Introduction
Systemic lupus erythematosus (SLE) is a chronic multisystem autoimmune disease and affects several organs, including the liver [1]. It is clinically frequent with abnormal liver function tests, and the prevalence of developing liver enzyme abnormalities is about 25–60% among patients with SLE [2–4]. The causes of liver enzyme abnormalities are numerous, such as drug toxicity, viral infections, alcohol abuse, and fatty infiltration, but either disease activity or drugs can be the main etiology among SLE patients [4–6]. With improvement of therapy, 10-year survival rates of patients with SLE have been more than 80%; moreover, patients with chronic liver injury are more prone to undergo the process from fibrosis to cirrhosis, liver failure, and even hepatocellular carcinoma (HCC) [7–10]. Moreover, malignancies, especially liver cancer, have become the leading causes of death among Western patients with SLE [11–13]. Thus, understanding the role of liver function in prognosis of SLE patients is important in developing an adaptive treatment strategy.
Few SLE patients have liver biopsy and imagological examination for liver function examination in routine clinical practice, meaning they are not suitable for screening of clinically significant liver function for patients with SLE [14]. Fortunately, several scoring systems methods based on simple clinical parameters and blood tests for assessing liver fibrosis have been developed, whereas the Fibrosis-4 (FIB-4) index is the better predictor [15, 16]. The FIB-4 index is developed from age, alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels, and the platelet (PLT) count, which has been applied in predicting overall and specific mortality of patients in several cohort studies [17–20]. Moreover, the FIB-4 index is much simpler than the disease activity index (SLEDAI) score, which is currently used by rheumatologists to evaluate the outcomes of patients with SLE [21]. However, so far no studies have explored the association between the FIB-4 index and mortality of patients with SLE. Therefore, we analyzed data collected from the Jiangsu SLE Cohort (JSC) Study, a large multicenter retrospective cohort study in China [22, 23]. Our study aimed to explore the potential prognostic role of the FIB-4 index for patients with SLE. In addition, we compared it with the SLEDAI score for prognosis in SLE.
Material and methods
Study design and participants
The detailed study design of the JSC Study has been described previously [22, 23]. To summarize, the JSC Study is a large-scale, multicenter retrospective cohort study in China. Since 2010, under the organization of the Jiangsu Rheumatology Association, the Lupus Collaborative Group has built up the cohort of patients with SLE from hospitals in Jiangsu province, China.
All patients were hospitalized during 1999–2009 in Jiangsu province and those with missing or incomplete medical records were excluded. Eligible patients were those who met at least 4 classification criteria of SLE revised and updated by the American College of Rheumatology [24, 25]. A follow-up for survival status of patients with SLE was conducted among those who had medical records for the first time/admission. Up to 2015, we reviewed and enrolled 2451 valid medical records and twice carried out the follow-up, in 2010 and 2015. In total, we observed 226 deaths, comprising 166 deaths in 2010 and 60 deaths in 2015. We further excluded 120 patients because their FIB-4 index cannot be calculated due to AST, ALT and/or PLT being missing.
This study was performed in 2015 and was exempt from ethics approval requirements, since ethical review of research involving medical records or biospecimens was firstly required in 2016 according to national legislation from the National Health and Family Planning Commission of China [26].
Data collection and definition
We built a website (http://sys.91sqs.net/sle/Index/index.html) to collect and manage data from medical records of patients with SLE from different hospitals. We also extracted data from all medical records of first admission, including demographic characteristics (gender, age), diagnosed information, disease activity and damage, organ involvements, laboratory tests, and treatments.
The SLEDAI score was calculated to assess disease activity and was categorized into four grades, including almost no activity (SLEDAI = 0–4), mild activity (SLEDAI = 5–9), moderate activity (SLEDAI = 10–14), and high activity (SLEDAI ≥ 15) [21]. The FIB-4 index was calculated according to the following formula: (age [years] × AST [IU/l])/(PLT [× 109/l] × ALT [IU/l]1/2) [27]. We combined all diseases other than SLE as comorbidities. Accumulated organ damage in SLE was evaluated by the Systemic Lupus International Collaborating Clinics (SLICC)/American College of Rheumatology (ACR) Damage Index (SDI) [28]. The following values were considered normal: hemoglobin ≥ 110 g/l for female or ≥ 120 g/l for male; white blood cells 4–10 × 109/l, PLT 100–300 × 109/l, ALT < 40 IU/l, AST < 40 IU/l, serum albumin ≥ 35 g/l, 24 h-urinary proteins < 500 mg, blood urea nitrogen 2.86–7.14 mmol/l, serum creatinine ≤ 133 µmol/l, anti-dsDNA negative, antinuclear antibody negative, anti-Sm negative, C3 ≥ 0.8 g/l, C4 ≥ 0.2 g/l.
Statistical analysis
Statistical analyses were performed using Statistical Analysis Software (SAS) version 9.3 (SAS Institute, Inc., Cary, North Carolina, USA) and the program R (Version 3.5.3, R core team). Continuous variables were expressed as the median (quartile) and compared using the Mann-Whitney U test, or as mean and standard deviation (SD) compared using the t test. Categorical variables were expressed as the number (percentage), and descriptive analyses on the basis of the χ2 test were carried out for the distribution differences between deaths and censored survivals.
Kaplan-Meier survival analysis and log-rank tests were used for the initial survival analysis. Time in years was calculated from the diagnosis date of the patient to the date of death for deaths and to the date of the last follow-up for censored survivors. For survival analysis, two approaches were employed to explore the influence of the FIB-4 index on the risk of mortality of SLE. Firstly, we used Cox proportional-hazards regression models regression to estimate crude and adjusted hazard ratio (HR) and 95% confidence interval (95% CI). The FIB-4 index was classified into two categories according to the optimal Youden index-based cut-off point value by receiver operating characteristic (ROC) curve. The cut-off value for the FIB-4 index was 1.92, which was within the two cut-off values for three-way classification of the FIB-4 index among patients with human immunodeficiency virus/hepatitis C virus (HIV/HCV) coinfection (1.45 and 3.25) and nonalcoholic fatty liver disease (NAFLD) (1.30 and 2.67) [16, 27]. In cause-specific mortality analyses, subjects who did not die from the cause of interest were censored at the date of death. Secondly, an restricted cubic spline (RCS) model was used to estimate the adjusted dose-response relationship between FIB-4 index and mortality of SLE patients. Furthermore, we performed ROC curve analysis for estimating and comparing time-dependent areas under curves (AUCs) between FIB-4 index and SLEDAI score [29].
