Stroke, resulting from disrupted cerebral perfusion, is the second leading cause of death and the third leading cause of disability worldwide, with over 13.7 million new cases annually [1–3]. This burden underscores the need for effective preventive strategies.
Skeletal muscle exerts critical metabolic functions in glycemic control and inflammatory modulation. Aging is accompanied by progressive muscle loss and fatty infiltration, impairing contractile function. Sarcopenia – defined by declines in muscle mass, strength, and physical performance – is an established risk factor for stroke [4]. Handgrip strength (HGS), a surrogate for overall muscular strength, predicts incident stroke [5]. However, strength declines more rapidly than mass, indicating dissociated trajectories; thus, comprehensive muscle assessment requires concurrent evaluation of both parameters. The muscle quality index (MQI), defined as HGS divided by appendicular skeletal muscle mass (ASM), quantifies strength per unit mass and is increasingly recognized as a robust health indicator [6, 7].
Although the association between sarcopenia and stroke has been extensively investigated using HGS, evidence specifically linking MQI to stroke remains scarce. To address this gap, the present study analyzed NHANES data to examine the relationship between MQI and stroke prevalence, with particular emphasis on potential nonlinearity and threshold effects.
Methods
Study population
Data were derived from the NHANES 2011–2014 cycles. Detailed methodologies are publicly available on the NHANES website. Among 19,931 participants initially screened, 5,149 adults aged 20–59 years were included after exclusions (Supplementary Figure S1).
Exposure and outcome
MQI was calculated according to Lopes et al. [6] as the sum of bilateral handgrip strength (Takei dynamometer) divided by ASM (dual-energy X-ray absorptiometry (DXA)). Participants were categorized into normal (≥ –1 SD), low (–1 to –2 SD), and extremely low (< –2 SD) MQI using ethnicity- and sex-specific cutoffs derived from a young reference population (age 20–39 years, normal body mass index (BMI)).
Stroke history was defined by a self-reported physician diagnosis. Participants answering “Yes” to “Has a doctor ever told you that you had a stroke?” were classified as having stroke; those answering “No” as non-stroke; “Didn’t know” were excluded.
Covariates
Potential confounders included sociodemographic factors (age, sex, ethnicity, marital status, poverty income ratio (PIR), education, body mass index (BMI)) and cardiovascular risk profiles (smoking, alcohol, physical activity, hypertension, diabetes, hypercholesterolemia).
Statistical analysis
Continuous variables were presented as mean ± SD, categorical variables as percentages. Group comparisons employed t-tests and χ2 tests. Three logistic regression models assessed the MQI–stroke association: Model 1 (unadjusted); Model 2 (adjusted for demographics, socioeconomic status, BMI); and Model 3 (additionally adjusted for cardiovascular risk factors).
Nonlinear relationships were examined using smooth curve fitting and two-piecewise linear regression. Subgroup and interaction analyses evaluated effect consistency. All analyses were conducted using R 4.1.1 and EmpowerStats, with significance set at p < 0.05. NHANES sampling weights were not applied, as the primary aim was internal validity rather than nationally representative estimation.
Results
Table I summarizes the baseline characteristics of the 5,149 participants (mean age: 38.8 years; range: 20–59 years; 51.1% male). Among them, 65 (1.3%) reported a history of stroke and 186 (3.6%) a history of cardiovascular disease.
Table I
Baseline characteristics of participants in the NHANES (2011–2014) by MQI groups
When stratified by MQI category (normal, low, and extremely low), significant differences were observed across the three groups. Participants with lower MQI levels were older, more likely to be female, and exhibited a higher burden of adverse socioeconomic factors – including lower income and education level and unmarried status – as well as unfavorable cardiovascular risk profiles (elevated BMI, current smoking, hypertension, diabetes, hypercholesterolemia, and physical inactivity) (all p < 0.01). Racial composition also differed significantly among the groups (p < 0.001).
Notably, a graded association was evident for both stroke and cardiovascular disease prevalence. The highest proportions were observed in the extremely low MQI group, followed by the low and normal MQI groups (stroke: 2.12%, 1.92%, and 0.66%, respectively; cardiovascular disease: 6.61%, 3.84%, and 2.25%, respectively; both P for trend < 0.001). Missing data information was described in Supplementary Table SI.
