Introduction
Multiple sclerosis (MS) is a chronic and progressive demyelinating disease of the brain and spinal cord that responds to immunosuppression [1]. Despite progress in the treatment of relapsing-remitting MS (RRMS) thanks to the approval of numerous therapies over the past decade, reducing disease relapses and disability progression remains a challenge for many patients.
Currently, B cell-depleting monoclonal antibodies that principally act through modulation of peripheral immune responses are proven as a highly effective strategy for the treatment of RRMS [2]. Immediate initiation of the treatment with highly effective drugs is currently the most effective way to treat patients with MS. However, we still encounter many MS patients who, when initially treated with drugs of lower efficacy, do not obtain satisfactory results in the long run.
Ofatumumab (OFA), an anti-CD-20 monoclonal antibody, was approved in 2020 in the European Union and has been shown to be highly effective in inhibiting disease activity and progression in randomized, controlled clinical trials [3]. It has been demonstrated that OFA is effective in treatment of RRMS, as it positively affects relapse rates, magnetic resonance imaging (MRI) measures of disease activity, and disability progression. Furthermore, it can reduce the risk of progression to clinically definite MS in patients with a first clinical demyelinating event.
In phase II studies (APLIOS, APOLITOS and MIRROR) subcutaneous OFA therapy in patients with RRMS was associated with a significant reduction in the number of new active (contrast-enhanced, Gd+) demyelinating lesions compared to baseline or placebo [4–6]. This was confirmed by the results of two multicenter, double-blind, randomized, active comparator-controlled (teriflunomide) phase III studies (ASCLEPIOS I (n = 927) and ASCLEPIOS II (n = 955), which enrolled patients aged 18–55 years, diagnosed with RRMS or secondary progressive MS (SPMS) [7]. Furthermore, long-term data from the open-label ALITHIOS study confirmed the durable efficacy of continuous OFA treatment for 5 and 6 years in patients with RRMS [8–10]. In the long-term analysis, there was a significant reduction in the frequency of relapses, a reduction in the number of new MRI lesions, and a high percentage of patients achieving no evidence of disease activity (NEDA-3). In patients who switched from teriflunomide to OFA, a marked reduction in relapses and resonance activity was observed after the change of treatment. A significant difference in annualized relapse rate (ARR) between teriflunomide and OFA was observed in the first 2 years of follow-up. After changing treatment to OFA, no statistically significant difference was noted in the group of patients previously taking teriflunomide. ARR remained low in the OFA group continuously from the initiation of the treatment. However, effectiveness of OFA in the real-world setting remains to be fully elucidated.
The aim of the present study was to assess the efficacy and safety of OFA treatment in patients with RRMS in real clinical practice in six Polish MS treatment centers. To the best of our knowledge, this is the first multi-center real world evidence (RWE) study in Poland. The hypothesis of the presented analysis, based on available clinical trials and RWE, was the high effectiveness of OFA in reducing the relapse activity of the disease and inhibiting its progression, especially in patients whose treatment was initiated immediately after the diagnosis of MS was established.