The following factors were included in the models as potential confounders: gender (male – 1, female – 0), SLEDAI score at admission (continuous), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0), immunosuppressive treatment on admission (yes – 1, no – 0). We also performed stratified analysis across clinical factors of patients with SLE patients.
Results
Characteristics of study subjects
Table I shows demographic and clinical characteristics of patients with SLE among deaths and censored survivals. Of all 2331 participants, 92.5% (2156) were female and the median (quartiles) age was 32.02 (23.61, 40.61). The median (quartiles) SLEDAI score at admission was 16.0 (11.0, 22.0) for deaths and 13.0 (9.0, 19.0) for censored survivals (p < 0.001). Deaths and censored survivals also differed in serum hemoglobin, PLT, AST, FIB-4 index, serum albumin, and 24 h urinary proteins, except age, body mass index (BMI) and white blood cells. For the distribution, no statistically significant differences were observed between deaths and censored survivals in gender, overall comorbidities, glucocorticoid drugs used before admission and on admission, mucocutaneous and musculoskeletal organ involvement, or positive autoantibodies of anti-dsDNA and antinuclear antibody, except immunosuppressive drugs used before admission (p = 0.001) and on admission (p < 0.001), neuropsychiatric (p < 0.001) and cardiopulmonary (p < 0.001) organ involvement, and anti-Sm positive autoantibodies (p = 0.006).
Table I
Characteristics of hospitalized patients with systemic lupus erythematosus (SLE) from Jiangsu cohort study
Hazard ratios for mortality
The hazard ratios of mortality of patients with SLE for SLEDAI score and liver function are shown in Table II. High SLEDAI score at admission was confirmed as a strong risk factor for mortality of SLE patients with adjusted HR and CI of 2.55 (95% CI: 1.68–3.00) for a SLEDAI score of 15 or more. After adjusting for confounding factors, positive associations were found between mortality of SLE and hepatitis, and abnormal serum albumin, with adjusted HR of 2.27 (95% CI: 1.23–4.21) and 2.20 (95% CI: 1.57–3.09), respectively. Drugs used before admission was not associated with mortality of SLE (adjusted HR = 1.29, 95% CI: 0.96–1.74). Compared with the group with normal values, abnormal groups of PLT, ALT and AST, and high FIB-4 (≥ 1.92) were positively associated with mortality of SLE, with adjusted HR of 1.58 (95% CI: 1.19–2.11), 1.54 (95% CI: 1.14–2.07), 1.58 (95% CI: 1.17–2.12), and 1.88 (95% CI: 1.42–2.12), respectively. Better survival was observed for those who had low FIB-4, compare with those who had high FIB-4, and log-rank p value was less than 0.001 (Figure 1). After adjusting for potential factors, a positive association between FIB-4 index and mortality of patients with SLE was observed consistently across all strata, except for male, normal hemoglobin, abnormal PLT, normal serum albumin, and antinuclear antibody negative (Figure 2).
Table II
Hazard ratios for survival of patients with systemic lupus erythematosus (SLE) according to SLEDAI score and liver function
| Variables | All N = 2331 n (%) | Death N = 226 n (%) | HR (95% CI) | Adjusted HR (95% CI)a |
|---|---|---|---|---|
| SLEDAI score at admission: | ||||
| 0–14 | 1273 (54.6) | 90 (39.8) | 1.00 | 1.00 |
| ≥ 15 | 1058 (45.4) | 136 (60.2) | 2.15 (1.61–2.86) | 2.25 (1.68–3.00) |
| Hepatitis: | ||||
| No | 2273 (97.5) | 215 (95.1) | 1.00 | 1.00 |
| Yes | 58 (2.5) | 11 (4.9) | 2.48 (1.35–4.55) | 2.27 (1.23–4.21) |
| Drugs used before admission: | ||||
| No | 1728 (74.1) | 147 (65.0) | 1.00 | 1.00 |
| Yes | 603 (25.9) | 79 (35.0) | 1.26 (0.94–1.69) | 1.29 (0.96–1.74) |
| Serum albumin [g/l]: | ||||
| ≥ 35 | 993 (42.6) | 57 (25.2) | 1.00 | 1.00 |
| < 35 | 1294 (55.5) | 169 (74.8) | 2.60 (1.87–3.61) | 2.20 (1.57–3.09) |
| PLT [109/l]: | ||||
| 100–300 | 1612 (69.2) | 125 (55.3) | 1.00 | 1.00 |
| < 100 or > 300 | 719 (30.8) | 101 (44.7) | 1.84 (1.39–2.43) | 1.58 (1.19–2.11) |
| ALT [IU/l]: | ||||
| < 40 | 1757 (75.4) | 151 (66.8) | 1.00 | 1.00 |
| ≥ 40 | 574 (24.6) | 75 (33.2) | 1.54 (1.14–2.07) | 1.54 (1.14–2.07) |
| AST [IU/l]: | ||||
| < 40 | 1729 (74.2) | 148 (65.5) | 1.00 | 1.00 |
| ≥ 40 | 602 (25.8) | 78 (34.5) | 1.69 (1.26–2.26) | 1.58 (1.17–2.12) |
| FIB-4 index: | ||||
| < 1.92 | 1531 (65.7) | 109 (48.2) | 1.00 | 1.00 |
| ≥ 1.92 | 800 (34.3) | 117 (51.8) | 2.11 (1.60–2.79) | 1.88 (1.42–2.50) |
a aAdjusted for sex (male – 1, female – 0), age (continuous, except for variables of FIB-4 index), SLEDAI score at admission (continuous, except for variables of SLEDAI score at admission), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0), immunosuppressive treatment on admission (yes – 1, no – 0). SLEDAI – SLE Disease Activity Index, PLT – platelet, ALT – alanine aminotransferase, AST – aspartate aminotransferase, FIB-4 – fibrosis-4.