Associations between MQI and stroke
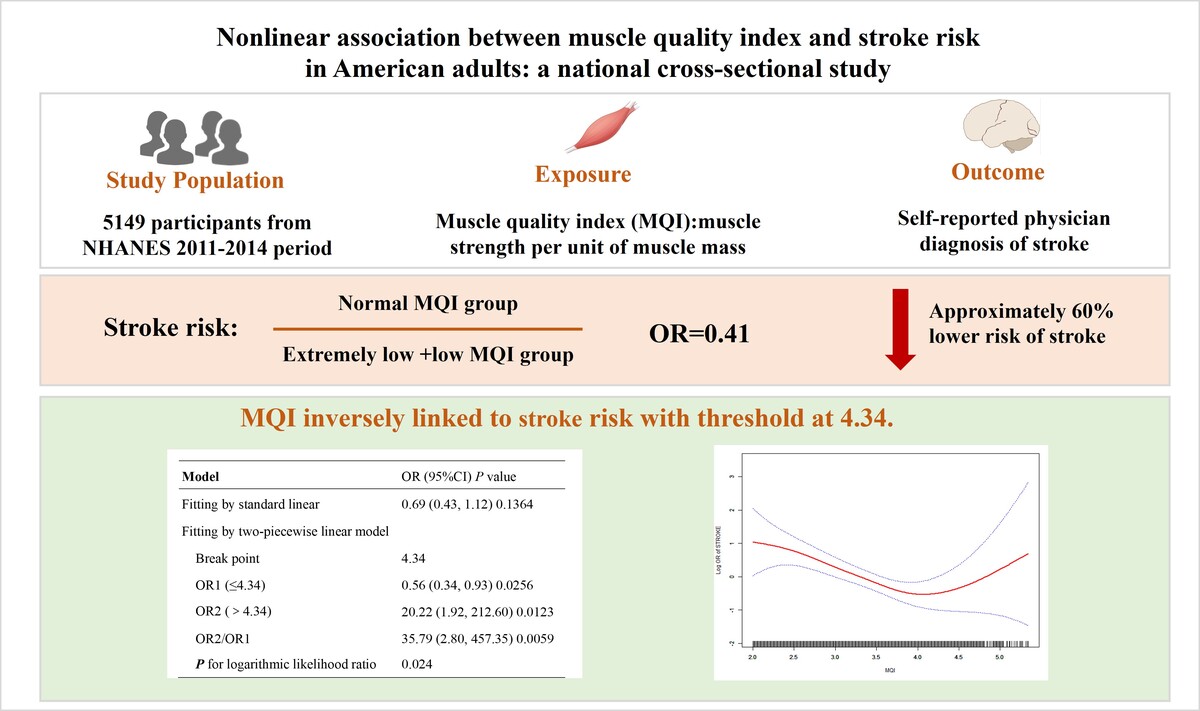
In the fully adjusted model, the normal MQI group had approximately 60% lower odds of stroke compared with the extremely low group (Supplementary Table SII).
A nonlinear relationship between MQI and stroke was suggested by generalized additive models (Figure 1). A two-piecewise logistic regression identified an inflection point at an MQI of 4.34 (log-likelihood ratio test, p = 0.024). Below this threshold, higher MQI was significantly associated with lower stroke prevalence (OR = 0.56, 95% CI: 0.34–0.93, p = 0.026). Above the threshold, the model suggested a positive association; however, this estimate was highly imprecise, as indicated by a wide confidence interval (OR = 20.22, 95% CI: 1.92–212.60, p = 0.012; Table II), likely due to a small number of participants with very high MQI values. This finding should therefore be interpreted with caution.
