Introduction
Osteonecrosis is a condition marked by the destruction of bone tissue caused by an inadequate blood supply to bone cells [1]. Factors such as trauma, medications, alcohol, or metabolic disorders can trigger an immune response that interferes with bone repair, ultimately resulting in osteonecrosis [2–5]. Although osteonecrosis primarily occurs in the femoral head, it can also involve other regions [6]. Once diagnosed, it leads to a high rate of disability, severely diminishing patients’ quality of life and imposing a substantial burden on families and society [7].
Inflammation is a key factor in the development of steroid-induced osteonecrosis, particularly through the macrophage polarization process driven by tumor necrosis factor-α (TNF-α) [8, 9]. Dysregulated inflammation not only hinders bone repair but also aggravates tissue damage by producing reactive oxygen species and proteases, underscoring the complex interplay between inflammation and bone loss [10–12]. Furthermore, recent research has revealed links between osteonecrosis and various metabolic abnormalities, such as lipid metabolism disruptions, coagulation pathway irregularities, and alterations in linoleic acid metabolism, offering new perspectives for diagnosis and treatment [13, 14]. However, the precise interaction between inflammation and metabolic disturbances in the progression of osteonecrosis remains insufficiently understood.
In this study, we adopted a mediation Mendelian randomization (MR) framework to examine the potential role of metabolites in the causal pathway linking inflammatory cytokines to drug-related osteonecrosis. Our objective was to unravel the mechanistic pathways connecting inflammation, metabolism, and drug-related osteonecrosis. Additionally, we aimed to identify innovative targets and strategies for the prevention, early diagnosis, and treatment of this condition. The outcomes of this research may offer fresh insights into the underlying causes of drug-related osteonecrosis and support the development of precision medicine solutions for managing this challenging disease.
Material and methods
Study design
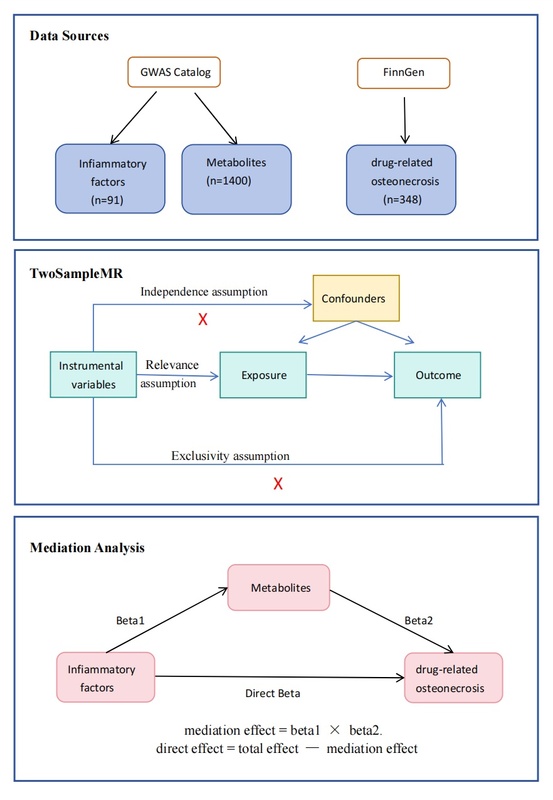
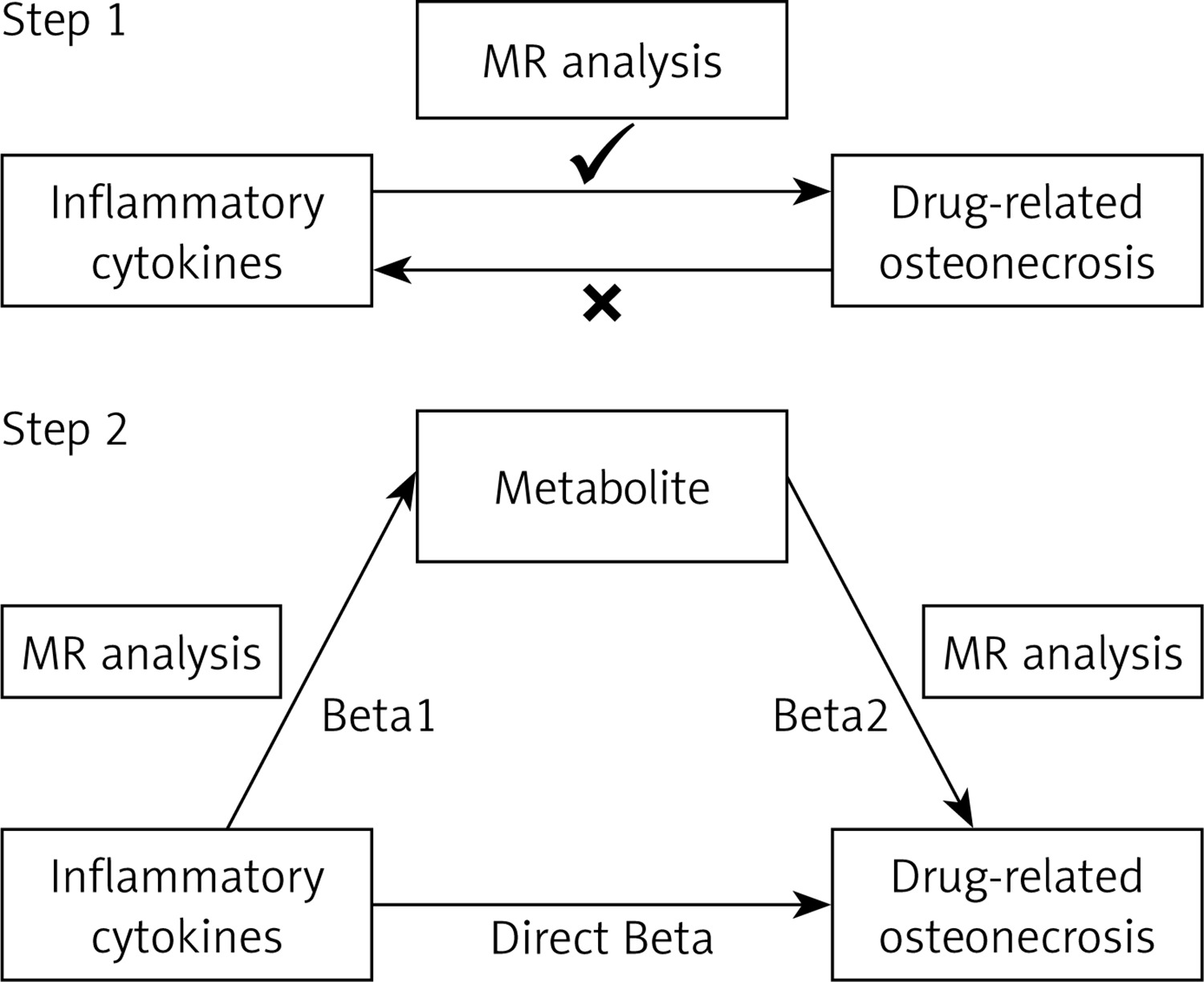
MR analysis relies on three fundamental assumptions: relevance, independence, and exclusivity [15]. This study was conducted in two stages. In the first stage, a two-sample MR method was applied, with inflammatory cytokines as the exposure and drug-related osteonecrosis as the outcome, to examine their causal relationship. Subsequently, reverse MR analysis was performed. The second stage focused on evaluating the mediating role of metabolites in the causal pathway between inflammatory cytokines and drug-related osteonecrosis. Inflammatory cytokines identified as significant in the first stage were used as exposure variables. Initially, the causal link between these inflammatory cytokines and potential mediators was tested, followed by an evaluation of the causal association between these mediators and drug-related osteonecrosis (Figure 1).