Material and methods
Study design
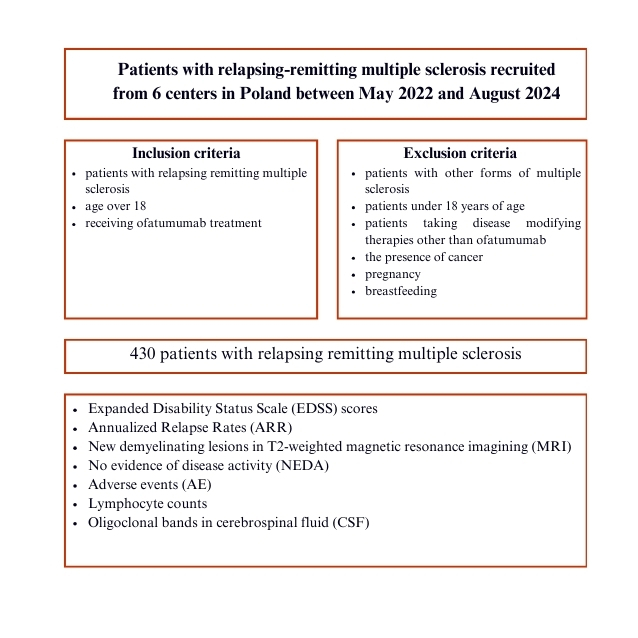
This retrospective observational study was conducted in six MS clinical centers in Poland, involving a cohort of patients with RRMS who started treatment with OFA between May 2022 and August 2024. The inclusion criteria were the following: patients with RRMS, age over 18, receiving OFA treatment. The exclusion criteria were: patients with other forms of MS, patients under 18 years of age, patients taking disease-modifying therapies (DMTs) other than OFA, the presence of cancer, pregnancy and breastfeeding. Epidemiologic data at baseline were applied to evaluate outcomes. All diagnoses were in accordance with the McDonald criteria (2017 update) [11]. The following data were collected: demographics, duration of the disease, number of previous MS therapies, the last DMT used before starting OFA treatment and the reason for switching; number of relapses within 12 months before OFA initiation and at 12 and 24 months after starting treatment; Expanded Disability Status Scale (EDSS) scores before OFA initiation and at 12 and 24 months; lymphocyte counts before OFA initiation and at 2, 6, 12, 14, 18, and 24 months; MRI assessments within 12 months before OFA initiation and at 12 and 24 months; adverse events (AE), discontinuation of OFA treatment, change to another DMT within 2 years of treatment.
Definitions
Active MRI lesions were defined as gadolinium enhanced (Gd+) lesions or new/enlarging T2 lesions. No evidence of disease activity (NEDA-3) was defined as no relapses, no disability progression, and no active MRI lesions. According to previous reports, changes in EDSS scores were classified as improvement or worsening as follows: for patients with a baseline EDSS of 0, a change of at least 1.5 points; for patients with a baseline EDSS of 0.5 to 4.5, a change of at least 1 point; and for patients with a baseline EDSS of ≥ 5, a change of at least 0.5 points. EDSS changes that did not meet the criteria for improvement or worsening were classified as stable EDSS [12].
The degrees of lymphopenia were defined as follows: grade I (< 1.0–0.8 × 109/l); grade II (< 0.8–0.5 × 109/l); grade III (< 0.5–0.2 × 109/l); and grade IV (< 0.2 × 109/l) [13]. The incidence of lymphopenia in patients whose lymphocyte counts were measured 2 months after the first treatment or later was evaluated, taking into account the lowest lymphocyte count recorded for each patient.
We considered naive patients as those who had not previously received any therapy, whereas previously treated patients were those who had used other DMTs prior to OFA.
Statistical analysis
The descriptive part of the statistical analysis included the numbers of each group and their structure indicators. As the variables analyzed were not normally distributed, the median and quartile range (IQR) values were provided in the descriptive analysis. The analysis of the significance of differences in the numbers of each subgroup was performed using Pearson’s χ2 test.
Multivariate logistic regression was used to evaluate potential correlations and the effects of independent variables on the parameters of interest, adjusted where necessary. The odds ratios (OR) and 95% confidence intervals (CI) were calculated respectively. A value of p < 0.05 was considered statistically significant. Statistical analysis was performed using Statistica 13.0 software (StatSoft, Krakow, Poland).
Results
Patients’ characteristics
The study recruited 430 patients with RRMS from 6 MS treatment centers in Poland. Among the patients, 66.5% were women; the mean age at diagnosis was 29.5 years. Until August of 2024, on average their disease lasted 6.90 (median: 5.28) years. Mean time between diagnosis and treatment initiation was 1.71 years; however, the median time was 0.25 years, between treatment start and OFA onset 3.90 years (median: 2.79), and between diagnosis and OFA treatment onset 5.61 years (median: 3.90). 27.44% of patients were treatment-naïve.