Figure 1
The results of smooth curve fitting analysis between muscle quality index and stroke. Age, sex, ethnicity, body mass index, poverty income ratio, marital status, education level, smoking status, alcohol consumption, hypertension, diabetes, hypercholesterolemia and physical activity were adjusted in the restricted cubic spline
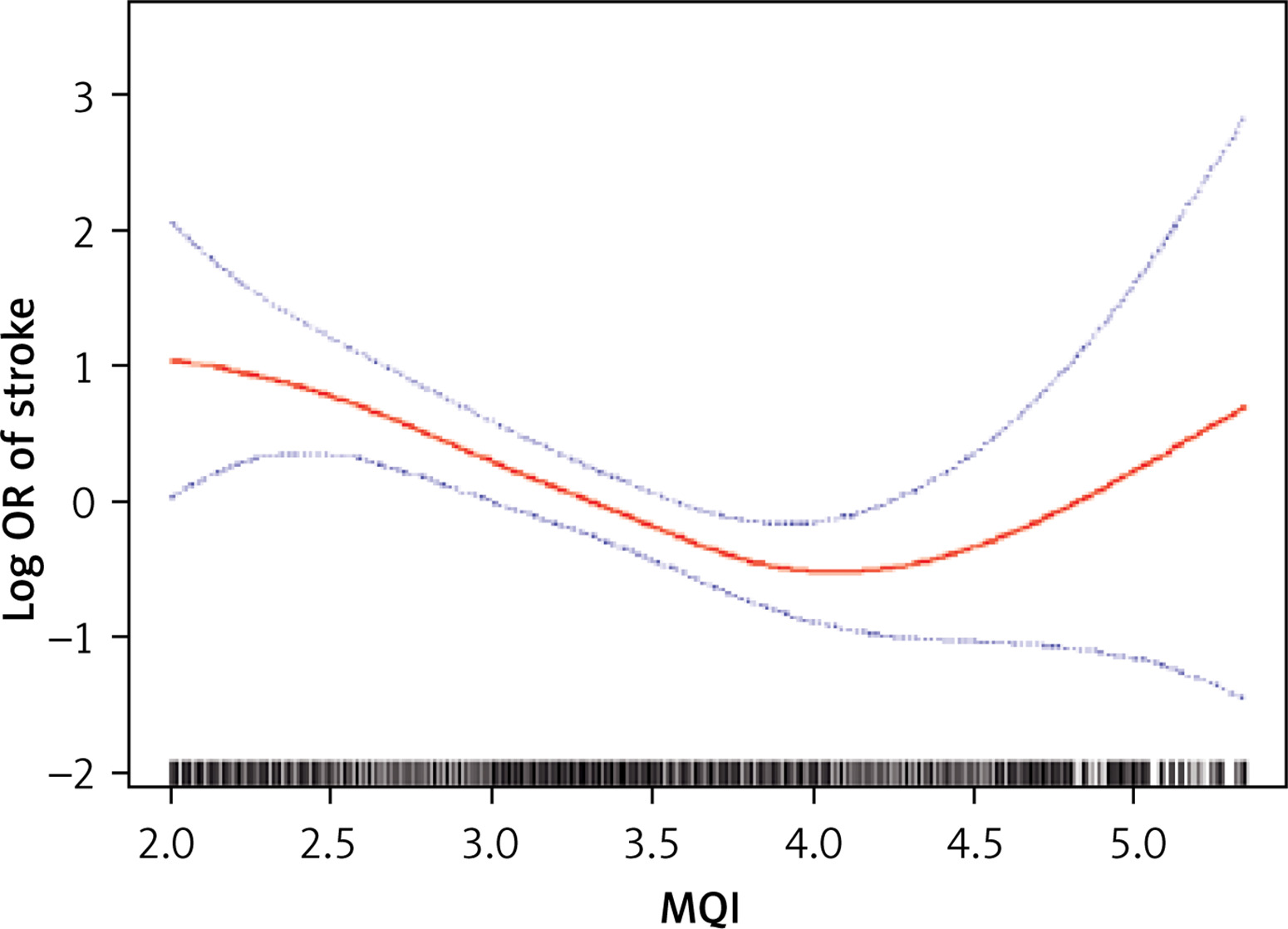
Table 2
Threshold effect analysis between muscle quality index and stroke. Age, sex, ethnicity, body mass index, poverty income ratio, marital status, education level, smoking status, alcohol consumption, hypertension, diabetes, hypercholesterolemia and physical activity were adjusted in the threshold effect analysis
Subgroup analyses
Subgroup analyses stratified by demographic, socioeconomic, and cardiovascular risk factors revealed no significant interactions (all p for interaction > 0.05; Supplementary Table SIII), indicating that the inverse association between MQI and stroke prevalence was consistent across all subgroups examined.
