Introduction
To improve the quality of life of the aging population, effective treatment of muscle-wasting (MW) diseases [1, 2] is needed [3–5]. One common approach is based on the use of exercise [3–11]. Many studies emphasize the importance of eccentric training [6–11]. As muscles regularly undergo eccentric contraction [6, 8], eccentric mechanotransduction appears to be a natural strategy for training muscle strength [6, 10] and the best activator of muscle mechanosensation [12], and one that may allow the reversal of MW changes [11, 13]. However, this reversal also depends on neuromuscular transmission (NT) [14], a self-contained factor known to stimulate neurogenic muscle atrophy and muscle fatty infiltration (MFI) [15].
Disuse MW changes to the shoulder caused by rotator cuff tear result in dysfunction of the upper limb, and hence a weakening of the second key pillar of life, independence, with such disability being particularly burdensome for the elderly [16]. The prevalence of rotator cuff tear is almost 50% in patients aged over 65 years [17], and its size is known to be a good predictor of the severity of MW or sarcopaenia [18]. Changes to the rotator cuff associated with MW are characterized by atrophy, muscle fibre loss, and muscle fatty infiltration (MFI) [19–21] also known as fatty degeneration (FD) [22].
Although various biomarkers have been proposed to measure the advancement of such MW changes [23], one of the best basic approaches to muscular study for this purpose is believed to be CT [24]. Therefore, CT images are commonly used to classify the degree of FD (MFI) in rotator cuff muscles according to the Goutallier et al. classification [22]; a score of grade 2 FD, i.e. tissue containing more muscle than fat, indicates borderline reversibility [22, 25].
A significant part of our knowledge of the development of changes to the rotator cuff muscles associated with disuse MW caused by tendon damage is derived from experimental research. One of the most widely used experimental models is the rabbit model [13, 26–34].
However, to the best of our knowledge, no human or animal data exist regarding the complex relationship between eccentric mechanotransduction, NT, and histomorphometric reversibility of MFI, in the case of advanced MW changes associated with muscle disuse.
The present study continues our previous work [13] by examining the reversibility of type I and II supraspinatus muscle fibre atrophy combined with MFI greater than second degree FD (MFI = 2.28) [29] according to Goutallier et al. [22], based on the rabbit model of disuse MW. The present work assumes the following hypotheses: 1) the presence of critical MFI changes to the supraspinatus corresponding to greater than second degree FD according to Goutallier et al. [22] is associated with an impairment of neuromuscular transmission highlighted by SFEMG; 2) in spite of FD greater than second degree, muscle mechanosensation is preserved and the implementation of eccentric mechanotransduction after successful supraspinatus tendon reconstruction may influence the reversibility of MFI; 3) the reversibility of MFI is correlated with muscle fibre type I and II hypertrophy.
Material and methods
The study was approved by the local Animal Bioethics Committee of the Medical University of Lodz (research protocol q/BO/207). The study used a previously described model of FD in the supraspinatus muscle of rabbits achieved 12 weeks after cutting the supraspinatus muscle tendon; the FD was evaluated as being greater than second degree (2.28) according to Goutallier et al. following CT examination [22]. Sixteen adult male rabbits of mixed breed (weight 3.8–4.6 kg) were anaesthetized with intravenous Vetbutal injection (30 mg/kg) (Biowet, Pulawy, Poland) supplemented by local infiltration with 1% lidocaine. The left shoulder was exposed, and after shaving and disinfecting the skin the lateral surgical approach was applied. The deltoid muscle was split and retracted, and about 3 mm of the supraspinatus tendon and its fibrocartilaginous part was resected and detached from the greater tubercle, as well as from the subscapularis and infraspinatus tendons (cut interdigitation-split length: 1 cm) [13, 30] The wounds were closed with layers, and the animals were allowed to move freely within a standard cage. The water was supplemented with metamizole sodium (Polpharma, Poland) to reduce postoperative pain for the first 3 postoperative days.