Most patients had been previously treated (72.56%), 63.02% received 1 or 2 DMTs; 9.54% received 3 or more DMTs. Most often, patients were treated with dimethyl fumarate (48.87%), IFN-1a/IFN-1b/GA (30.8%) and teriflunomide (12.54%). Treatment-naïve patients and those previously treated with other therapies were not compared with each other in this study. The reason for switching treatment for OFA was mostly the ineffectiveness of the previous therapy (36.13%) and side effects (29.19%). Among patients with data available (n = 234), 87.6% had type 2 oligoclonal bands in the cerebrospinal fluid (CSF).
Baseline characteristics of the group are presented in Table I.
Table I
Baseline characteristics of patients treated with OFA (n = 430)
Treatment efficacy
The results of the present study show a statistically significant decrease in the relapse activity of the disease during 1 year of OFA therapy. The percentage of patients free of relapses increased from 45% before treatment, to 88% after 1 year of follow-up (Figure 1). Moreover, the disability assessment index measured by mean EDSS remained stable after a year of follow-up and was 2. With regard to the reduction of radiological activity of the described treatment, the percentage of patients without new demyelinating lesions in T2-weighted MRI increased from 59.52% before the start of treatment to 89.77% after 6 months of treatment and 73.96% after a year of follow-up. The NEDA-3 index after the first year of treatment was obtained by 72.7% of patients, including 68% of women and 83% of men (Table II). Moreover, logistic regression analysis showed that men were 2.3 times more likely to achieve NEDA-3 (OR = 2.309, CL95 = [1.064; 5.012], p = 0.031).
Figure 1
Efficacy of ofatumumab therapy in reducing relapse activity of the disease. The percentage of patients free of relapses increased from 45% before treatment to 88% after 1 year of follow-up
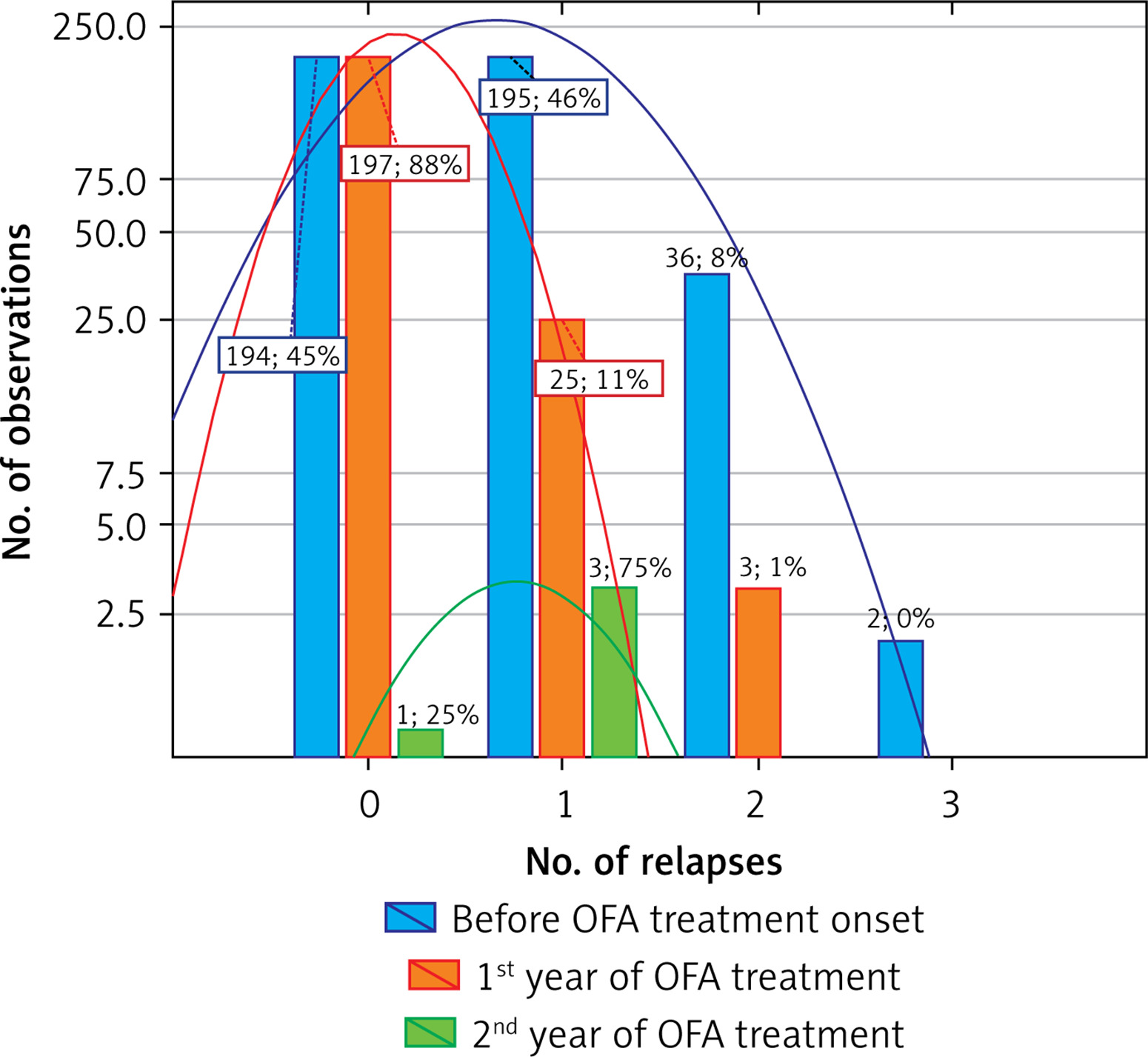
Table II
Percentage of patients who achieved NEDA-3 (no evidence of disease activity), defined as no relapses, no disability progression, and no active MRI lesions, by subgroup (women vs. men)
| Parameter | NEDA-3 | |
|---|---|---|
| n | % | |
| Total | 136 | 72.73 |
| Women | 87 | 67.97 |
| Men | 49 | 83.05 |
| P-value | 0.0314 | |
