Introduction
Autism spectrum disorder (ASD) is a complex neurodevelopmental condition characterized by diverse symptoms, including social interaction challenges, atypical sensory responses, and unique behavioral patterns [1, 2]. Advances in research have improved understanding of ASD onset, early signs, and comorbidities, contributing to rising global prevalence rates [3]. Enhanced awareness and better diagnostic tools have increased accuracy, particularly in children, and led many adults to seek assessments for ASD traits [4].
ASD affects individuals and their whole family systems universally, regardless of socio-demographic factors, making it a significant social concern. Prevalence rates are higher in countries with advanced healthcare systems due to improved screening and standardized diagnostic practices [5–7]. However, comorbid conditions such as ADHD, anxiety, and intellectual disabilities complicate diagnosis as overlapping symptoms can obscure ASD traits. Approximately 70% of individuals with ASD have additional psychiatric conditions, with anxiety disorders often exacerbating symptoms and delaying intervention [8, 9].
Early diagnosis is crucial for improving quality of life. Interventions initiated before the age of three, such as Applied Behavior Analysis (ABA) and the Early Start Denver Model (ESDM), have demonstrated long-term benefits, including enhanced cognitive and social skills and reduced need for special education [10–13].
Healthcare professionals, particularly primary care physicians and pediatricians, are vital in identifying undiagnosed ASD, especially in cases with masking comorbidities. Standardized diagnostic tools like ADOS-2 and ADI-R and professional training are essential for improving diagnostic accuracy [14]. In Poland, studies have highlighted knowledge gaps among physicians, underscoring the need for targeted educational initiatives to enhance support for individuals with ASD and their families [15, 16].
This article aims to assess physicians’ knowledge of ASD, focusing on symptoms, comorbidities, and diagnostic challenges. It also identifies areas where further education is needed to improve patient care quality.
Material and methods
Study design
The study was conducted online between May and June 2024 using the LimeSurvey platform in the Center of Postgraduate Medical Education (CMKP) in Warsaw, Poland. A personalized link to the survey was distributed via email to 1029 physicians enrolled in mandatory specialization courses offered by CMKP. These courses, delivered by a public institution responsible for the majority of postgraduate medical training in Poland. Participation in the study was voluntary, and the survey was presented as an optional component of the training. A total of 395 physicians completed the questionnaire, yielding a response rate of 38.4%.
To ensure anonymity and data confidentiality, no identifying information was collected. Participants were informed about the anonymous nature of the survey and the intended use of the data for research purposes as detailed in the informed consent statement displayed at the beginning of the questionnaire. The distribution process involved sending a unique survey link to each participant via email. To enhance response rates, reminder emails were issued; however, the anonymity of the participants was preserved throughout the process. Data were collected and aggregated automatically by the LimeSurvey system, ensuring both data integrity and confidentiality.
The research tool was a standardized questionnaire, i.e. Knowledge about childhood autism among health workers (KCAHW) [17]. The KCAHW questionnaire comprises 19 item questions, each offering three response options, with only one correct answer. A correct answer to each question is awarded a score of one, while each of the two incorrect answers receives a score of zero. The total score of KCAHW is the number of correct answers to 19 questions and it ranges from 0 to 19. The higher the total score, the better the respondent’s knowledge about ASD. The KCAHW questionnaire is divided into four domains:
Domain 1. This domain comprised eight item questions focusing on the social interaction impairments typically observed in children with childhood autism. Scores in this domain can range from a minimum of 0 to a maximum of 8.
Domain 2. This domain included one item question that assessed impairments in communication and language development, which are part of the symptom presentation in children with childhood autism. The possible scores in this domain range from 0 to 1.
Domain 3. This domain consisted of four item questions that addressed obsessive and compulsive behavioral patterns in children with childhood autism. These behaviors are characterized as restricted, repetitive, and stereotyped. Scores in this domain can range from a minimum of 0 to a maximum of 4.
Domain 4. This domain included six item questions that provided information about the nature of childhood autism, potential comorbid conditions, and the onset of the disorder in affected children. The scoring in this domain ranges from a minimum of 0 to a maximum of 6.
The higher the score in a particular domain, the better the respondent’s knowledge about ASD in this domain.
We also used an author’s own questionnaire on autism – a questionnaire consisting of 10 questions regarding knowledge about the autism spectrum, including 8 closed, 1 semi-open and 1 open-ended question. Additionally, the doctors were asked about professional and sociodemographic data such as professional experience (as a doctor), specialization, place of work, year of birth/age, gender, marital status, and place of residence.
Statistical analysis
The statistical analyses were conducted using Statistica software.
Minimum and maximum values as well as mean (M) and standard deviation (SD) were estimated for numerical variables, while absolute numbers (n) and percentages (%) of the occurrence of category for categorical variables.