Twelve weeks after the procedure, the tendon was reinserted under the same anaesthetic conditions. According to our previous work on a similar rabbit supraspinatus model, 12 weeks was a sufficient period for development of grade > 2 FD (2.28) [29] according to Goutallier et al. [22]. Thus, the thin scar tissue and the edge of the supraspinatus tendon were resected, and the tendon was reattached to the abraded groove between the humeral head and the greater tubercle with the help of a modified Mason-Allen stitch [35] with a number 2 AMIFIL polyamide non-absorbable suture (Simpo, Poznan, Poland). The reattachment was performed under tension due to the shortening of the tendon. The suture was passed through the groove with the help of a needle and tied over the external cortex. The connections between the supraspinatus and infraspinatus, as well as the subscapularis, were reconstructed using an AMIFIL 3/0 polyamide non-resorbable suture (Simpo, Poznan, Poland). Very strong fixation was observed, and the tendon stump adapted well to the bone bed. The wound was closed in layers. The shoulder was not immobilized post-operatively.
After 6 weeks, the animals were moved from the standard cage to an open one 4 times as large every second week to allow more space for activity: daily changes of water and food were provided in opposite corners. Although two animals were euthanized 8 and 9 weeks after reattachment of the tendon due to an unknown general infection, they were not included in the histomorphometric study due to excessive loss of body weight. Twenty-four weeks after reattachment of the tendon, 10 animals were euthanized by intravenous application of a lethal dose of Vetbutal (100 mg/kg), and full thickness muscle samples were taken from the middle part of the supraspinatus, both from the operated and the non-operated limbs.
Histomorphometry
The muscle samples had previously been used to measure type I and type II muscle fibre diameter in a recent study [13]. In the present study, they were used to determine the cross-sectional areas of MFI regions within the muscle. For this purpose, the muscle samples were stained with haematoxylin and eosin. Care was taken to ensure that the cuts were perpendicular to the long axis of the muscle fibres. Histological morphometry was performed with an image analysis system consisting of a computer running MultiScan image analysis software (CSS-Poland) equipped with an Aver 2000 card (frame grabber, true colour, real time) and a colour TV camera linked to a microscope. This system was programmed to calculate the distance between 2 points and a regulated area of a structure using a stereological net with a regulated number of points. The cross-sectional areas of the MFI regions were measured with the help of a point counting method based on Weibl [36] using a stereological net. The point spacing was 16 μm. The total number of points in each net was 169, and the total area 0.37 mm2. Ten fields of the middle part of the muscle were studied under these nets.
SFEMG study
The SFEMG was performed on 4 randomly selected rabbits from a group of 14 animals 12 weeks after the supraspinatus tendon detachment. The animals were anaesthetized under identical anaesthetic conditions, and the supraspinatus muscle and the suprascapular nerve were exposed.
SFEMG stimulation studies were performed with Keypoint (Medtronic) apparatus using extra-muscular axonal stimulation techniques, which allowed direct muscle fibre stimulation to be avoided [16, 37–40]. Bipolar hook electrodes were placed under the suprascapular nerve. The axons were stimulated at 10 Hz (pulses of 50 μs duration). The strength of the stimulus used was 0.7–4 mA. Artifacts related to threshold stimulation were avoided by using supramaximal stimulation. A ring electrode around the ear provided grounding. Recordings were made from the middle part of the supraspinatus muscle with a 26 G × 40 mm SFEMG needle electrode. The high-pass filter was set at 1 kHz and the low-pass filter at 20 kHz. After introduction of the needle electrode into the muscle belly, its position had to be precisely adjusted to find the potentials.
When muscle fibre action potentials are recorded during repetitive nerve stimulation, the latency from the stimulus to the response is subject to some fluctuations. This variation is called neuromuscular jitter, and its value (in µs) is calculated as the mean consecutive difference (MCD) of successive stimulus-response intervals (SRI) using the following formula: MCD = [(SRI2 – SRI1) (SRI3 – SRI2) + ··· + (SRIn–1 – SRIn)]/(n–1) [16, 37].
The MCD was calculated automatically by the equipment software as the mean of the absolute differences of 100 consecutive inter-potential intervals between stimuli and single-fibre potential. Twenty potentials were recorded, and the mean MCD for 20 muscle fibres was then calculated during the examination of each muscle. To eliminate the possibility of the direct muscle stimulation only potentials with MCD values ≥ 3.0 µs were accepted for analysis. The number of abnormal potentials and potentials with blocking were recorded. The examination was performed on the operated side and then on the control side.