This was most likely related to the fact that in the population analyzed, men were included in OFA treatment sooner than women. Interestingly, a significantly longer period of time from MS diagnosis to treatment initiation was observed among women (mean: 100 weeks vs. 67.5 weeks in men) (p = 0.00514). This may suggest that a significant factor that has an influence on the chance of achieving NEDA-3 after the first year of OFA treatment is the duration of the disease – the earlier the DMT is initiated, the greater the chance of NEDA-3 being achieved by the patient (p = 0.005) (Figure 2). The analysis of the correlation of the period of time from diagnosis to the initiation of DMT treatment confirmed the hypothesis that a significant factor increasing the chance of obtaining NEDA-3 after the first year of OFA treatment is the duration of the disease – the greater the difference in the period between diagnosis and initiation of DMT treatment, the lower is the chance of obtaining NEDA-3. Similarly, a significant factor decreasing the chance of obtaining NEDA-3 after the first year of OFA treatment is the delay between diagnosis and initiation of OFA treatment. Although the influence of patient’s age and the length of the delay in OFA treatment proved to be statistically significant in logistic regression (p = 0.045 and p = 0.005, respectively), the size of the odds ratio in both cases does not allow the type of correlation to be determined (OR = 0.967 and OR = 0.999). It should be noted that in the regression analysis, age and delay were treated as continuous (numeric) variables. On the other hand, the analysis of the effect of delay as a variable coded into intervals showed that the shorter the delay period from diagnosis to the moment of initiation of OFA treatment was, the higher was the percentage of NEDA-3 obtained. The relationship was statistically significant (p = 0.005).
Figure 2
Assessment of the correlation of the length of the period between the diagnosis of multiple sclerosis (MS) and the implementation of disease-modifying treatment (DMT) with ofatumumab (OFA) with the percentage of patients achieving disease inactivity (no evidence of disease activity – NEDA-3) defined as no relapses, no disability progression, and no active MRI lesions
Safety profile of therapy
The study also confirmed the beneficial safety profile of OFA therapy. No new safety signals were detected. AE were reported in 56 (18.60%) patients during 2 years of the treatment, including flu-like symptoms and weakness (Table III). These symptoms were mild in most patients and occurred mostly after the first dose of OFA. These events did not require additional interventions and did not lead to discontinuation of the drug. All patients completed 2 years of treatment and did not start another treatment during the follow-up period.
