival of 14 months (95% CI: 8–17 months), and a median overall survival of 22 months (95% CI: 14–52 months). Nine (22%) patients could be downstaged for surgical intervention, and 8 (20%) patients ultimately achieved R0 (microscopically negative margins) resection. The study concluded that for unresectable ICC patients, SIRT combined with chemotherapy has an anti-tumor effect, and a significant proportion of patients can be downstaged for surgical intervention [8]. Another phase II study [35] indicated that combined local fluorouracil and high-dose conformal radiotherapy (median dose: 60.75 Gy) for inoperable intrahepatic malignant tumors (with ICC accounting for approximately 35.9%, 46/128) resulted in a median survival of 15.8 months. All of these studies highlight the potential value of combining radiotherapy and chemotherapy in the treatment of unresectable ICC.
A population-based cohort study, based on the Cancer Registry database of Taiwan [36], included 844 cases of inoperable, non-metastatic ICC patients. They were divided into four groups: synchronous radiotherapy and chemotherapy, sequential chemoradiotherapy, chemotherapy alone, and palliative symptomatic treatment. The results of multivariate analysis indicated that synchronous radiotherapy and chemotherapy could reduce the risk of death by 35% compared to palliative treatment, and it was superior to sequential chemoradiotherapy and chemotherapy alone. Our study enrolled 11,753 patients with advanced unresectable ICC, and yielded similar findings. Compared to the chemotherapy alone group, patients in the combined chemotherapy and radiotherapy group had a significantly reduced risk of death (HR = 0.775; 95% CI: 0.718–0.837, p < 0.001). The radiotherapy alone group did not have a significantly increased risk of death (HR = 1.070; 95% CI: 0.963–1.188, p = 0.207), while the groups that did not receive chemotherapy or radiotherapy showed a significantly increased risk of death (HR = 1.824; 95% CI: 1.744–1.908, p < 0.001). Therefore, combined chemotherapy and radiotherapy can improve the survival benefits for unresectable ICC patients.
As shown in Tables II and III, the differences in overall survival and cancer-specific survival between unresectable ICC patients during 2000–2009 and 2010–2018 were not statistically significant. This finding is based on a multivariate analysis that included patients undergoing various treatment modalities, such as chemotherapy alone (CT), radiotherapy alone (RT), chemoradiotherapy (CT + RT), and no chemotherapy or radiotherapy (NCT + NRT). Previous studies, including ABC-02 and BT22, have demonstrated that gemcitabine combined with cisplatin significantly improves survival outcomes in patients with advanced cholangiocarcinoma compared to gemcitabine monotherapy, establishing it as the standard treatment. While combined chemotherapy (e.g., gemcitabine + cisplatin) during 2010–2018 may have provided potential survival benefits compared to monotherapy in 2000–2009, other treatment modalities received by patients in this study (e.g., radiotherapy alone, chemoradiotherapy, or no treatment) likely introduced additional complex factors or potential confounders that could have mitigated the survival benefits of combined chemotherapy. This complexity may explain the absence of statistically significant survival differences between the two periods (2000–2009 vs. 2010–2018) among unresectable ICC patients. Moreover, due to the lack of detailed treatment information in the SEER database (e.g., specific drug types and treatment regimens), this study was unable to further compare the effects of monotherapy and combined chemotherapy on survival rates for unresectable ICC patients across the two time periods. This limitation should be acknowledged, and future research should aim to incorporate more granular treatment data to better evaluate the specific impacts of different treatment regimens on survival outcomes.
Our study cohort, comparable to the SEER database results, included 27 patients who received standalone chemotherapy (average age 58.59 ±10.02, tumor size 7.77 ±3.29 cm) and 9 patients who underwent chemotherapy combined with radiation therapy (average age 58.0 ±5.66, tumor size 6.36 ±2.66 cm). The median survival times were 9 (range: 2–24) months and 11 (range: 5–20) months, respectively (Supplementary Table SI). While the combined treatment cohort showed longer median survival, the difference was not statistically significant (p = 0.232). This might be attributable to the small sample size, indicating a need for further investigation with larger sample sizes.
The main novel contributions of this study include the following: First, based on large-scale data from the SEER database, we analyzed the impact of different treatment strategies (such as monotherapy, chemoradiotherapy, radiotherapy, and no treatment) on the survival rate of unresectable ICC patients, providing important insights for personalized treatment. Second, this is the largest comparative study to date on treatment strategies for unresectable ICC patients, ensuring the broad applicability and high statistical power of the results. Finally, the study highlights the limitations of the data, particularly the lack of treatment details, and emphasizes the need for future evaluations of treatment regimens through more precise clinical data and multi-center trials.
However, the study also has some limitations: Firstly, it lacks specific radiation therapy data. The SEER database does not provide details such as the dose, fractionation, field size, prescription point/volume, and other parameters of radiation therapy. It also lacks information on brachytherapy, including particle type, activity, prescription dose, and radiation-related toxicities. These factors could significantly affect treatment decisions and outcomes. Secondly, specific chemotherapy information is unavailable. The database does not record the types of chemotherapy drugs, combination regimens, and chemotherapy-related toxicities. For instance, the default first-line treatment for advanced biliary tract cancer is gemcitabine combined with cisplatin, a finding based on the ABC-02 study [5] published in NEJM in 2010. Patients diagnosed with ICC before 2010 might have received less effective or outdated chemotherapy regimens, potentially compromising treatment efficacy. Thirdly, patient-specific factors were omitted: Patients’ overall health, liver function, and comorbidities – crucial factors affecting survival – are not available in the SEER database. Fourthly, it was a non-randomized study, a design which inherently leads to selection bias and the influence of unregistered variables in the database. Fifthly, there was potential imbalance between treatment groups: Differences in patient characteristics or other unexplained variables between treatment groups may have resulted in biased outcomes.
In conclusion, our study suggests that patient age, gender, grade classification, tumor diameter, and treatment modality act as independent prognostic factors for unresectable advanced ICC patients. For these patients, combined chemoradiotherapy significantly improves the overall survival compared to either chemotherapy or radiotherapy alone. However, further confirmation of the role of combined chemoradiotherapy in the treatment of unresectable ICC patients necessitates prospective, large-sample, randomized controlled trials.