Figure 1
Kaplan-Meier analysis and log-rank P-values (< 0.001) for FIB-4 index in patients with systemic lupus erythematosus (SLE)
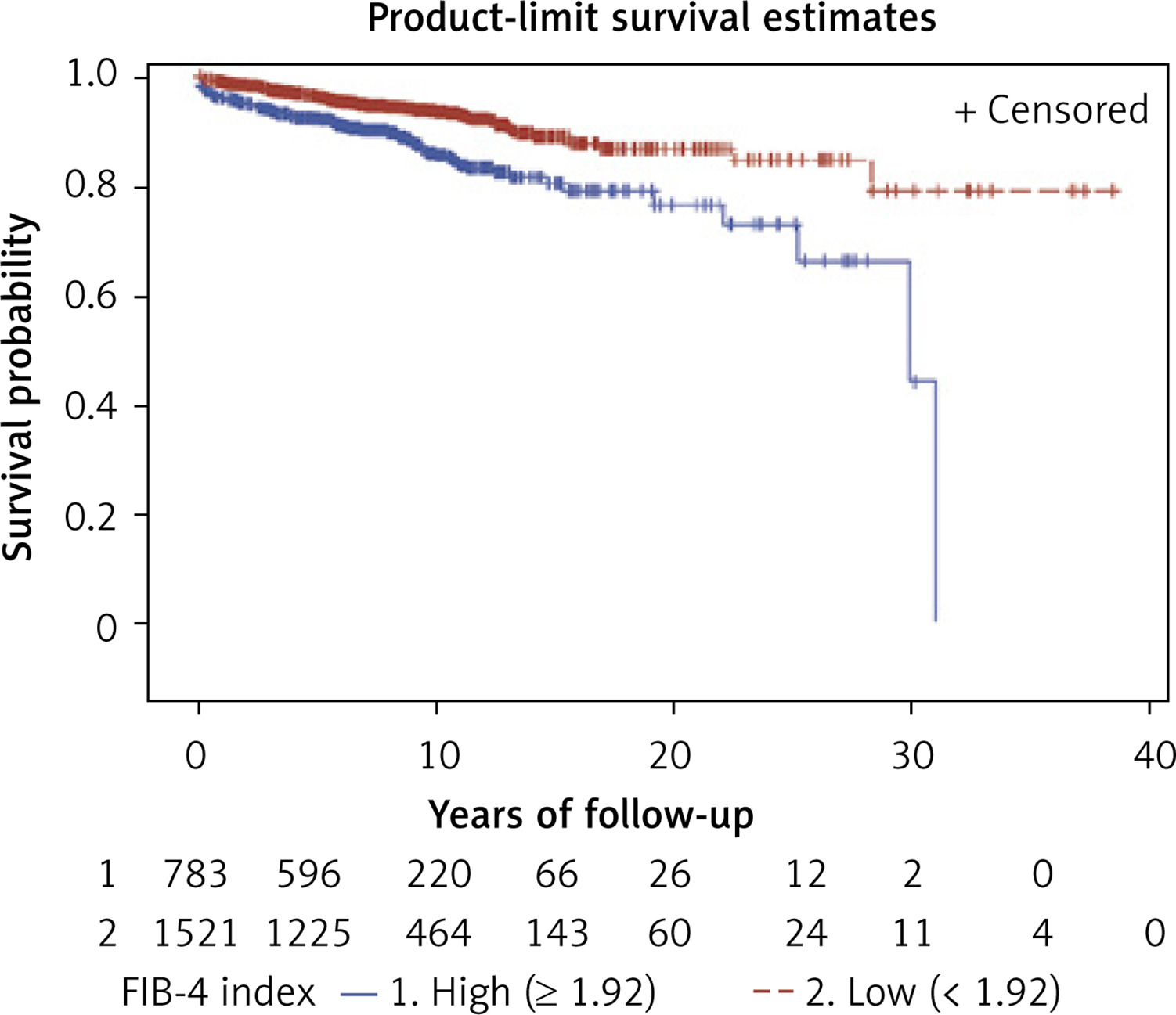
Figure 2
Hazard ratios for survival according to FIB-4 index stratified by clinical factors of systemic lupus erythematosus (SLE) patients. Models were adjusted for gender (male – 1, female – 0), SLEDAI score at admission (continuous), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0) and immunosuppressive treatment on admission (yes – 1, no – 0), and the above adjusted variables would be excluded when it was the stratified variable
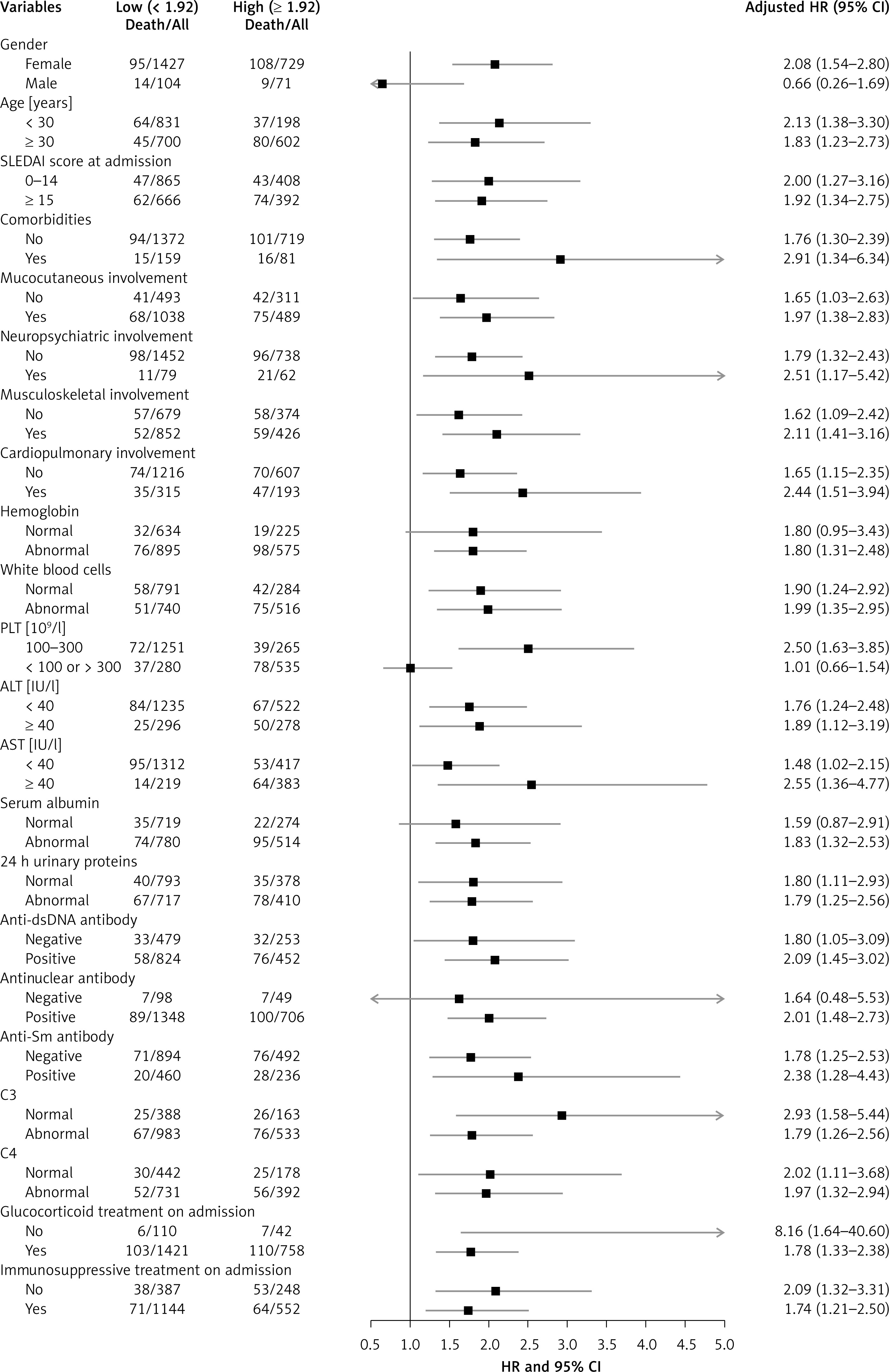
aAdjusted for sex (male – 1, female – 0), age (continuous, except for variables of FIB-4 index), SLEDAI score at admission (continuous, except for variables of SLEDAI score at admission), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0), immunosuppressive treatment on admission (yes – 1, no – 0). SLEDAI – SLE Disease Activity Index, PLT – platelet, ALT – alanine aminotransferase, AST – aspartate aminotransferase, FIB-4 – fibrosis-4.
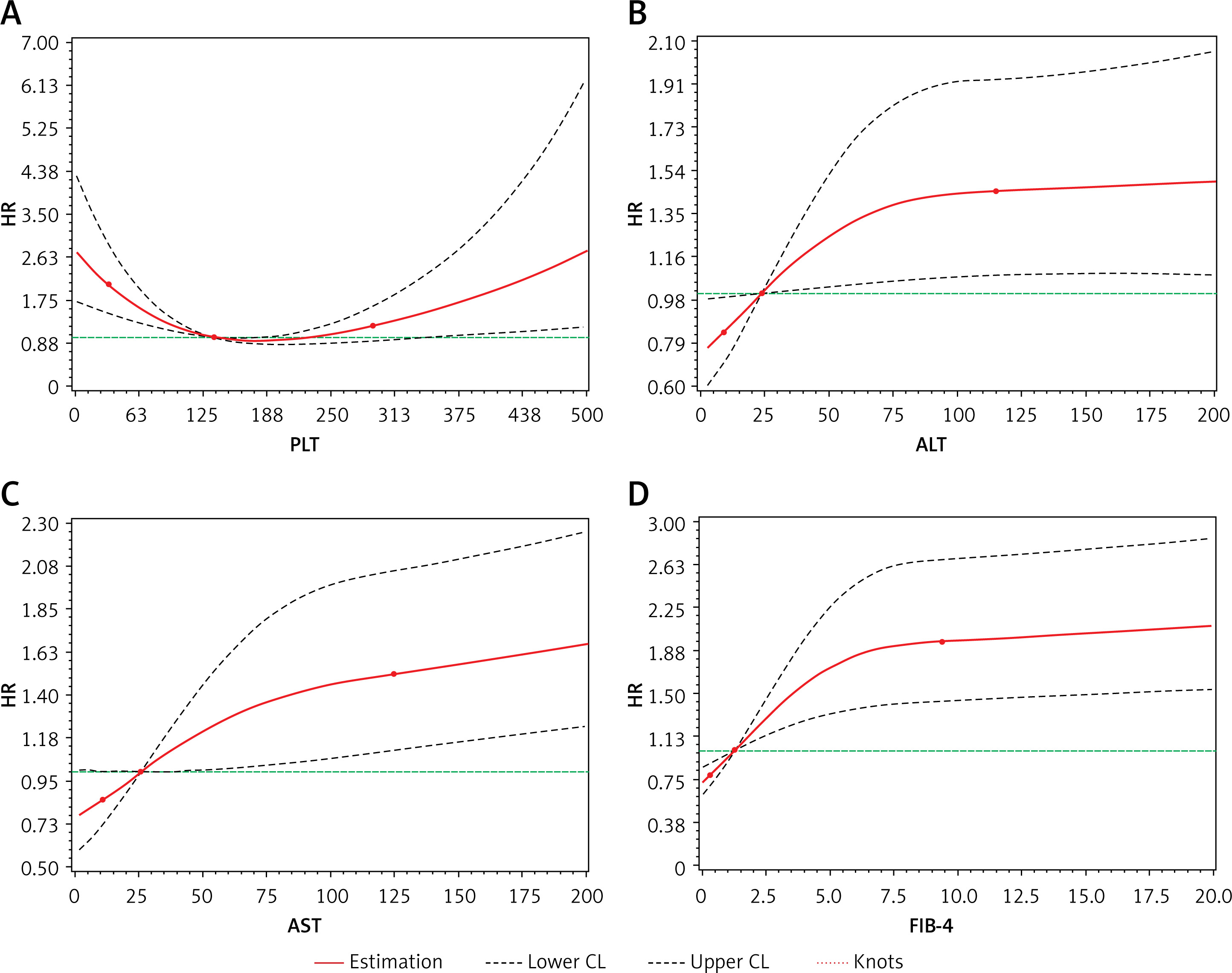
Dose-response relationships
In the RCS model, significant dose-response relationships (p values for overall association) were found between increased mortality of SLE patients and elevated level of PLT (p < 0.001), ALT (p = 0.043), AST (p < 0.001) and FIB-4 index (p < 0.001). Also it was nonlinear (p values for nonlinear association) for ALT (p = 0.046), PLT (p < 0.001) and FIB-4 (p < 0.001), but not AST (p = 0.109) (Figure 3).
