Polycystic ovary syndrome (PCOS) is one of the most common endocrine disorders in adolescent girls, affecting an estimated 6–15% of this population depending on diagnostic criteria, pubertal stage, and racial and ethnic differences [1, 2]. It is also increasingly recognized as a disorder with a substantial metabolic component, characterized by insulin resistance, central adiposity, and early disturbances in lipid metabolism. Dyslipidemia is frequently reported in adolescents and young adults with PCOS, most commonly presenting as reduced high-density lipoprotein cholesterol (HDL-C) and elevated triglyceride (TG) levels [3]. The high and largely underdiagnosed prevalence of dyslipidemia in many populations underscores the importance of early-life determinants of cardiometabolic risk [4, 5].
However, traditional lipid measurements may not fully capture subtle abnormalities in lipid metabolism or the underlying atherogenic risk associated with insulin resistance. In adults, composite indices such as the triglyceride-to-HDL-C ratio (TG/HDL-C), total cholesterol-to-HDL-C ratio (TC/HDL-C), LDL-to-HDL-C ratio (LDL/HDL-C) and the atherogenic index of plasma (AIP) have been proposed as more sensitive markers of cardiometabolic risk than isolated lipid concentrations [6–8]. These ratios correlate with visceral adiposity, hepatic steatosis, inflammation, and insulin resistance, and in adult PCOS populations they have been widely shown to be elevated compared with controls [9].
Despite growing interest in these atherogenic indices, evidence regarding their relevance in adolescents with PCOS remains limited. Most available studies include small sample sizes and mixed pubertal stages or lack non-PCOS control groups. To address these gaps, we performed a study to investigate lipid metabolism and insulin resistance in teenage girls. By focusing on adolescence, a critical period for cardiometabolic risk development, this study provides new insight into the metabolic phenotype of young girls with PCOS and explores the potential clinical utility of atherogenic lipid ratios for early, personalized risk stratification.
Methods
Between January 2014 and December 2022, a retrospective, observational, cross-sectional study of consecutively referred patients was conducted at the Department of Pediatrics and Pediatric Endocrinology in Katowice. The study included 429 adolescent girls aged 13–18 years who were referred for the evaluation of menstrual irregularities and/or symptoms of hyperandrogenism. Patients were classified into PCOS and non-PCOS (control CG) groups using the international adolescent PCOS diagnostic recommendations proposed by Ibáñez et al. in 2017 [10].
Diagnosis required the simultaneous presence of persistent menstrual irregularity more than 2 years after menarche and hyperandrogenism. Menstrual irregularity was defined as oligomenorrhea (menstrual cycles longer than 45 days), secondary amenorrhea (absence of menstruation for more than 3 months), or primary amenorrhea (absence of menarche by 15 years of age). Hyperandrogenism was identified as either clinical, indicated by hirsutism with a Ferriman–Gallwey score of ≥ 8, and/or biochemical, defined by total testosterone levels exceeding 55 ng/dl. Participants who did not meet these criteria were assigned to the non-PCOS group (control group = CG).
Exclusion criteria for both groups included eating disorders, hyperprolactinemia (prolactin ≥ 721 mIU/l), adrenal disorders including congenital adrenal hyperplasia (defined by 17-hydroxyprogesterone ≥ 10 ng/ml and/or abnormal steroid metabolome in 24-hour urine collection), other secondary causes of hyperandrogenism or menstrual disturbances, and the use of medications influencing sex hormone levels or the hypothalamic–pituitary–gonadal axis within the preceding 3 months.
The study protocol included clinical and laboratory assessments. Clinical parameters comprised anthropometric measurements, with overweight defined as body mass index (BMI) between the 90th and 97th percentiles and obesity as BMI above the 97th percentile according to Poland-specific reference values [11]. Clinical history included age at menarche, gynecological age, and symptoms of hyperandrogenism. Hyperandrogenism was assessed clinically by the Ferriman–Gallwey hirsutism score and the presence of acne. Pelvic ultrasonography was performed to evaluate ovarian morphology and to measure right and left ovarian volumes.
Laboratory parameters included the lipid profile as well as glucose and insulin concentrations measured in the fasting state and at 120 min during a 75 g oral glucose tolerance test. Hormonal profile was assessed. Derived indices included the Homeostasis Model Assessment of Insulin Resistance (HOMA-IR), atherogenic lipid ratios (TG/HDL-C, TC/HDL-C, LDL-C/HDL-C), and the atherogenic index of plasma (log10[TG/HDL-C]). Within both groups, participants were stratified into subgroups according to BMI, distinguishing individuals with BMI below and at or above the 90th percentile. Statistical analyses were performed using Python 3.13.8 (Python Software Foundation, Wilmington, DE, USA).