Table III
Adverse events during follow-up period
| Adverse events (AE) | N | % |
|---|---|---|
| No AE | 245 | 81.40 |
| Influenza-like symptoms | 42 | 13.95 |
| Weakness | 14 | 4.65 |
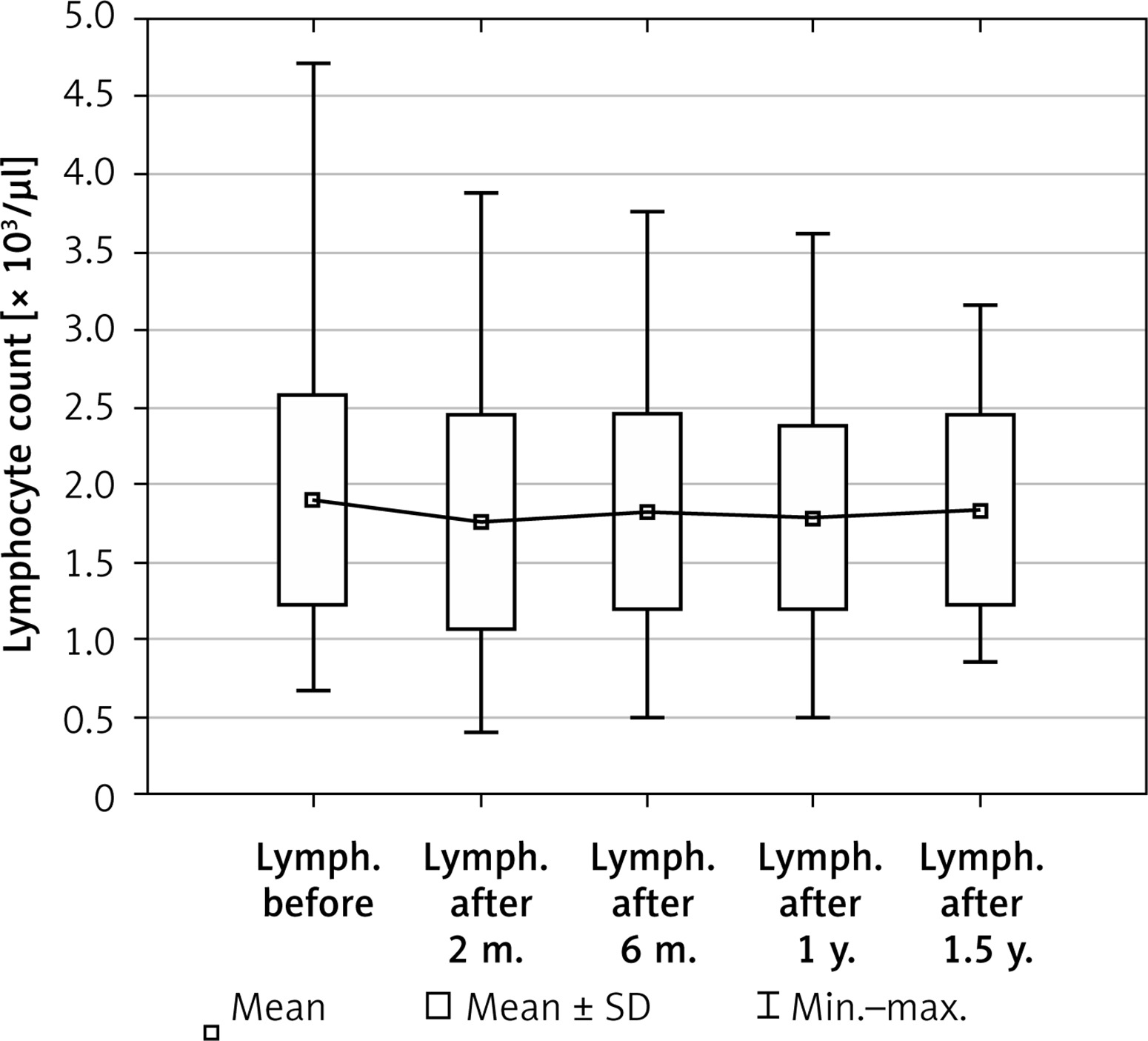
The lymphocyte count 2 months after the first dose (mean 1.76) was statistically significantly lower than before the start of therapy (mean: 1.90) (p < 0.0000) (Figure 3). However, after a 6-month follow-up period, it returned almost to the baseline (mean: 1.83) (p > 0.05). 86.67% of patients had normal lymphocyte counts across the study, 9.39% had grade 1 lymphopenia, 3.64% grade 2 lymphopenia, 0.30% grade 3 lymphopenia, and none grade 4 lymphopenia. Lymphopenia of grade 3 and higher was only observed until month 4. COVID-19 infection was noted in 29 out of 107 patients. 59 out of 109 patients were vaccinated.