Two-sample unpaired Student t test was used to compare numerical scores of KCAHW between women and men, between the respondents who had contact with a person on the autism spectrum and those who did not, between the respondents who had a person on the autism spectrum in their own family or environment and those who did not.
Analysis of variance (ANOVA) F test was used to compare numerical scores of KCAHW between age groups, professional experience, places of residence, and between the respondents who thought that autism spectrum disorders occurred very often, those who thought they occurred often and those who thought they occurred rarely in the society.
Due to a large sample size, the central limit theorem was used to analyze numerical scores of KCAHW. This theorem states that sampling distribution of the sample means can be approximated using a normal probability distribution when sample size is large. The significance level was assumed at 0.05. All the figures were generated using MS Excel.
Results
Study group characteristics
The study involved 395 physicians aged 25–69 years (mean age: 31 ±6.3 years), with 63% aged 25–29. The group was predominantly female (75%), and most participants were either married or in a relationship (55.7%). The majority lived in urban areas (45%), had up to 5 years of professional experience (79%), were in the process of specialization/specialty (86%), and worked in hospitals (84%) (Table I).
Table I
Demographic and professional characteristics of the study group (N = 395)
Perceptions of ASD
Most respondents (75%) reported contact with individuals on the autism spectrum, with 28% having contact within their own family or close circle (Table II). Around half believed ASD is a frequent social condition, while 37% considered it rare. Nearly all respondents (96%) agreed that ASD’s causes are largely unknown, though 50% cited/mentioned genetic factors, while smaller proportions attributed it to parent-child bond disturbances/disruption (15.7%), maternal alcohol use (14%), GMO foods (1.5%), and vaccines (1%).
Table II
Answers to questions regarding autism spectrum disorders, in the study group (N = 395)
ASD was recognized as a socially relevant issue by 93% of participants, but only 23.5% saw tangible impacts from government/government impacts or institutional efforts. Critical areas for improvement included education (20%) and access to diagnostic and therapeutic services (7%). The internet (85%) and social media (60%) were the most common sources of ASD information, followed by TV/radio (24%) and print media (18%). Most respondents (72%) believed public awareness of ASD had increased in recent years.
Knowledge of autism (KCAHW) results
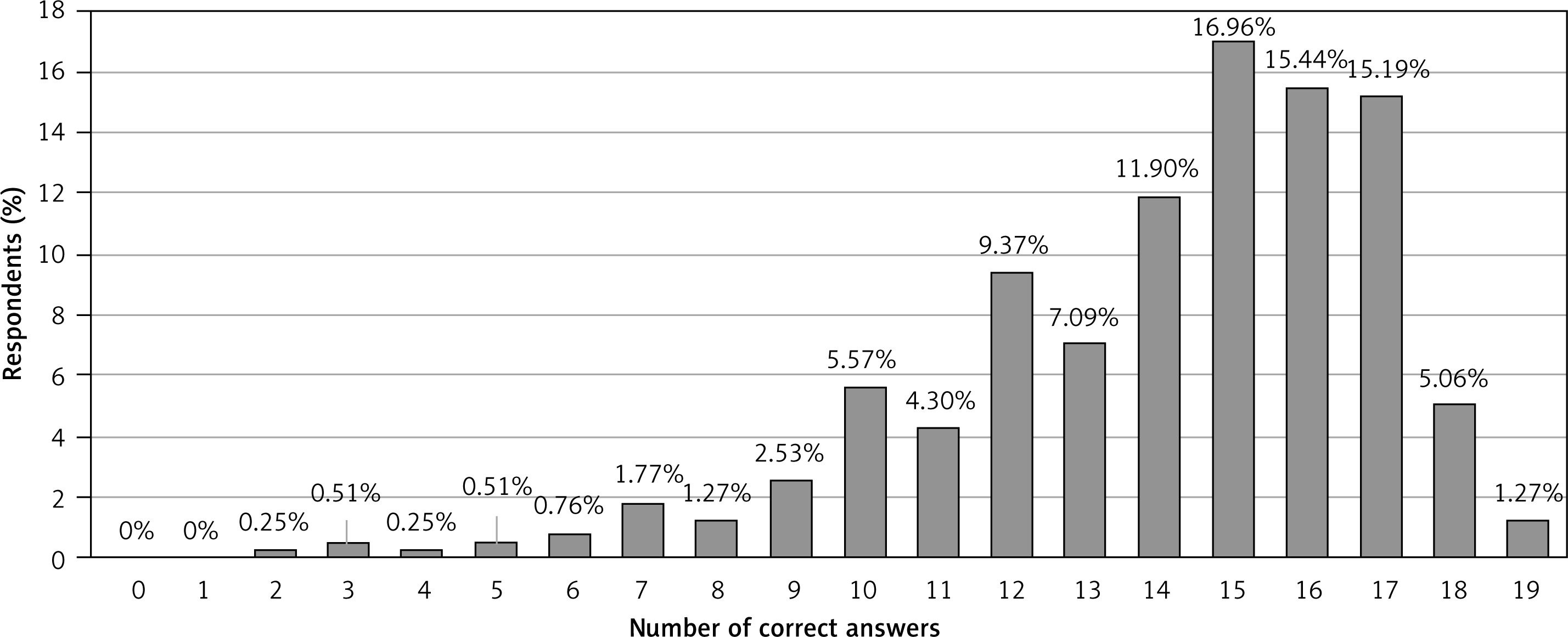
Physicians answered 74% of KCAHW questions correctly on average (mean score: 14.1 ±3.0), with only 1.3% achieving perfect scores (Table III). The most correctly answered questions concerned non-verbal behavior impairments, peer relationship failures/problems, and the perception of children with ASD as “deaf or dumb” (over 90% correct). In contrast, questions on intellectual impairment (18% correct) and childhood onset of ASD (29% correct) had the lowest accuracy.