Data sources
All the data utilized in this study were obtained from publicly available genome-wide association study (GWAS) datasets; thus, no new ethics review board approval was necessary. The genetic data for inflammatory cytokines were derived from an earlier GWAS that included 91 plasma inflammatory cytokines, involving 14,824 individuals of European descent [16]. The genetic data for blood metabolites, which encompass 1,091 serum metabolites and 309 metabolite ratios, were sourced from the most recent GWAS summary dataset, which contained whole-genome genotyping data from 8,096 participants [17]. The data on drug-related osteonecrosis were obtained from the FinnGen R11 GWAS summary dataset (GWAS ID: finn-b-OSTEON_DRUGS), which comprised 348 cases and 453,385 control samples, available at this link: https://www.finngen.fi/en. To minimize potential bias arising from population heterogeneity, we specifically restricted the genetic composition of the study cohort to individuals of European ancestry.
Selection of tool variables
In MR analysis, SNPs are chosen as instrumental variables due to their strong association with the exposure variable. To address the potential limitation of obtaining too few SNPs with a p-value threshold of 5 × 10–8, which may hinder further analysis, we relaxed the threshold to p < 1 × 10–5 [18, 19]. To ensure the selected SNPs are independent, a linkage disequilibrium test was performed using an R2 threshold of 0.001 and a physical distance threshold of 1,000 kb, filtering out SNPs that exhibit linkage disequilibrium [20]. By applying these stringent criteria, we identified a robust set of instrumental variables that are strongly associated with blood metabolites or inflammatory factors and are mutually independent, minimizing the risk of violating the MR assumptions of independence and exclusivity. Furthermore, to validate the strength of the instrumental variables, we calculated the F-statistic for each SNP, excluding those with an F-statistic below 10 [21]. To enhance the reliability and accuracy of the analysis, we also excluded instrumental variables that could potentially affect the results through pleiotropy.
Statistical analysis
This study employed multiple MR approaches, including inverse variance weighted (IVW), MR-Egger regression, weighted median (WM), simple mode, and weighted mode methods. Given the robustness of the IVW approach for inferring causality, it was chosen as the primary method for estimating causal relationships [22]. A p-value below 0.05 was considered indicative of a significant causal association between the exposure and the outcome.
To ensure the robustness and reliability of the findings, several sensitivity analyses were performed. First, heterogeneity and pleiotropy in the causal estimates were examined using Cochran’s Q test and the MR-Egger intercept [23, 24]. Second, the MR-PRESSO method was employed to detect pleiotropic bias, with a p-value exceeding 0.05 indicating no substantial evidence of horizontal pleiotropy [24]. Additionally, a leave-one-out analysis was conducted to assess the influence of individual SNPs on the overall causal estimate [25].
To explore the causal pathways among blood inflammatory cytokines, metabolites, and drug-related osteonecrosis, a two-step MR analysis was conducted to evaluate whether metabolites mediate the relationship between inflammatory factors and osteonecrosis. Initially, a two-sample MR analysis was used to estimate the total causal effect of inflammatory factors on osteonecrosis, primarily relying on the IVW method while incorporating sensitivity analyses with MR-Egger regression and the WM approach [24]. Subsequently, two independent two-sample MR analyses were performed: the first estimated the causal relationship between inflammatory factors and metabolites, yielding the causal effect estimate beta1 [26], while the second assessed the relationship between metabolites and drug-related osteonecrosis, resulting in the causal effect estimate beta2 [26]. The mediating effects were calculated using the two-step MR approach as follows: mediation effect = beta1 * beta2. The direct effect was determined by subtracting the mediation effect from the total effect [26]. All MR analyses were implemented using R software (version 4.4.1) along with relevant packages such as “TwoSampleMR” and “MRInstruments.”