The upper limit of normal jitter is defined as the mean MCD of the control muscles plus 3 standard deviations [38]. The upper value of the MCD range of the control muscles is considered the individual normative value of a single muscle fibre [37].
Statistical analysis
A power analysis was performed (α = 0.05, 80% power). The arithmetic mean and standard deviation were calculated from the basic position measurements. The Shapiro-Wilk test was used to confirm whether the tested values were normally distributed, and the t-test and Wilcoxon test were used for further analyses depending on the distribution. Differences with p-values < 0.05 were considered significant. All calculations were performed using Statistica ver. 10 software (StatSoft, Inc., 2011, DASS, www.statsoft.com).
Results
The result of the power analysis was 99%. Significant differences were found between the operated and control sides with regard to MFI volume (Student’s t-test; p < 0.001) (Table I). No significant differences were found between the mean jitter values of the disuse and the control supraspinatus muscles (Wilcoxon test; p = 0.051) in the SFEMG examination.
Table I
The muscle fatty infiltration volume of rabbit supraspinatus muscle 6 months after the reconstruction of its tendon and its eccentric mechanotransduction
| Supraspinatus | Mean | Min. | Max. | SD |
|---|---|---|---|---|
| Operated | 4.6 | 3.2 | 6.2 | 1.1 |
| Control | 2.91 | 2.3 | 4.1 | 0.61 |
| Operated | Control | |||
| 4.2 | 2.3 | |||
| 3.5 | 2.5 | |||
| 3.2 | 2.9 | |||
| 4.1 | 2.7 | |||
| 3.4 | 2.6 | |||
| 5.2 | 4.1 | |||
| 4.6 | 3.3 | |||
| 6.1 | 2.8 | |||
| 5.5 | 3.4 | |||
| 6.2 | 2.5 |
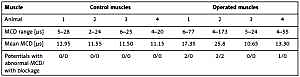
The mean MCD value of the unoperated control muscles was 11.79 ±80 µs (4–28), and the normative MCD value of control animals was 14.19 µs (11.79 ±2.4) (Table II). The normative MCD value of an individual muscle fibre in controls was 28 µs (Table II). Only 5 abnormal potentials (MCD) (6.5%) associated with the presence of blocking were observed within 2 fibres (2.5%) of the entire pool of 80 muscle fibres evaluated in the 4 operated muscles (Table II).
Table II
The results of SFEMG stimulation of the supraspinatus muscle 3 months after the tendon detachment. MCD - mean calculated difference between jitters in µs
Discussion
To our knowledge, this study is the first to document the correlation between eccentric mechanotransduction, NT and the histomorphometric reversibility of MFI in an animal model of changes resulting from critical disuse MW in the supraspinatus, i.e. grade > 2 FD according to Goutallier et al. based on CT classification [22].
Our present findings and those of previous studies [13] corroborate those of Gerber et al. [41], who reported that passive mechanotransduction of sheep infraspinatus can lead to partial reversal of muscle atrophy and the inhibition of fatty infiltration, as well as the study by Park et al. [42], who proved the reversibility of supraspinatus muscle atrophy after arthroscopic repair of its tendon. However, in contrast, Matsumoto et al. [31] did not report hypertrophy or the regression of fatty tissue of rabbit supraspinatus 3 months after reattachment of its tendon. These differences can be accounted for by differences in follow-up time, one study being twice the length of the other, the stitching technique, and the choice of rehabilitation program, as detailed previously [13]. In addition, Rubino et al. [32] report the progression of fatty degeneration and muscle atrophy halting 6 months after the rabbit supraspinatus tendon reconstruction. However, their study used a larger cage to stimulate animal activity, with water and food being placed in the same position within the cage.
The rabbit supraspinatus is responsible for the eccentric control of the shoulder when landing on the upper limbs after jumping. In the procedure described by Rubino et al. [32], the tendon was reinserted in its primary attachment side, i.e. the greater tubercle, resulting in the restoration of normal eccentric load, leading ultimately to a halt in the progression of MW changes. Our biomechanical modification of supraspinatus tendon reinsertion combined with its adequate resection resulted in greater tendon tension and eccentric load, thus fostering muscle fibre hypertrophy [13] and MIF reversibility. This hypothesis coincides with previous findings by Goldspink et al. [43]. The authors proved on the rabbit model that the stretch by itself prevents collagen accumulation and combined with electrical stimulation is also an anabolic signal inducing rapid and marked growth of skeletal muscle [43].