Table III
Knowledge about autism according to KCAHW, in the study group (N = 395)
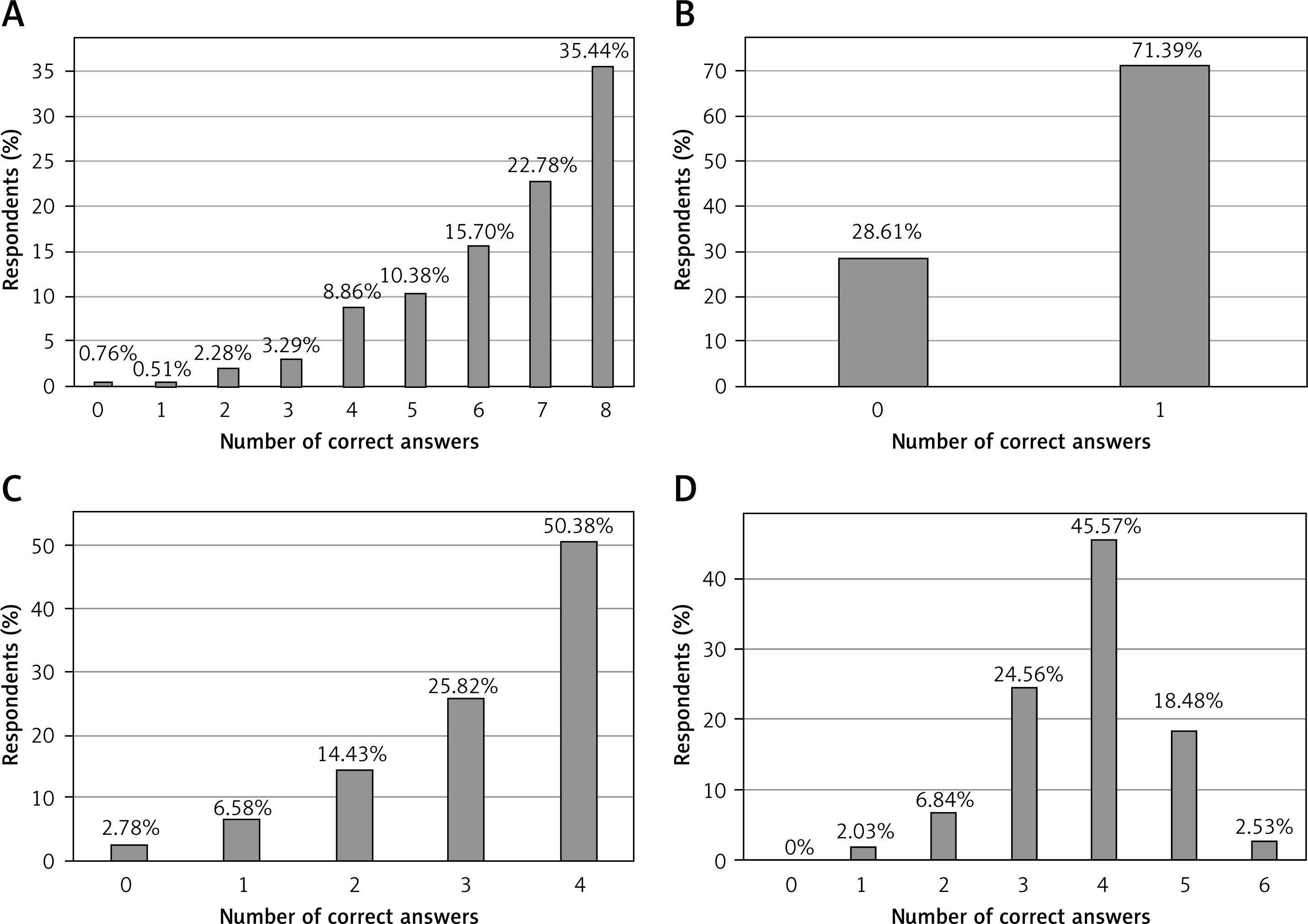
Performance across the four KCAHW domains varied:
– social interaction impairments: participants averaged 6.4 ±1.7 out of/in 8 questions (80% accuracy).