Results
The causal relationship between inflammatory cytokines and drug-related osteonecrosis
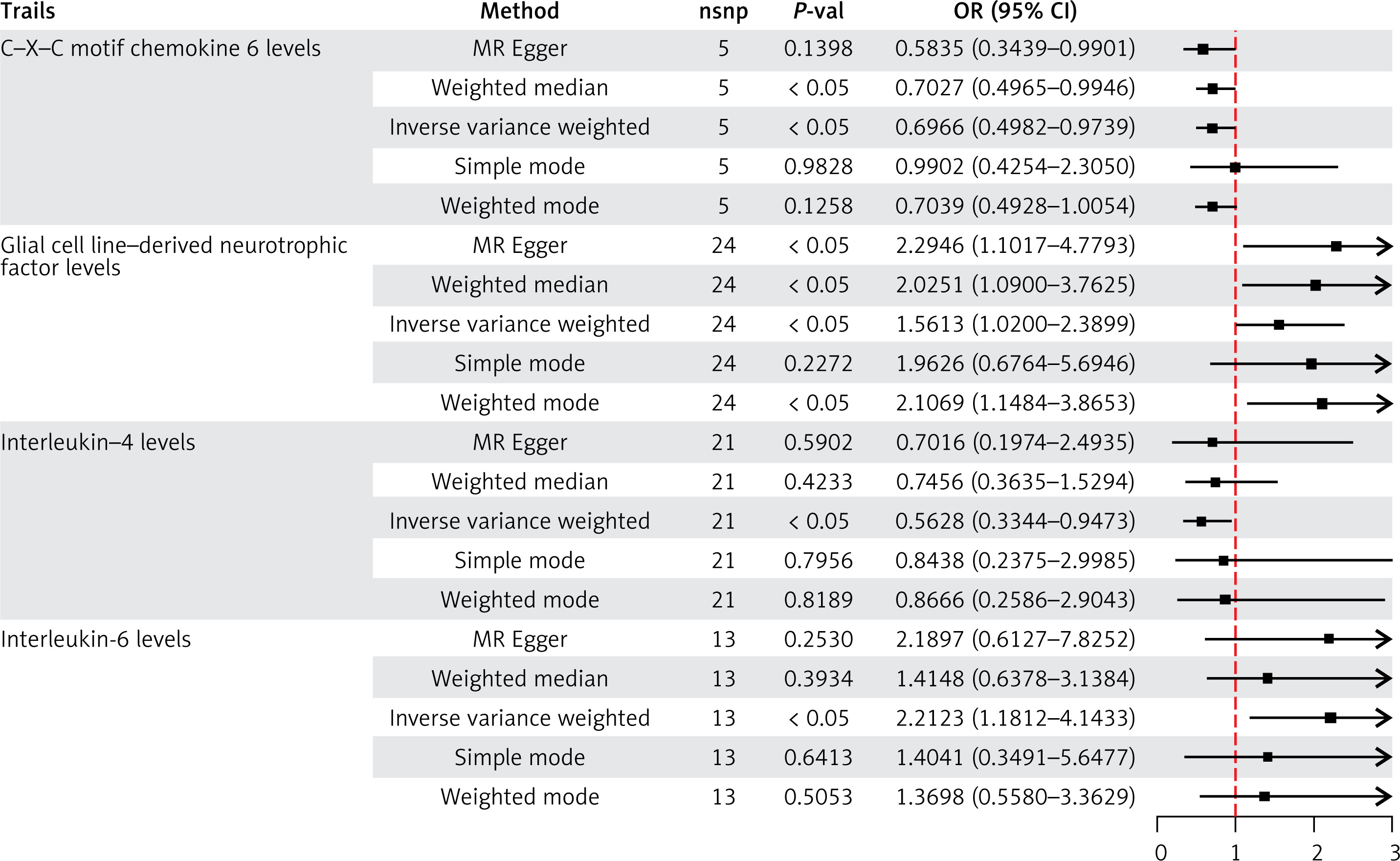
Using the IVW method as the primary analytical tool, the MR results indicated a significant causal relationship between the genetically predicted levels of four specific inflammatory cytokines and the risk of drug-related osteonecrosis. Notably, IL-4 (OR = 0.562; 95% CI: 0.334–0.947; p = 0.030) and CXCL6 (OR = 0.696; 95% CI: 0.498–0.973; p = 0.034) were identified as protective factors against drug-related osteonecrosis, while IL-6 (OR = 2.212; 95% CI: 1.181–4.143; p = 0.013) and GDNF (OR = 1.561; 95% CI: 1.019–2.389; p = 0.040) were found to be risk factors (Figure 2). Further sensitivity analysis showed no evidence of heterogeneity or pleiotropic bias among these four factors (Supplementary Table SI). Additionally, leave-one-out analysis further confirmed the reliability and stability of the results (Supplementary Figure S1). Subsequently, a reverse MR analysis was conducted, with drug-related osteonecrosis as the exposure variable and these four inflammatory cytokines as the outcomes. The results of the IVW method in the reverse analysis showed no causal relationship between drug-related osteonecrosis and these inflammatory cytokines, suggesting the feasibility of further research (Supplementary Table SII).