Discussion
In this nationally representative sample of U.S. adults aged 20–59 years, we observed a nonlinear, inverse association between the MQI and stroke prevalence. This association reversed beyond an inflection point (MQI = 4.34). And this pattern remained consistent across comprehensive subgroup analyses, and the lower odds of stroke in the normal MQI group were robust to both continuous and categorical specifications. However, this study uses a cross-sectional design, where the exposure (MQI measured in 2011–2014) and outcome (self-reported history of stroke) were ascertained concurrently. As stroke often leads to motor deficits, disuse atrophy, and metabolic changes that can directly reduce muscle mass and strength, any observed association between lower MQI and prevalent stroke may be driven by reverse causality. In this context, a low MQI could be a consequence of the stroke rather than a pre-existing risk factor. This critical limitation will be considered when interpreting the findings.
Although previous studies have established sarcopenia and low handgrip strength as independent risk factors for stroke [5, 8], evidence regarding the MQI – a composite measure of muscle efficiency – remains scarce. To our knowledge, only one prior investigation using NHANES 2011–2014 data examined MQI in relation to stroke and reported no significant independent association after multivariable adjustment [9]. A key distinction is that the prior study relied solely on linear logistic regression and did not assess potential nonlinearity or threshold effects. By applying generalized additive models and piecewise regression, we identified a significant nonlinear relationship with a distinct inflection point, which may account for the discrepant findings. Our results suggest that the association between MQI and stroke is not uniform across the entire distribution and that failing to account for nonlinearity may obscure true effects.
Skeletal muscle is not merely a contractile tissue but also a metabolically active endocrine organ that secretes myokines regulating inflammation, insulin sensitivity, and energy homeostasis [10]. The MQI, which integrates strength and mass, captures the qualitative aspect of muscle function that declines more rapidly than mass alone [11]. Several biological mechanisms may underlie the observed inverse association. First, reduced muscle mass and strength are linked to chronic low-grade systemic inflammation, characterized by elevated pro-inflammatory cytokines (e.g., TNF-α, IL-6) and diminished anti-inflammatory mediators (e.g., IL-10) [12]. This pro-inflammatory state promotes endothelial dysfunction and accelerates atherosclerotic plaque formation and destabilization [13]. Second, muscle dysfunction induces insulin resistance and compensatory hyperinsulinemia, which contribute to visceral adiposity, dyslipidemia, and metabolic syndrome – all established stroke risk factors [14]. Third, sarcopenia is associated with a higher incidence of heart failure, myocardial infarction, and atrial fibrillation, thereby increasing the risk of cardioembolic stroke [9, 15]. Fourth, physical inactivity may both precipitate and result from muscle deterioration, forming a vicious cycle that amplifies cardiovascular risk [16].
The positive association between MQI and stroke risk above the threshold should be interpreted with caution. This finding was based on a small number of participants with extremely high MQI, and the wide confidence interval (OR = 20.22, 95% CI: 1.92–212.60) indicates substantial imprecision. Although extremely high muscle quality may occasionally reflect supraphysiological conditions (e.g., androgen abuse or pathological hypertrophy) [17, 18], it more likely represents random variation or residual confounding. It is important to note that overinterpretation of this finding could be misleading, as it does not support the concept of a “threshold effect” in the sense of a harmful level of high muscle quality. Replication in larger, more diverse populations is warranted before drawing definitive conclusions.
Several limitations merit consideration. First and foremost, the cross-sectional design precludes any determination of temporality or causality. The observed association is likely confounded by reverse causality, as discussed. Second, despite adjustment for a wide range of confounders, residual confounding due to unmeasured variables cannot be excluded. Third, stroke history was self-reported and not verified by medical records, which may introduce misclassification bias. Fourth, DXA scans were available only for participants aged 20–59 years; thus, our findings may not be generalizable to older adults or nonU.S. populations. Fifth, MQI cutoffs were derived from a young adult reference population (20–39 years), whereas our sample included individuals up to 59 years. Although age- and sex-specific cutoffs were applied, some misclassification may persist. Finally, analyses were unweighted and therefore do not provide nationally representative estimates – a consequence of our analytic focus on internal validity rather than population inference.
In conclusion, this cross-sectional study demonstrates a nonlinear, inverse association between MQI and stroke prevalence in U.S. adults aged 20–59. However, due to the temporal ambiguity inherent in the study design, this association may just reflect post-stroke muscle deterioration rather than a protective effect of high pre-morbid muscle quality. The findings underscore the necessity for prospective cohort studies in the future to measure MQI prior to the onset of stroke, with the aim of establishing the temporal sequence and elucidating whether muscle quality is a modifiable risk factor for cerebrovascular disease. At this juncture, the study proposes a hypothesis that merits further investigation with more robust methodologies.