Figure 3
Dose-response association between FIB-4 index and mortality of systemic lupus erythematosus (SLE) patients. RCS plots were adjusted dose-response association between mortality of SLE patients and (A) PLT, (B) ALT, (C) AST, and (D) FIB-4 index. Each liver function index was coded using RCS function with three knots, located at the 5th, 50th, and 95th percentiles (represented by dots). Y-axis represents the adjusted HR for SLE death for individuals with any value compared to individuals with median. Dashed lines are 95% CI. The P-values for overall association and nonlinear association were both < 0.001 for PLT, 0.043 and 0.046 for ALT, < 0.001 and 0.109 for AST, and both < 0.001 for FIB-4 index
Factors associated with high FIB-4 index
The risk factors associated with high FIB-4 index were gender, age, SLEDAI score at admission, 24 h urinary proteins, neuropsychiatric and cardiopulmonary organ involvement, and abnormal complement of C3 and C4 (Table III).
Table III
Logistic regression analysis for high FIB-4 index
Cause-specific mortality
Among 226 deaths in this cohort, the main causes of death were infection (n = 64, 28.3%), cardiopulmonary involvement (n = 38, 16.8%), neuropsychiatric impairment (n = 37, 16.4%), and renal failure (n = 33, 14.6%). A group of other causes of death (n = 54, 23.9%) includes hematologic involvement, macrophage activation syndrome, tumor, suicide and unknown (recorded as cardiopulmonary failure or multiple organ failure).
In particular, 7 patients died of gastrointestinal complications, including liver failure (n = 4), gastrointestinal bleeding (n = 2), and pancreatitis (n = 1).
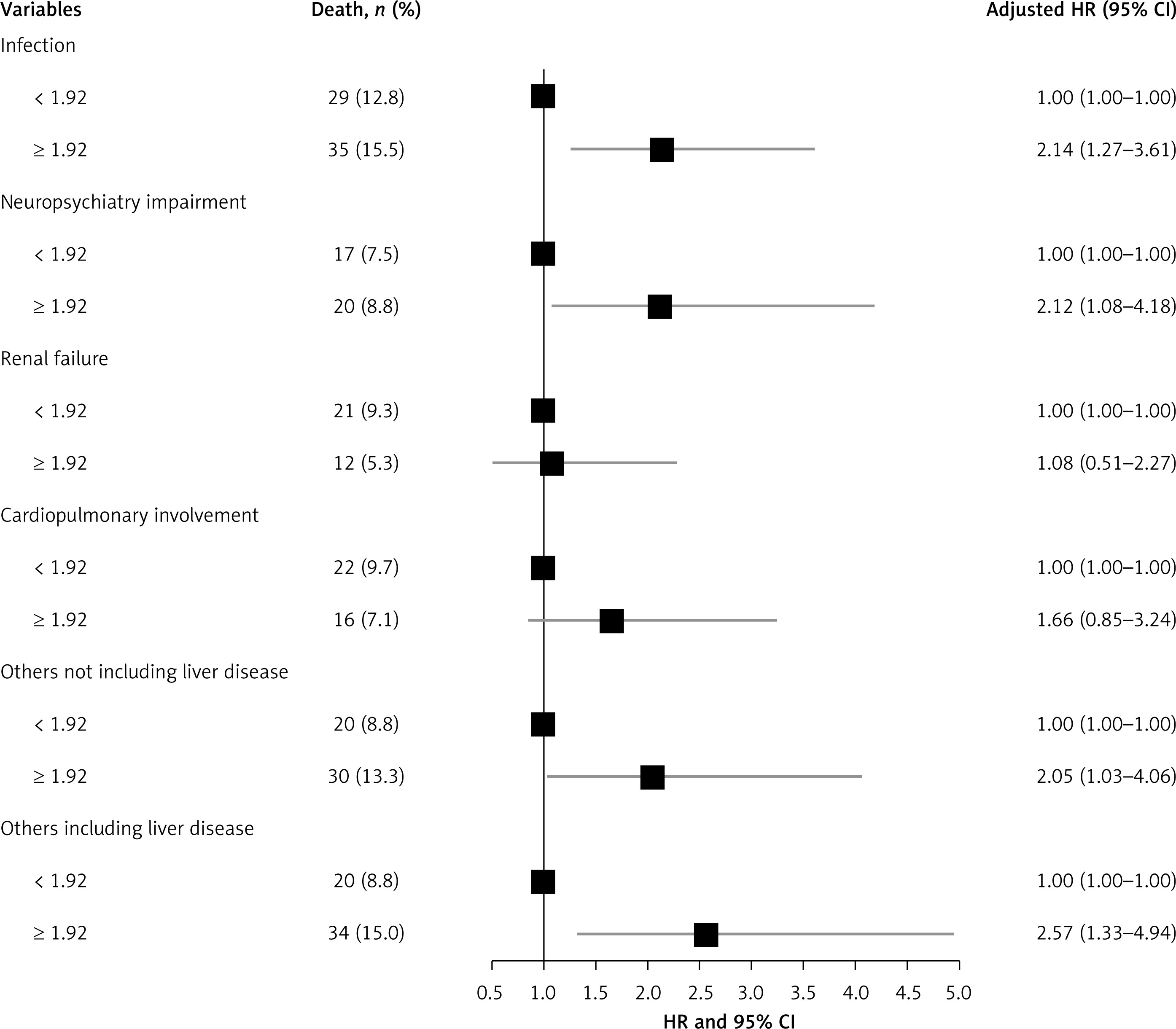