The causal relationship between metabolites and drug-related osteonecrosis
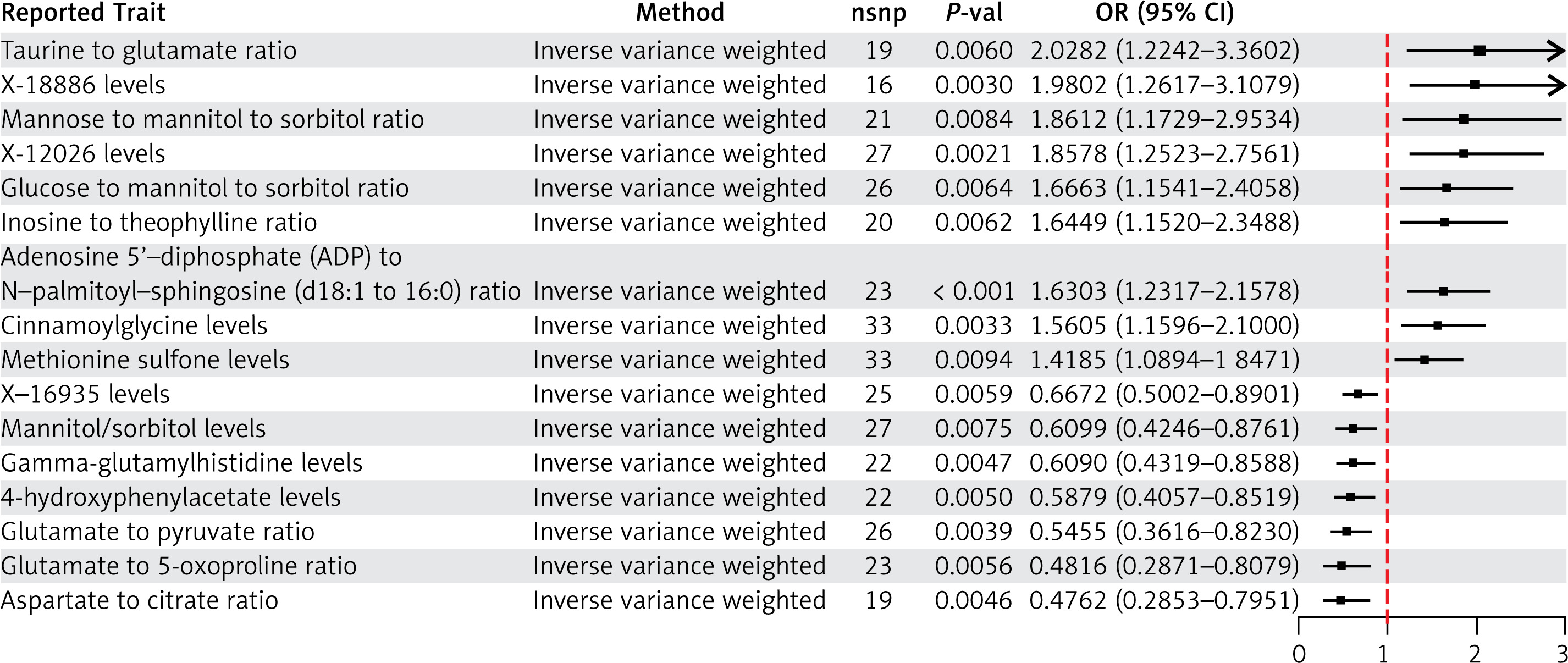
To verify the robustness of the MR analysis results, we performed cross-validation using five statistical approaches: IVW, MR-Egger regression, WM, simple mode, and weighted mode. Metabolites considered significant had to meet the following inclusion criterion: the OR values from all five methods consistently being either greater than 1 or less than 1. Additionally, pleiotropy was assessed (p > 0.05) to rule out the possibility of pleiotropic bias. Ultimately, 16 metabolites showing the strongest associations with drug-related osteonecrosis were identified, including 8 individual metabolites and 8 metabolite ratios (Figure 3). Sensitivity analysis revealed no evidence of horizontal pleiotropy or heterogeneity in the results (Supplementary Table SIII).
