Cardiovascular disease (CVD) and cancer remain the two leading causes of morbidity and mortality worldwide. In 2022, an estimated 20 million new cancer cases and 9.7 million cancer-related deaths were reported globally [1]. Meanwhile, in 2023, there were 19.2 million CVD deaths worldwide (up from 13.1 million in 1990), and 626 million prevalent cases of CVD globally, more than double the 311 million prevalent cases reported in 1990 [2]. With continued improvements in cancer diagnosis and effective personalized treatment, a growing proportion of patients survive their malignancy in the long term, shifting the clinical focus from cancer-related mortality toward chronic comorbidity management [3]. As cancer-specific mortality declines, CVD has emerged as the leading non-cancer cause of death, accounting for up to 49% of non-cancer deaths among survivors of solid tumors [4].
The concept of survivorship has evolved from a singular focus on achieving cancer remission to a broader emphasis on preserving long-term quality of life during and after treatment [5]. This expanded perspective necessitates greater attention to cardiometabolic health, as cancer survivors exhibit a heightened risk of conditions such as hypertension, dyslipidemia, diabetes, obesity, and metabolic syndrome [3, 6]. This elevated risk reflects not only the direct effects of cancer itself, such as increased inflammation and oxidative stress, and exposure to oncologic therapies, but also the cumulative impact of pre-existing conditions and lifestyle disruptions that are often exacerbated during and after the cancer journey [5]. For this reason, the Polish Lipid Association (PoLA), in its 2026 lipid guidelines, considers cancer an important CVD risk modifier [7].
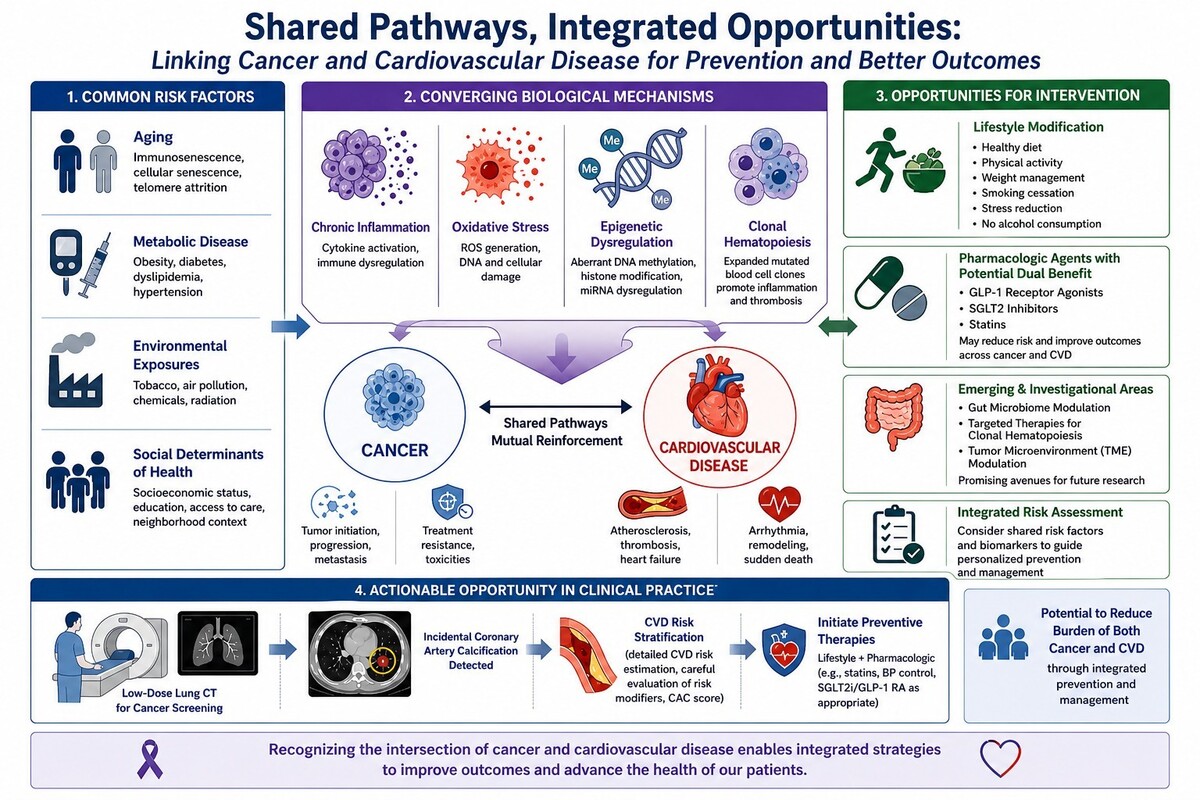
Increasing evidence supports a complex and bidirectional relationship between cancer and CVD, driven by shared modifiable risk factors, including aging, smoking, dyslipidemia, obesity, diabetes, hypertension, adverse lifestyle behaviors, and socioeconomic determinants, as well as overlapping biological pathways such as chronic inflammation, oxidative stress, and metabolic dysregulation [3, 6]. Despite these overlaps, global evidence characterizing the co-occurrence and temporal evolution of CVD and cancer burden across epidemiological transition stages remains limited, underscoring the need for integrated analyses to inform coordinated prevention strategies. This gap is further compounded by suboptimal CVD risk detection (e.g. lipid measurements are performed in only about 5% of cancer patients) and management in oncology practice, where preventive strategies and structured risk assessment are not consistently implemented, despite recommendations from the Heart Failure Association of the European Society of Cardiology and the International Cardio-Oncology Society [8]. This gap is particularly concerning given the expanding population of cancer survivors and the increasing long-term exposure to cardiovascular risk.