Discussion
This was the first multicenter RWE study to assess the efficacy and safety of OFA in the Polish population, which made it innovative. The obtained results confirmed the high efficacy and safety of OFA therapy in a 1-year follow-up.
The results of the proposed analysis proved the effectiveness of OFA therapy in reducing relapsing and radiological disease activity. Our data further demonstrated a measurable benefit of initiating treatment with OFA with respect to confirmed disability progression, as after 1 year of the treatment, the patients remained stable in EDSS assessment.
It was also found that the best result of the treatment can be achieved in patients who start the therapy as soon as possible after the diagnosis of the disease has been established. Suboptimal effectiveness of OFA was noted in patients whose treatment was initiated with a delay after the diagnosis of MS was made. Therefore, early treatment with OFA is recommended for patients with active relapsing MS. These findings supported previous studies indicating the greatest effectiveness of immune B-cell-depleting therapies in naïve patients with RMS [9].
In relation to the safety profile, no new safety signals or side effects were detected during the follow-up period. The most common AE was flu-like symptoms that occurred after the first dose of treatment and did not require any intervention. This was consistent with previous analyses, mainly from clinical trials, and confirmed the high safety profile of OFA therapy.
Similarly to our results, the ASCLEPIOS I and ASCLEPIOS II studies showed that OFA therapy, compared to the one based on teriflunomide, was associated with a significantly lower ARR [7]. In addition, a reduced risk of confirmed disability worsening (CDW) was observed at 3 and 6 months. Furthermore, OFA therapy was more effective in reducing new demyelinating lesions on MRI – there was an almost complete reduction of active demyelinating lesions. A similar effect of OFA compared to teriflunomide was observed in all analyzed subgroups (age, gender, body weight, disease activity, previous DMTs).
Additionally, a post hoc analysis of the ASCLEPIOS study assessed the effectiveness of OFA in a subgroup of treatment-naïve patients diagnosed with RRMS within the last 3 years [14]. Compared with patients receiving teriflunomide, OFA reduced ARR by 50.3% (0.09 vs. 0.18; p < 0.001), the number of Gd+ lesions by 95.4% (0.02 vs. 0.39: p < 0.001), and the number of new/enlarging T2 lesions/year by 82.0% (0.86 vs. 4.78, p < 0.001).
The latest data from the open-label ALITHIOS study showed sustained efficacy of OFA treatment for up to 6 years in recently diagnosed patients – defined as those initiating treatment within 3 years of initial diagnosis – and previously untreated patients [9, 10]. In patients whose OFA therapy was initiated from the beginning of diagnosis, a 44% reduction in ARR was achieved, and a 96.4% and 82.7% reduction in MRI changes (Gd+ and T2), respectively. Similarly, a 24.5% and 21.6% reduction in CDW at 3 and 6 months, respectively was noted, compared with patients who replaced teriflunomide therapy with OFA. The ARR in treatment-naïve RRMS patients was reduced from 0.104 to 0.050 (52.0% reduction), corresponding to an adjusted ARR of one relapse per 20 years. The 3- and 6-month rates of progression independent of relapse activity (PIRA) in previously untreated patients were also lower compared to patients who had changed their treatment. A rapid increase in the percentage of patients achieving NEDA-3 was also observed, which was maintained during the 6 years of follow-up. This is in accordance with our results, which indicated that the earlier OFA treatment was initiated after diagnosis, the higher was the chance of achieving NEDA-3.