The causal relationship between inflammatory cytokines and metabolites
To investigate the mechanisms driving the onset and progression of drug-related osteonecrosis, we performed a mediation analysis to uncover pathways through which metabolites mediate the effects of inflammatory cytokines. Specifically, we analyzed the causal links between IL-4 and three metabolites and their subsequent influence on drug-related osteonecrosis. Our findings demonstrated a significant positive causal relationship between IL-4 and mannitol/sorbitol levels (OR = 1.128, 95% CI: 1.013–1.256, p = 0.026), indicating that elevated IL-4 levels may lead to increased mannitol/sorbitol levels. Furthermore, mannitol/sorbitol levels were significantly negatively associated with the risk of drug-related osteonecrosis (OR = 0.609, 95% CI: 0.424–0.876, p = 0.007), suggesting that these levels mediate IL-4’s protective effect on osteonecrosis.
We also identified a significant negative relationship between IL-4 and the mannose-to-mannitol-to-sorbitol ratio (OR = 0.881, 95% CI: 0.791–0.981, p = 0.021), while this ratio was positively associated with an increased risk of osteonecrosis (OR = 1.861, 95% CI: 1.172–2.953, p = 0.008). These results suggest that elevated IL-4 may lower the mannose-to-mannitol-to-sorbitol ratio, thereby reducing osteonecrosis risk. Similarly, a significant negative causal relationship was observed between IL-4 and the glucose-to-mannitol-to-sorbitol ratio (OR = 0.876, 95% CI: 0.787–0.974, p = 0.015). Conversely, this ratio was positively associated with the risk of drug-related osteonecrosis (OR = 1.666, 95% CI: 1.154–2.405, p = 0.006). These findings suggest that higher IL-4 levels may reduce the glucose-to-mannitol-to-sorbitol ratio, further mitigating osteonecrosis risk (Figure 4). Sensitivity analyses confirmed the absence of horizontal pleiotropy and heterogeneity (Supplementary Table SIV). Finally, the mediation effects of the three metabolites – mannitol/sorbitol levels, the mannose-to-mannitol-to-sorbitol ratio, and the glucose-to-mannitol-to-sorbitol ratio – were assessed in the causal pathway between IL-4 and drug-related osteonecrosis. The estimated mediation effects were –0.0598 (95% CI: [–0.1290, 0.0089]), –0.0785 (95% CI: [–0.1600, 0.0103]), and –0.0674 (95% CI: [–0.1400, 0.0054]), respectively (Table I).