Results
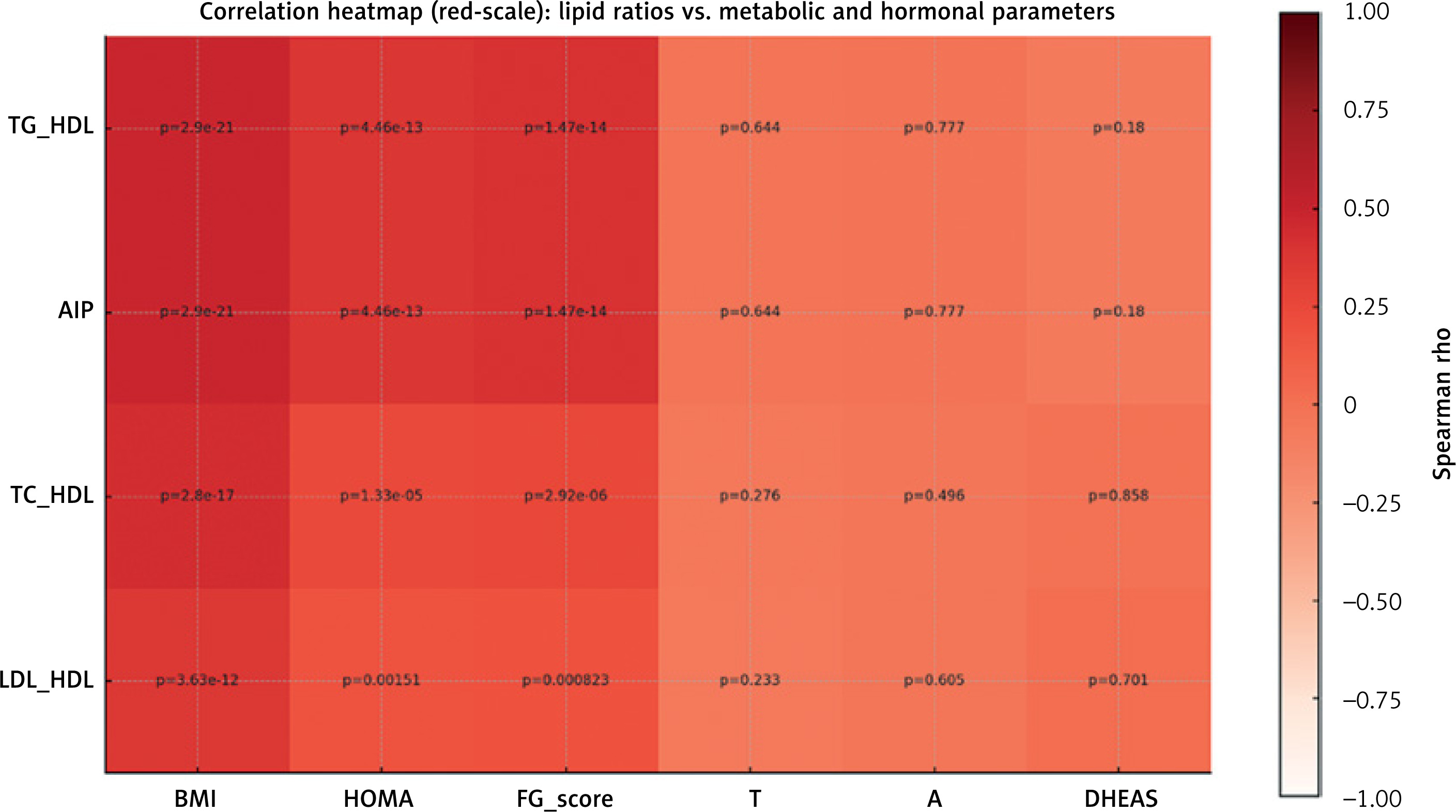
A total of 429 adolescent girls – of whom 191 (44.5% of the study group) met the diagnostic criteria for PCOS (PCOS group) and 238 (55.5% of the study group) were classified as non-PCOS controls (control group, CG) – were included in the analysis. In the PCOS group, 94 (49.2%) patients and in the CG group, 97 (40.8%) patients had BMI > 90th percentile. Clinical characteristics of participants are shown in Table I. Metabolic parameters and atherogenic lipid ratios stratified by PCOS status and BMI percentile are summarized in Table II. Across the entire cohort, atherogenic lipid ratios were significantly associated with markers of adiposity and insulin resistance. As shown in the correlation heatmap (Figure 1), TG/HDL-C and AIP demonstrated the strongest associations, with moderate positive correlations with BMI (ρ ≈ 0.48, p < 0.001) and HOMA-IR (ρ ≈ 0.38, p < 0.001).