Figure 4 shows the association between FIB-4 index and mortality from each specific cause among patients with SLE. High FIB-4 index (≥ 1.92) was significantly associated with increased mortality from infection and neuropsychiatric impairment, with adjusted HR of 2.14 (95% CI: 1.27–3.61) and 2.12 (95% CI: 1.08–4.18), respectively. Elevated mortality from renal failure (adjusted HR = 1.08, 95% CI: 0.51–2.27) and cardiopulmonary involvement (adjusted HR = 1.66, 95% CI: 0.85–3.24) were observed in subjects with a high FIB-4 index compared to those with a low FIB-4 index, but it was not statistically significant. For subjects with a high FIB-4 index, adjusted HR of 2.05 (95% CI: 1.03–4.06) for risk of mortality from other causes increased to 2.57 (95% CI: 1.33–4.94) when specific mortality from liver diseases was included in the analysis.
Figure 4
Association between FIB-4 index and cause-specific mortality among patients with systemic lupus erythematosus (SLE). Models were adjusted for gender (male – 1, female – 0), SLEDAI score at admission (continuous), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0) and immunosuppressive treatment on admission (yes – 1, no – 0)
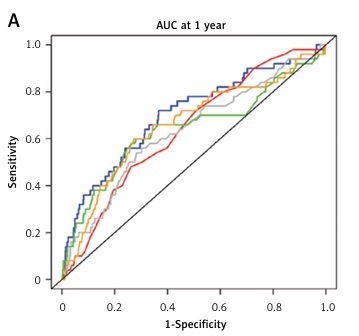
Comparison of performance of FIB-4 index and SLEDAI score
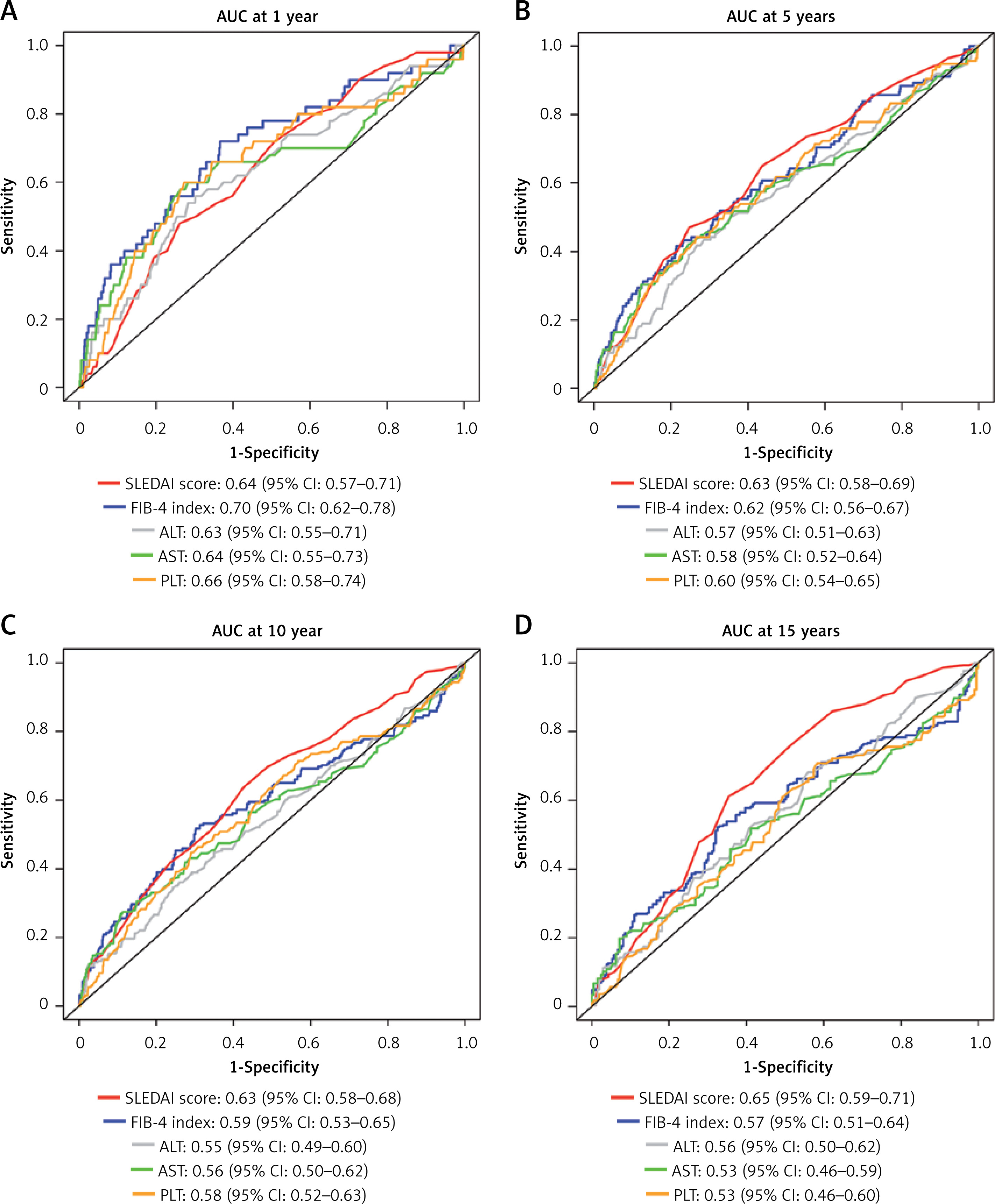
The joint effects of FIB-4 index and SLEDAI score at admission on hazard ratios for survival of patients with SLE are described in Table IV. No significant difference was observed between SLEDAI score and PLT (p = 0.339), ALT (p = 0.846), AST (p = 0.785) or FIB-4 index (p = 0.996) for the association with mortality of SLE patients. Moreover, Figure 5 demonstrates ROC curve analysis for estimating and comparing time-dependent AUCs between FIB-4 index and SLEDAI score at (A) 1, (B) 5, (C) 10 and (D) 15 years. We found no significant difference of AUCs between FIB-4 index and SLEDAI score, with p values for the comparison of AUCs at 1, 5, 10 and 15 years between FIB-4 index and SLEDAI score of 0.263, 0.654, 0.250, and 0.074, respectively.