The development of MFI in cases of disuse MW follows a complex pathomechanism. Itoigawa et al. [44] proposed that a decrease in muscle tension caused by a tear in the tendon induces a reduction in the expression of Wnt10b mRNA, which is responsible for adipocytogenesis and fatty degeneration. Other studies [20, 45, 46] indicate that chronic unloading of muscle induced by a rotator cuff tear disrupts muscle homeostasis, leading to decreased myogenesis (Myf5), lowered metabolism (PPARα), and increased adipogenesis (CEBPα, Lep, Wnt10b). Liu et al. [47] postulate that the cellular origin of rotator cuff muscle MFI after its tendon rupture lies with muscle mesenchymal progenitor cells. Earlier works documented the influence of mechanotransduction on the inhibition of mesenchymal stem cell differentiation in adipocytes [48], and adipocyte proliferation [49, 50]. Hence, these findings and those of our present and past studies [13] confirm the positive impact of exercise on preventing increased in MFI [51].
Our current and previous findings [13], together with those of Rubino et al. [32], Gerber et al. [41], and Park et al. [42], suggest that regardless of the severity of disuse MW changes, mechanosensation is preserved in the muscle, and it is capable of responding to mechanotransduction. Eccentric mechanotransduction relates to the simultaneous generation of tensile, contractive, and compressive stresses [11]. Therefore, eccentric mechanotransduction has unique potential to counter the negative impact of MFI on muscle mechanosensation associated with stiffness and the number of adipocytes [52]. In addition, eccentric training also offers advantages of a greater impact on type II muscle fibre mechanosensation and less energetic demands than concentric training [11]. Collectively, these findings indicate that the eccentric load gradually activates the process of transduction of mechanical stimuli to the molecular cascade, thus stimulating muscle fibre hypertrophy and decreasing MFI, as confirmed by our previous [13] and current studies.
Moreover, these studies support data about the skeletal muscle memory related to previously encountered environmental stimuli and the retention of epigenetic information in skeletal muscle cells [53]. Furthermore, this skeletal muscle memory [53] seems to explain why, despite experiencing age-related progressive decline in muscle strength, seniors appear to retain the ability to produce eccentric torque [9].
The present study uses an experimental model described in a previous study [30]. It was found that the presence of grade 2 FD is connected with an increase of MFI by 18.34% (from 2.9% to 21.21%) over a 12-week period following tendon detachment [30]. During the same period, 18.2% atrophy was observed for type I muscle fibres and 19.7% for type II fibres from the same supraspinatus sample [30]. Thus, a 1% decrease in type I and type II muscle fibre size was related to a 1.01% growth in MFI (18.34 : 18.2%) for the former and 0.93% (18.34 : 19.7%) for the latter [30].
The previous [13] and current studies allow a unique assessment of the change in the diameters of type I and II muscle fibres regarding MFI regression by morphometric testing of the same muscle. Their results indicate that following eccentric training of the rabbit supraspinatus muscle after tendon stitching, 26.5% hypertrophy was observed for type I muscle fibres and 26.9% for type II, while MFI was reduced by 16.61%, i.e. from 21.21% to 4.6% (Table I) during the same period [13, 30]. Hence, a 1% increase of type I and type II muscle fibre diameter was found to be connected with a 0.63% reversal of MFI (16.61 : 26.5; 16.61 : 26.9) [13, 30]. Moreover, these results indicate for the first time that type I muscle fibres possessed the same quantitative impact on MFI reversibility as type II muscle fibres, which are mainly responsible for the loss of muscle mass with age [54, 55]); however, the final impact depends on the proportions of particular muscle fibre types [30, 54, 55]. Therefore, although most research studies regarding MW disorders have focused attention on type II muscle fibres, type I fibres possess underestimated potential and should be considered a separate physiotherapeutic target. This is especially important in light of the recent findings that the loss of satellite cells is more significant in the case of type II fibres than type I fibres [56]; however, muscle fibre type II hypertrophy is connected with an increase of satellite cell content [57].