In this issue of Archives of Medical Science, Qiu et al. provide important global evidence on the co-occurrence of CVD and neoplasms using Global Burden of Disease (GBD) 2021 data [9]. The authors demonstrate marked spatial clustering of disease burden aligned with socioeconomic development stages, identifying four distinct regional patterns, low-burden, neoplasm-dominant, CVD-dominant, and dual-burden regions, with clear divergence in temporal trends across these groups. The geographic distribution of four patterns overlaps substantially with global economic development level. Low-burden regions achieved 3–4% annual reductions in CVD burden, whereas dual-burden regions experienced increasing trends, resulting in a 5.8% gap. Overall, nearly half of the CVD burden (49.7%) was attributable to high systolic blood pressure, with additional contributions from high LDL-C (20.2%), high body mass index (10.5%), and high fasting plasma glucose (10.0%). By comparison, smoking accounted for 18.5% of the neoplasm burden. These contributions varied markedly across regional patterns, with specific combinations of modifiable risk factors playing a key role in shaping global disparities in disease burden trajectories [9].
Socioeconomic conditions play a key role in CVD outcomes among patients with cancer, particularly across countries with different levels of economic development [10]. In low- and middle-income settings, limited financial resources, lower insurance coverage, and constrained healthcare infrastructure are associated with delayed diagnosis, reduced access to cancer and cardiovascular care, and poorer adherence to guideline-directed therapies. These factors contribute to higher financial burden, worse quality of life, and suboptimal management of e.g. of cardiotoxicity and heart failure in cancer survivors. In contrast, higher-income countries are more likely to provide structured surveillance and cardio-oncology services, leading to earlier detection and better management of CVD complications [10]. But even in high-income countries, where cardio-oncology departments have been established, the diagnosis and management of CVD risk factors and the detection and treatment of CVD and its complications remain far from optimal [11].
Hypertension is the leading cause of CVD significantly contributes to adverse cardiovascular outcomes, including myocardial infarction, stroke, and heart failure [3]. This risk is further amplified in patients with cancer, who often have a higher prevalence of hypertension than the general population, reflecting both shared risk factors and treatment-related effects [3]. In addition, hypertension has been associated with increased risks of cancer incidence and mortality [3].
Tobacco use is a well-established cause of cancer, accounting for a substantial proportion of cancer-related deaths and contributing to multiple site-specific malignancies in a dose-dependent manner [3]. It also markedly increases cardiovascular risk, raising the incidence of CVD by approximately 63% and more than doubling CVD-related mortality. Notably, even low levels of exposure and passive smoking are associated with significantly elevated risks of coronary artery disease and stroke [3].
Among patients with active or remitted cancer, the prevalence of dyslipidemia ranges from 28% to 58% [6]. In the general population, dyslipidemia is strongly associated with CVD and mortality, while in patients with cancer it has also been linked to increased tumor progression and higher cancer-related and all-cause mortality [6]. Low to extremely low HDL-C (< 30 mg/dl), like very high HDL-C (>100 mg/dl), are of large interest as potential markers of carcinogenesis, but this association remains to be confirmed [12].
These findings highlight that a “one-size-fits-all” prevention strategy is unlikely to be effective, as the burden of CVD and neoplasms clusters strongly by socioeconomic development. Regions facing a dual burden require integrated, system-level approaches (comprehensive integrated programs) that address both cardiometabolic and cancer risks simultaneously, rather than relying on traditionally siloed programs. A possible solution is joint preventive strategies and management using proven interventions that reduce all-cause and cause specific mortality through comprehensive programs dedicated to patients with cancer and CVD. The divergence in temporal trends, where low-burden regions achieve sustained reductions while dual-burden regions worsen, also signals widening global health inequities. Without targeted investment in prevention, early detection, and primary healthcare infrastructure, this gap is likely to expand further [13].
The observed variation in both combined and region-specific risk factor patterns suggests that prevention strategies should move beyond single-risk-factor models toward more integrated and context-specific frameworks. Accordingly, healthcare systems, particularly in low- and middle-income countries where primary care capacity is still developing, should prioritize integrated non-communicable disease management platforms rather than maintaining separate cardiovascular and oncology services. Such integration may improve efficiency, reduce fragmentation of care, and better address the clustering of risk factors underlying the co-occurrence of CVD and neoplasms.
While lifestyle modification remains central to prevention e.g. the highly effective role of regular physical exercise in reducing the risk of both cancer and CVD [14–16], pharmacologic strategies are increasingly being recognized for their potential dual benefits across CVD and neoplasms [5]. Agents such as glucagon-like peptide-1 (GLP-1) receptor agonists, sodium-glucose cotransporter-2 (SGLT2) inhibitors, and statins may confer cross-disease protective effects through improvements in metabolic, inflammatory, and endothelial pathways [3]. In particular, statins, widely used in cardiovascular prevention, have been proposed to have potential relevance in oncology due to their pleiotropic effects, although evidence for cancer-related outcomes remains evolving [17]. In addition, emerging areas of investigation, including gut microbiome modulation, targeting clonal hematopoiesis, and interventions influencing the tumor microenvironment, represent promising directions for integrated cardio-oncology prevention strategies [3].