Table IV
Joint effects of FIB-4 index and SLEDAI score at admission on hazard ratios for survival of patients with systemic lupus erythematosus (SLE)
| Variables | SLEDAI score | Death/All | OR (95% CI) | aOR (95% CI)a |
|---|---|---|---|---|
| PLT [109/l] | ||||
| 100–300 | 0–14 | 53/871 | 1.00 | 1.00 |
| < 100 or > 300 | 0–14 | 37/402 | 1.51 (0.96–2.39) | 1.54 (0.97–2.43) |
| 100–300 | ≥ 15 | 58/645 | 1.71 (1.14–2.54) | 1.88 (1.25–2.81) |
| < 100 or > 300 | ≥ 15 | 78/413 | 3.75 (2.58–5.45) | 3.83 (2.63–5.58) |
| Interaction: p = 0.339 | ||||
| ALT [IU/l] | ||||
| < 40 | 0–14 | 60/967 | 1.00 | 1.00 |
| ≥ 40 | 0–14 | 30/306 | 1.59 (0.98–2.56) | 1.60 (0.99–2.59) |
| < 40 | ≥ 15 | 91/790 | 2.18 (1.54–3.09) | 2.34 (1.65–3.34) |
| ≥ 40 | ≥ 15 | 45/268 | 3.32 (2.18–5.04) | 3.52 (2.31–5.36) |
| Interaction: p = 0.846 | ||||
| AST [IU/l] | ||||
| < 40 | 0–14 | 65/981 | 1.00 | 1.00 |
| ≥ 40 | 0–14 | 25/292 | 1.48 (0.90–2.44) | 1.51 (0.92–2.49) |
| < 40 | ≥ 15 | 83/748 | 2.01 (1.42–2.86) | 2.18 (1.53–3.10) |
| ≥ 40 | ≥ 15 | 53/310 | 3.36 (2.27–4.98) | 3.59 (2.41–5.33) |
| Interaction: p = 0.785 | ||||
| FIB-4 index | ||||
| < 1.92 | 0–14 | 47/865 | 1.00 | 1.00 |
| ≥ 1.92 | 0–14 | 43/408 | 1.95 (1.24–3.07) | 1.96 (1.25–3.09) |
| < 1.92 | ≥ 15 | 62/666 | 2.01 (1.35–3.00) | 2.16 (1.44–3.23) |
| ≥ 1.92 | ≥ 15 | 74/392 | 4.21 (2.84–6.23) | 4.24 (2.86–6.31) |
| Interaction: p = 0.996 | ||||
a Adjusted for sex (male – 1, female – 0), age (continuous, except for variables of FIB-4 index), comorbidities (yes – 1, no – 0), glucocorticoid treatment on admission (yes – 1, no – 0), immunosuppressive treatment on admission (yes – 1, no – 0). PLT – platelet, ALT – alanine aminotransferase, AST – aspartate aminotransferase, FIB-4 – fibrosis-4.
Discussion
In this large-scale multicenter retrospective cohort study, we found that higher FIB-4 index was positively associated with increased overall mortality of SLE with a nonlinear dose-response relationship. Moreover, ROC curve analysis indicated no significant differences of AUCs between FIB-4 index and SLEDAI score.