RWE analyses are also consistent with the results from our study. Two non-interventional studies are ongoing in Germany to assess the efficacy, safety and tolerability of OFA – AIOLOS (a study with previously untreated patients) and KAIROS (a study with patients previously taking other DMTs) [15, 16]. In the AIOLOS analysis, 384 patients – 78.6% receiving OFA, 21.4% receiving interferon β/glatiramer acetate (IFNβ/GA) – were enrolled by 75 centers. Relapses in the IFNβ/GA cohort tended to be more severe, and more often required hospitalization or corticosteroid treatment. In addition, more patients in the IFNβ/GA cohort than in the OFA cohort experienced serious adverse events and AEs, leading to study discontinuation.
Moreover, a retrospective secondary study of MSBase registry data conducted in Australia by Van der Walt et al., which included both naïve and transition/previous therapy patients, showed that the relapse-free rate in the OFA group at 1 year was 94.7% and 92.9% at 2 years [17]. Furthermore, in a Swedish registry of 111 MS patients treated with OFA, a decrease in ARR from 0.690 to 0.019 during a 1-year follow-up was observed [18]. In addition, patients remained stable on the EDSS scale. Similar reductions in relapse activity and disability inhibition were confirmed in the study by Chisari et al., which recruited patients with RRMS who were treated with OFA from seven Italian MS centers [19]. In contrast to the other studies, no significant differences were found between the previously treated and switched groups. Furthermore, no serious AEs were reported, the most common being fever on first administration (80.3%), as in our analysis.
The study by Harding et al. demonstrated that in a real-world setting, long-term outcomes are more favorable with early intensive therapy compared with first-line moderately effective DMTs [20]. It is consistent with the He et al. study, which showed that highly effective therapy initiated within 2 years of disease onset is associated with less disability after 6–10 years than that initiated later in the course of the disease [21].
Our study had several limitations. First, due to the nature of the study (RWE) and the relatively recent approval of OFA for the treatment of RRMS in Europe (2020), the follow-up period was only 1 year. Therefore, our study can be considered a pilot study, especially since data are still being collected in all centers, and further results will be presented in subsequent publications. In addition, it is currently a retrospective study, but as mentioned above, due to the continuous updating of data, we will be able to evaluate patients prospectively. Moreover, the vast majority of the analyzed patients had been previously treated with another DMT (over 72%), which could have influenced the assessment of the efficacy of OFA. Additionally, naïve patients and patients previously treated with other therapies are not currently compared with each other, but it is planned for the next stages of the analysis. Nevertheless, in our opinion, the proposed study constitutes a significant contribution to the evaluation of the effectiveness and safety of OFA treatment analyzed in the Polish population. Already at this stage, the presented RWE analysis has provided reliable results on the assessed therapy, which are consistent with previous clinical studies and RWE from other countries. Moreover, the perspective of further data collection creates the possibility for even more detailed, prospective and long-term observation of patients using OFA treatment.
In conclusion, the results of the present study confirmed the high effectiveness of OFA therapy in reducing the relapsing activity of the disease, as well as in inhibiting the progression of disability, with a favorable safety profile. They also indicated the necessity to start treatment as soon as possible after diagnosis in order to achieve the best possible inhibition of the disease activity and progression. Early access to highly effective treatment methods, such as OFA, may help reduce the burden of disease and the risk of RRMS progression and contribute to long-term improvement of quality of life. Moreover, the present study is one of the few multicenter RWE studies that are currently available in the literature. The analysis seemed to be limited by the short observation period. Therefore, there is a need to continue obtaining data for long-term assessment of the efficacy and safety of OFA therapy in real medical practice.