– communication impairments: the single question in this domain was correctly answered by 71%.
– repetitive behaviors: respondents averaged 3.1 ±1.1 out of/in 4 questions (78.5% accuracy).
– types of disorder and comorbidities: the weakest domain, with an average score of 3.8 ±1.0 out of/in 6 questions (63% accuracy). Only 10% of respondents answered all questions correctly (Figures 1, 2).
Correlations between knowledge and demographic features/characteristics
Female physicians scored higher than males across all domains and in total KCAHW scores (p < 0.05). Younger participants showed significantly better overall knowledge (p = 0.024), particularly in the “Types of Disorder and Comorbidities” domain (p = 0.05) (Table IV).
Table IV
Correlations of KCAHW with demographic and professional characteristics of the study group as well as with some questions regarding autism spectrum disorders, in the study group (N = 395)
Physicians with up to 5 years of professional experience also outperformed more experienced colleagues, especially in understanding comorbidities and onset (p = 0.006). Place of residence showed no significant impact on knowledge (p > 0.05).
Personal or familial contact with individuals on the autism spectrum was associated with higher total KCAHW scores and better performance in three domains: social interaction impairments, communication and language development, and repetitive behavior patterns (p < 0.05). Additionally, respondents who viewed autism as a frequent social condition scored higher in communication-related knowledge than those who considered it rare (p = 0.044).
Discussion
This study evaluated ASD knowledge among Polish physicians using the Knowledge about childhood autism among health workers (KCAHW) questionnaire, providing a comprehensive analysis and enabling comparisons with international research [17, 18]. Physicians demonstrated a solid understanding of core ASD concepts, with an average score of 74%, aligning with global findings [19]. However, varying knowledge levels across domains revealed gaps that may hinder patient care, highlighting the urgent need for targeted educational interventions [20, 21].
Direct contact with individuals on the autism spectrum correlated with higher knowledge scores, reflecting the benefits of experiential learning. This finding supports integrating hands-on components into ASD training programs to foster empathy and practical understanding, ultimately improving diagnostic accuracy and communication with patients [19, 22].
Significant knowledge gaps were noted in understanding ASD onset and intellectual impairment, with only 29% accuracy in these areas. Misconceptions here could lead to delayed diagnoses and missed early interventions, emphasizing the need for more rigorous education on ASD comorbidities and development [23, 24].
Socio-demographic factors influenced knowledge levels. Female physicians scored higher, particularly in behavioral and social interaction domains, possibly reflecting their specialization in pediatrics and psychiatry, where ASD knowledge is more relevant. Younger physicians demonstrated greater awareness of ASD comorbidities, likely due to updated curricula. However, the need for continuous education remains critical for those who did not receive formal ASD training during their education [25].
A concerning finding was the high reliance on internet and social media as primary information sources. This trend raises the risk of misinformation, especially in a complex condition like ASD, where nuanced understanding is essential. Educational efforts should include critical appraisal skills to help healthcare providers navigate digital sources effectively and apply evidence-based practices [26, 27].
The study highlights the importance of combining theoretical knowledge with experiential learning to address knowledge gaps and improve empathy and diagnostic skills. Cross-disciplinary training and evidence-based digital education resources could further enhance healthcare providers’ knowledge on ASD, supporting a more holistic approach to diagnosis and management.
Strengths of the study include its large, diverse sample and use of the validated KCAHW tool, enabling reliable international comparisons. Demographic analysis provided valuable insights for developing targeted educational initiatives. However, limitations include potential biases due to the digital format, reliance on self-reported data, and the focus on theoretical knowledge, leaving practical clinical understanding unmeasured. These factors should be addressed in future research to optimize ASD education and support for healthcare providers.
In conclusion, this study highlights the urgent need for continuous, targeted ASD education to address specific knowledge gaps across demographic and professional groups. However, the findings should be interpreted with caution due to the small sample size and the potential lack of representativeness of the broader population. These limitations underscore the need for further research using larger, more diverse samples. Future studies should also examine the impact of experiential and digital learning modules on improving practical ASD knowledge and diagnostic skills, aiming to enhance care quality as ASD prevalence rises. Ensuring informed, evidence-based, and compassionate ASD care remains essential for healthcare systems striving to meet the needs of individuals with ASD effectively.