Figure 4
Forest plot of MR analysis of the causal effects of IL-4 on mannitol/sorbitol levels, mannose to mannitol to sorbitol ratio, and glucose to mannitol to sorbitol ratio in drug-related osteonecrosis
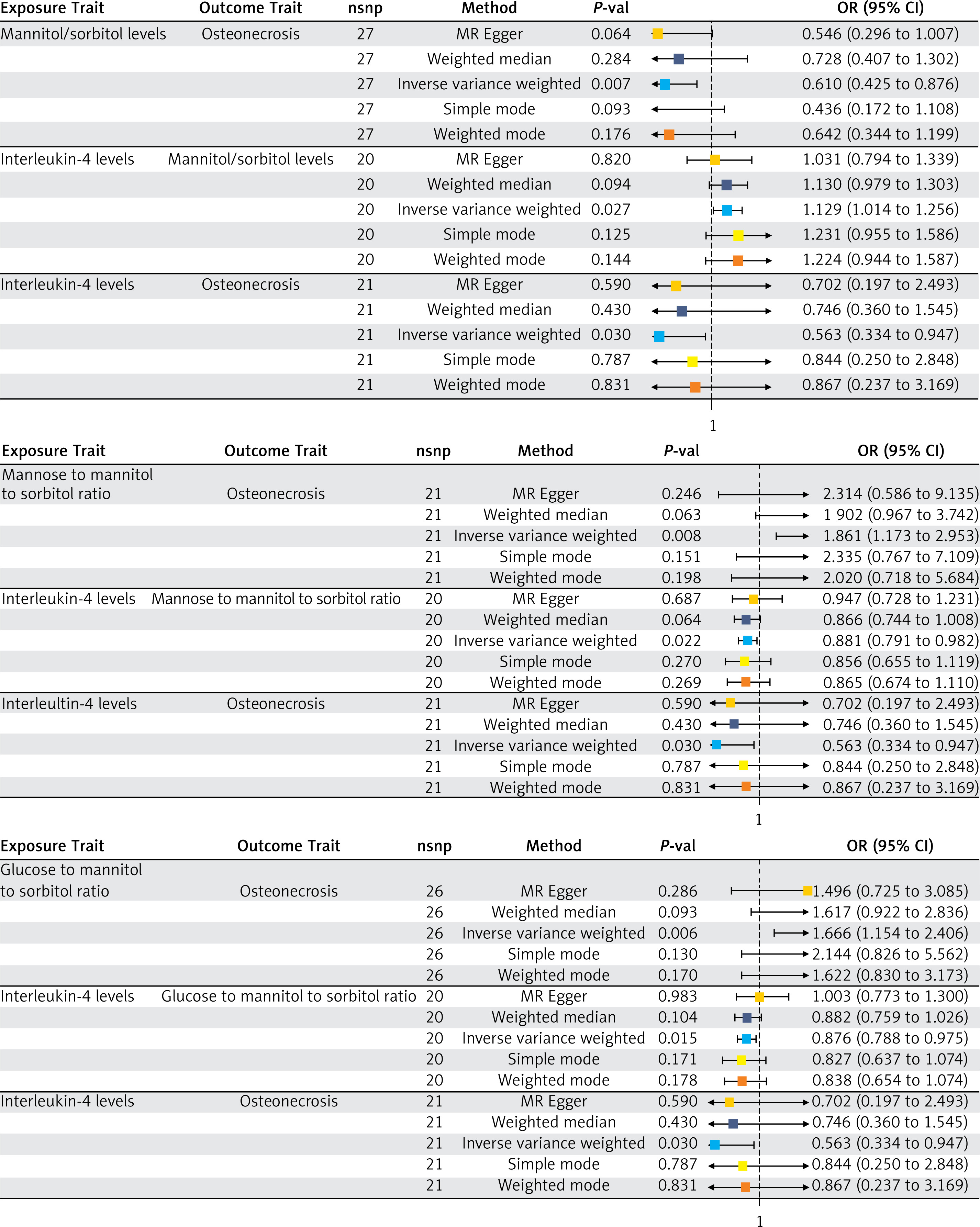
Table I
The mediation effect of IL-4 on drug-related osteonecrosis through mannitol/sorbitol levels, mannose to mannitol to sorbitol ratio, and glucose to mannitol to sorbitol ratio
Discussion
We explored the causal impact of inflammatory cytokines on drug-related osteonecrosis and examined possible mediators. The findings confirm that metabolites play a mediating role in the inflammatory cytokine-driven pathogenesis of drug-related osteonecrosis.