Table I
Clinical characteristics of study population
Table II
Metabolic characteristics and atherogenic lipid ratios in study population
[i] BMI – body mass index, PCOS – polycystic ovary syndrome, CG – control group (non-PCOS); Glucose 0 min – fasting glucose, glucose 120 min – glucose 120 min during oral glucose test (OGTT), HOMA-IR – homeostatic model assessment for insulin resistance, insulin 0 min – fasting insulin, insulin 120 min – insulin 120 min OGTT, FIGR – fasting insulin-to-glucose ratio, HDL-C – high-density lipoprotein cholesterol, LDL-C – low-density lipoprotein cholesterol, TC – total cholesterol, TG – triglyceride, p = All PCOS vs. All CG, p1 = PCOS BMI < 90 pc vs. PCOS BMI ≥ 90 pc, p2 = CG BMI < 90 pc vs. CG BMI ≥ 90 pc, p3 = PCOS BMI < 90 pc vs. CG BMI < 90 pc, p4 = PCOS BMI ≥ 90 pc vs. CG BMI ≥ 90 pc.
Figure 1
Correlation heatmap of atherogenic ratios with metabolic and hormonal parameters in the total cohort
A – androstenedione, DHEAS – dehydroepiandrosterone, FG-score – Ferriman-Gallwey score, HDL-C – high-density lipoprotein cholesterol; LDL-C – low-density lipoprotein cholesterol, T – total testosterone, TC – total cholesterol, TG – triglycerides, BMI – body mass index, HOMA – homeostatic model assessment for insulin resistance.
A multivariate logistic regression model was constructed to identify independent predictors of insulin resistance (defined as HOMA-IR ≥ 75th percentile (14)). The model included TG/HDL-C, BMI, chronological age, and PCOS status. BMI was the only statistically significant independent predictor (OR 1.17 per kg/m2 increase; 95% CI 1.06–1.28; p = 0.0009). TG/HDL-C was not statistically significant (OR = 1.45; 95% CI 0.97–2.17; p = 0.068). Neither age nor PCOS status was a significant predictor.
Discussion
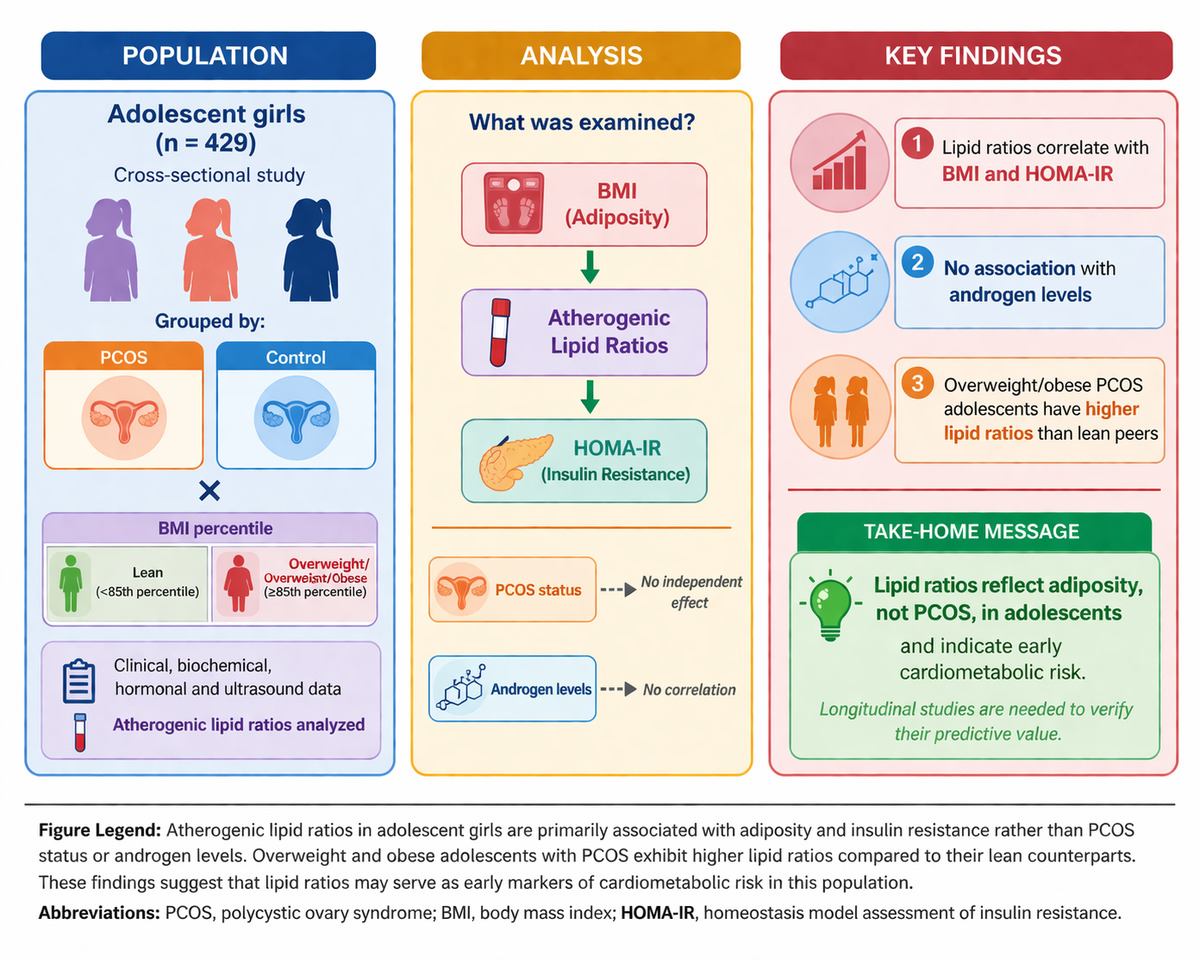
In this large, clinically well-characterized adolescent cohort, we observed that atherogenic lipid ratios were closely associated with adiposity and insulin resistance and only weakly associated with hyperandrogenism. These findings indicate that, in adolescents, atherogenic lipid ratios cluster with markers of metabolic burden rather than hormonal hyperandrogenism. When adolescents were stratified by both PCOS status and BMI percentile, the most adverse metabolic profile consistently clustered in the high-BMI strata, with PCOS adding only a modest incremental shift. This pattern supports the central concept that, during adolescence, atherogenic lipid ratios primarily reflect the metabolic burden of excess adiposity and insulin resistance, rather than serving as disease-specific biomarkers of PCOS status [12, 13].
Atherogenic lipid ratios such as TG/HDL-C and the atherogenic index of plasma were closely associated with BMI and surrogate markers of insulin resistance, while their relationships with biochemical hyperandrogenism were negligible.
In the adult population, we can observe a correlation between elevated androgen levels and abnormal lipid profiles, as well as a higher incidence of dysglycemia, which increases with the severity of the androgenic phenotype [14–16]. Our study of adolescent patients did not demonstrate a similar correlation. A possible reason for this finding, which merits further analysis, is the effect of androgens over time and their impact on the lipid profile after long-term exposure to their excess. Further research is necessary to determine whether the duration of hyperandrogenemia is a key factor in lipid profile abnormalities in this case.