Up to now, there are no studies focusing on the association between the FIB-4 index and mortality of patients with SLE. This can be easily understood as few prospective studies have enough statistical power to predict mortality of liver-related diseases by using liver function indexes [17, 30, 31]. Consistent with our results that high FIB-4 index (≥ 1.92 vs. < 1.92) was associated with increased overall mortality of SLE patients with adjusted HR of 1.88 (95% CI: 1.42–2.50), accumulated evidence has shown that the FIB-4 index may be used as a prognostic marker [17–20, 30, 31]. Recently, in the United States, in a population-based prospective study, with up to 23 years of follow-up of 14,841 viral hepatitis-negative adult participants, researchers observed that a high FIB-4 index of more than 2.67 was associated with increased overall mortality with age adjusted HR of 1.38 (95% CI: 1.21–1.58) [18]. Moreover, for the cause-specific mortality risk, mortality from cardiovascular disease was only higher with a high FIB-4 index (HR = 1.32, 95% CI: 1.05–1.66), while mortality from liver disease was higher with an intermediate (HR = 3.49, 95% CI: 1.52–8.03) or high (HR = 42.45, 95% CI: 14.93–120.72) FIB-4 index in multivariate-adjusted analyses, but mortality from neoplasms and diabetes were elevated with neither intermediate nor high FIB-4 indexes [18]. In a previous study using the same cohort with 18 years of follow-up, FIB-4 index was also found to be independently associated with increased overall mortality, primarily from cardiovascular disease but not from liver disease [19]. In another recent cohort study of 2075 patients with chronic hepatitis B virus (HBV) infection, a high FIB-4 index (≥ 1.29 vs. < 1.29) was found associated with increased risks of adverse liver events including liver-related mortality (HR = 4.24, 95% CI: 2.19–8.23) and cirrhosis development during a mean follow-up period of 15.47 years [20]. Moreover, two retrospective studies demonstrated that FIB-4 index predicted overall mortality and liver events, but both concern not very large cohorts with long-term follow-up to study disease-specific mortality [30, 31]. One is a retrospective, international, multicenter cohort study, with a median of 8.7 years follow-up of 320 patients diagnosed with NAFLD, and the other is a retrospective Canadian cohort study with a median of 5 years of 148 patients who had liver biopsies and hepatic venous pressure gradient measurement. In this study with up to 15 years follow-up, we observed that 4 subjects died from liver diseases and all had a high FIB-4 index, so long-term observation would be needed in the future.
There is probably another reason why we cannot observe enough liver-related deaths, because competition risk exists in causes of death. Infections and organ involvement (mainly neuropsychiatric, renal and cardiopulmonary) affected by SLE are among the major causes of deaths among patients with SLE in Asian countries, which might produce the effects of competing risks on deaths of liver-related diseases [32]. Thus, in this study we observed that high FIB-4 index was mainly associated with the increased risk of specific mortality from infections, neuropsychiatric involvement, cardiopulmonary involvement and renal failure, though the latter two were not significant because of the limitation of small sample size.
The harm of liver-related diseases has been shown and affects other organs’ function among SLE patients, which makes it possible to understand how increased FIB-4 index is associated with a poorer outcome of SLE. In this study, we found that high FIB-4 index was positively associated with other risk factors, such as SLEDAI score at admission, 24 h urinary proteins, neuropsychiatric and cardiopulmonary organ involvement (Table III). In Western countries, cardiovascular involvements and malignancies have become the leading causes of death among Western patients with SLE [11, 12]. In regard to cancers, a meta-analysis reported that liver cancer was more frequently observed in patients with SLE with a standardized incidence ratio (SIR) of 2.44 (95% CI: 1.46–4.05), compared to the general population [13]. Also the SIR of liver cancer was higher than the SIR observed for all the other cancers overall (1.16) or for lung (1.68), prostate (0.71) or bladder (1.78) cancer. As for cardiovascular involvement, a large body of evidence indicates that it is also associated with liver diseases, given that acute or chronic heart diseases can affect liver congestion and/or ischemia and impaired liver function can lead to heart failure [33, 34]. As for renal failure, high FIB-4 index has been suggested as an independent risk factor of prevalent chronic kidney disease in patients with NAFLD [15]. Even for neuropsychiatric involvement, accumulated epidemiological evidence has suggested that patients with elevated ALT level, liver cirrhosis, or liver disease have a significantly increased risk of intracranial hemorrhage and ischemic stroke [35, 36]. Also the mechanisms conferring the association are numerous, including endothelial dysfunction and vessel wall damage, inflammation, oxidative stress, and impaired hemostasis due to liver dysfunction [35]. Besides SLE itself, many studies have found that bacterial and fungal infections are common in patients with liver disease, especially among patients with liver cirrhosis and cirrhosis [37, 38]. Several biological mechanisms have been proposed to explain the susceptibility to infection among patients with liver disease, including bacterial translocation from the intestine, impaired hepatic clearance mechanisms, and immune paralysis of circulating immune cells [39].
Several limitations of this study should be acknowledged. First, we used blood tests to assess the liver function among patients without a liver biopsy and imagological examination, as they are seldom performed on SLE patients for liver function examination in routine clinical practice. Thus, information on patients diagnosed with liver cirrhosis was lacking. However, previous studies have validated the performance characteristics of scoring system methods in predicting hepatic fibrosis and overall mortality, regardless of etiology [17, 18, 27, 40–46]. Moreover, compared to the Child-Pugh and Model for End-Stage Liver Disease (MELD) scores, the FIB-4 index was better in predicating hepatic decompensation and HCC in HCV-positive persons, and showed no differences in predictive ability for mortality [47, 48]. Further studies still should be conducted to validate the performance of the FIB-4 index in predicating mortality among SLE patients. Second, we observed a very low percentage (less than 1%) of viral infections and alcohol drinking, because the majority of (92.5%) of SLE patients were female in this study, and the prevalence of alcohol drinking (9.4%) and viral infections of HBV (5.7%) and HCV (0.4%) was low among Chinese females in general [49]. Consistently, a study on 206 SLE patients reported that the causes of liver dysfunction were limitedly due to viral infections (0.8%), alcohol (1.6%), and fatty liver (17.9%), but mainly due to either SLE itself (30.9%) or drugs (28.5%) [4]. Moreover, we cannot include all risk factors of liver diseases due to the nature of the retrospective cohort study design. Thus, the causes of liver enzyme abnormalities were overall in this study. In spite of those limitations, however, the present study has several strengths as follows: 1) it was a large-scale multicenter cohort study; 2) having 15 years of mortality follow-up; 3) the key variables were from laboratory tests and detailed information on various mortality risk factors of SLE was collected; 4) both multivariate and stratified analyses were carried out for excluding potential confounding factors.
In conclusion, this retrospective cohort study is the first to report an association between higher FIB-4 index and increased overall mortality of SLE with a nonlinear dose-response relationship, and found no significant differences of AUCs between FIB-4 index and SLEDAI score. The FIB-4 index may potentially serve as an independent predictor for prognosis in SLE, and warrants further in-depth investigations.