IL-4 is a versatile cytokine that plays a crucial role in regulating macrophage activity. It primarily promotes the polarization of macrophages to the M2 phenotype, which is vital in processes such as anti-inflammatory responses, tissue repair, and fibrosis. In particular, IL-4 functions by suppressing the expression of CD14 and inhibiting the release of pro-inflammatory cytokines such as IL-6 and tumor necrosis factor (TNF) [27]. We propose that in the context of drug-induced osteonecrosis, IL-4 may reduce tissue damage by limiting the secretion of key pro-inflammatory mediators. CXCL6, a member of the chemokine ligand family, has been found to be overexpressed in tissues affected by diabetic nephropathy. Research indicates that miR-20a targets CXCL6, thereby inhibiting the JAK/STAT3 pathway, promoting the proliferation of HK-2 cells treated with high glucose, and reducing both cell apoptosis and inflammation [28]. These findings have led us to further explore whether CXCL6 may similarly affect drug-related osteonecrosis through comparable molecular mechanisms and pathways.
Cytokines are pivotal in regulating immune responses, and their imbalance or excessive production is often linked to tissue damage and the progression of various diseases [29]. For instance, IL-6, a cytokine involved in inflammation, immune homeostasis, and bone metabolism regulation [30], demonstrates a minimal effect on bone remodeling under normal conditions. However, its expression significantly increases in pathological states, which may contribute to greater bone resorption, aggravated inflammation, and metabolic disturbances [31]. These findings highlight the intricate relationship between IL-6 and bone-related disorders. GDNF, a member of the transforming growth factor-β family, has been found to be elevated in degenerated intervertebral disc tissues, which have a pro-inflammatory microenvironment. This cytokine may play a pivotal role in the onset and spread of discogenic pain [32]. Building on these findings, we propose that inflammatory factors might regulate GDNF expression in drug-induced osteonecrosis cells. Additionally, the upregulation of GDNF could potentially enhance the transmission of inflammatory pain sensitivity. However, further research is necessary to better understand the underlying pathological mechanisms.
Mannitol and sorbitol are produced through the metabolism of fructose, mannose, and galactose, while glucose is converted to sorbitol through glycolysis and gluconeogenesis, and further oxidized into fructose [33, 34]. Under high glucose conditions, sorbitol dehydrogenase plays a crucial role in converting sorbitol into fructose. These metabolites can then form advanced glycation end products, which trigger liver metabolic changes, enhance de novo lipogenesis, and influence blood lipid levels, increasing cardiovascular disease risk [35, 36]. Our findings suggest that the levels of mannitol/sorbitol and related metabolites mediate IL-4’s role in osteonecrosis development. This is a significant discovery, as research on these metabolites is limited, and their mechanisms remain unclear. Future studies should explore how these metabolites mediate the interaction between inflammatory cytokines and drug-related osteonecrosis, offering new insights into disease mechanisms and therapeutic strategies.
This study investigates the causal link between inflammatory cytokines, metabolites, and the risk of drug-related osteonecrosis using MR analysis. However, there are limitations to consider. The GWAS data primarily come from European populations, which raises concerns about whether the findings can be generalized to other ethnic groups. The reliance on European cohorts may introduce population stratification bias, limiting the broader applicability of the results. Future research should include data from diverse ethnic groups to address this issue. Furthermore, while several metabolites linked to drug-related osteonecrosis have been identified, their precise role in disease development remains unclear, which limits the full interpretation of the study’s findings.
In conclusion, this study used MR to investigate the causal relationship between inflammatory cytokines and drug-related osteonecrosis, as well as the mediating role of metabolites. Four inflammatory cytokines were identified as causally linked to drug-related osteonecrosis. Mediation analysis further revealed that three blood metabolites, regulated through the IL-4 pathway, affect the risk of this condition. These findings provide valuable insights for prevention and treatment strategies.