From a clinical perspective, atherogenic lipid ratios may serve as pragmatic tools for early identification of adolescents with PCOS who are at increased metabolic risk, particularly those with overweight or obesity. However, they should not be used as screening or diagnostic markers for PCOS. Comprehensive metabolic risk assessment in adolescent PCOS should prioritize evaluation of adiposity and insulin resistance, with lipid ratios interpreted as complementary indicators of cardiometabolic burden.
From a clinical standpoint, these data support the interpretation that atherogenic lipid ratios in adolescent PCOS, such as TG/HDL-C and AIP, function as risk-enrichment markers for identifying individuals with a more adverse metabolic phenotype, particularly those with overweight or obesity, higher insulin concentrations, and elevated HOMA-IR.
This distinction has practical importance in adolescent care, where PCOS diagnosis is challenging due to physiological pubertal variability and where diagnostic guidelines appropriately emphasize persistent irregular cycles and hyperandrogenism after exclusion of mimicking disorders [1]. In our cohort, the absence of meaningful associations between lipid ratios and biochemical hyperandrogenism further supports the view that lipid indices should be positioned as metabolic monitoring tools rather than as endocrine diagnostic proxies.
Due to the increased risk of carbohydrate and lipid metabolism disorders among PCOS patients, special attention should be paid to lifestyle modifications, which should be an integral part and foundation of PCOS care. Recent reports emphasize the importance of a balanced diet and physical activity in improving both hormonal and metabolic parameters. Early patient education, starting in the teenage years, may result in a reduction of cardiometabolic risk in the future, improved reproductive health, and a positive impact on quality of life, and eating and activity habits may become an integral part of living with PCOS [17].
This study has several limitations. The study group does not reflect the general population, as it consisted of patients referred for evaluation of menstrual disturbances and hyperandrogenism, which may introduce selection bias. Additionally, the retrospective, observational, cross-sectional, and single-center design limits causal inference and generalizability of the findings. Insulin resistance was defined using a cohort-specific threshold (HOMA-IR ≥ 75th percentile), which may limit comparability with other studies and reduce external validity. Further studies on larger and more diverse populations are needed to confirm these results.
Artificial intelligence-based image generation tools were used to assist in the design of the graphical abstract. The authors critically reviewed, edited, and validated the final figure and take full responsibility for its accuracy and originality.