Neuro-muscular junction dysfunction is currently recognized as an important co-mechanism in the development and progression of changes associated with disuse MW [14, 58–60]. Therefore, the present study examines whether the presence of critical MW changes to the supraspinatus, i.e. grade 2 FD according to the Goutallier et al. [22] CT scale, is associated with an impairment of neuromuscular transmission. The most sensitive test for the evaluation of neuromuscular transmission is SFEMG. SFEMG reveals neuromuscular transmission abnormalities caused by both pre- and postsynaptic conditions, and the usefulness of SFEMG has been confirmed also in animal studies [38–40].
Our SFEMG results corroborate those of a recent histopathological study on a very similar supraspinatus rabbit model, which also used 4 rabbits and the same follow-up time [33]. Gayton et al. [33] reported the occurrence of 19% MFI hyperplasia; however, this did not correlate with the histopathological state of the neuromuscular junction and was not influenced by the motor endplate. However, in the present study, a few potential relationships were recorded with pathological MCD and blocking (Table II), indicating that rabbits with advanced MW changes, i.e. FD > Grade 2 [29], demonstrated some electrophysiological symptoms of subclinical neuromuscular transmission disorders. The study also suggests that subclinical NT disorder depends more on the muscular side than the potential traction of the suprascapular nerve caused by supraspinatus muscle contraction [61] due to its tendon detachment. In our opinion, this is because the physiological activation of the suprascapular nerve is not blocked in the brain and occurs during every shoulder movement in which the supraspinatus muscle innervated by it is involved. It should also be mentioned that recent experimental studies [62] provide evidence that exercise training attenuates skeletal muscle atrophy through the activation of BDNF pathway. Moreover, the conducted studies also indicate that increasing the expression level of the FTO gene has an influence on the increase of skeletal muscle mass [63].
There are some limitations to our study. Firstly, as in previous studies, adult animals were used as test subjects; this may have influenced the muscle regenerative potential because the process is known to depend on age [55, 56, 64, 65]. What is more, as we know, the commonly used therapy for lipid disorders in old age can exacerbate MW [23, 66]. Secondly, the SFEMG study was limited to 4 rabbits; however, our findings are in line with those given by Gayton et al. [33]. However, our present SFEMG results, indicating MAC deviations and blockage of individual muscle fibres (Table II), indicate that dysfunction of subclinical neuromuscular transmission may be a signal of MW changes [66]. Thirdly, a limitation of our work is the inability to assess whether and to what extent the connective tissue hypertrophy has been reduced. Despite these limitations, our findings, as well as those from our previous study [13], provide new insight into the regenerative potential of muscle. It appears to depend on 3 types of fundamental structural change associated with MW, these being related to muscle fibres, MFI, and NT. Furthermore, it should be emphasised that the chosen model fulfils the strict requirements placed on animal models for MW evaluation [64]: the time points used for the study, i.e. 12 and 24 weeks, conform to human recommendations related to intervention with exercise formulated by the International Sarcopaenia Initiative [3].
Although it is difficult to directly transfer the results of animal tests to humans, close similarities exist between the response of the supraspinatus in animals following tendon detachment and that of rotator cuff rupture in seniors [67–69]. Furthermore, the results of our recent [13] and present studies, for the first time, provide extremely important quantitative histomorphometric data supporting the rationale for incorporating routine eccentric training in a program aimed at preventing the development and progression of MW changes or their reversal in ageing adults [11, 13].
In conclusion, the critical increase of muscle fatty infiltration associated with disuse changes in rabbit supraspinatus muscle, i.e. those greater than CT Grade 2 Fatty Degeneration, is substantially reversible by eccentric training. The SFEMG revealed no significant differences between the disuse and the control supraspinatus muscles; however, 6.5% of the examined muscle fibres exhibited NT disorders combined with blockade of conduction in 2.5% of fibres. A 0.63% decrease of MFI is correlated with 1% hypertrophy of type I and II muscle fibre diameter. The obtained results strongly support the rationale for incorporating routine eccentric training in a program aimed at preventing the development and progression of MW changes or their reversal in ageing adults.