Introduction
Natural killer (NK) cells are well known for their cytolytic function within the innate immune system and act as a natural defender protecting the human organism from infection and malignant cells [1, 2]. Several inhibitory receptors expressed on the surface of NK cells enable them to differentiate between normal and affected cells [3, 4] and increase their cytotoxicity against targets [5, 6], allowing for their efficacy in controlling cancer growth and spread.
NK cell activity (NKCA) is linked to the risk of cancer. A low level of NKCA leads to increased risk of developing cancer [7, 8], whereas high NKCA in the blood is associated with reduced cancer risk [9]. In addition, it has been shown that NK cells can be used as a prognostic marker in various carcinomas [10, 11]. Moreover, some studies have demonstrated a strong correlation between high NK cell cytotoxicity and reduced risk of colorectal cancer (CRC) in high risk individuals [11, 12]. At the same time, Jung et al. observed a gradual decrease in NKCA level as colonic adenoma transforms into CRC [13]. Similarly, 10 times higher risk of detecting CRC is reported with NKCA lower than 200 pg/ml [14].
While existing data on the link of NKCA and colonic neoplasia and CRC are growing in high-risk individuals, there are no data on the use of NKCA for CRC screening in the population at average risk.
Thus, the main goal of our study was to evaluate NKCA as a diagnostic marker for CRC and advanced neoplasia (AN) in an average risk population undergoing CRC screening by computed tomographic colonography (CTC). Also, the function of NK cells in association with demographic factors and health status of the general population was also assessed.
Material and methods
Study population
Average risk individuals of 45–75 years old eligible for CRC screening were invited to participate in an NKCA test trial along with evaluation by CTC. We invited subjects who had completed both CTC screening and follow-up endoscopic colonoscopy within our previous research study [15]. Using a pre-test questionnaire, the exclusion criteria included (i) any recent acute inflammatory process within 4 weeks or chronic diseases such as human immunodeficiency virus, hepatitis B or C viruses, (ii) history or current or previous malignant diseases, (iii) use of medications that may affect NK cell function, for example, immunosuppressive drugs, therapeutic immunoglobulins, methylprednisolone, anticoagulant drugs, etc. [16–18]. In addition, the average risk of participants for CRC was assured prior to the enrollment. The population at average risk for CRC comprised individuals without previously defined risk factors such as personal/family history of colorectal neoplasia and inflammatory bowel disease, having inherited syndromes linked with CRC or having type II diabetes, and others.
Study design
This prospective, cross-sectional observational study was approved by the institutional research review board and conducted at our tertiary cancer center, the Kazakh Institute of Oncology and Radiology (Almaty, Kazakhstan). All the participants have signed an informed consent form.
Blood sample collection and flow cytometry assay
On the same day as the scheduled CTC, 1 ml of venous blood sample was collected into the NK Vue tube (NKMax, Seongnam-si, South Korea) using a standard antecubital approach. Determination of NK cell activity was performed according to the previously described established method [19]. Briefly, during the test, the whole blood sample is stimulated with cytokine that results in NK cells secreting interferon γ (IFNG), subsequently quantified by the enzyme-linked immunosorbent assay (ELISA). A range of 25–2500 pg/ml was set for the NKCA level.
Computed tomography colonoscopy (CTC), endoscopic colonoscopy (EC), and histopathology
Scanning parameters and the protocol of CTC were according to the previously published articles [20]. Briefly, low-dose protocol (collimation 32 × 0.6, pitch 1.4, rotation time 0.5 s, 120 kVp, 50 mAs) was used for CTC acquisition. Colonic distension with carbon dioxide was achieved by an automatic insufflator. CTC examinations was evaluated by two experienced radiologists with more than 200 CTC examinations reads. CTC results were classified according to the CT colonography reporting and data system (C-RADS) categories [21]. C1 category of C-RADS represented a normal colon and/or benign colorectal findings; C2-C4 categories included findings consistent with colonic AN/CRC and thus considered as a positive result. All positive cases by CTC were referred for EC and subsequent biopsy and/or polypectomy. EC and histopathology evaluation were performed in accordance with the previously published standard methods [22] by endoscopists with 6 and 11 years of experience and pathologists with more than 10 years of professional experience, respectively. According to the histopathology results, colorectal lesions were classified as carcinoma, serrated or adenomatous polyps. The latter were subclassified as tubular, tubulovillous, or villous based on architectural patterns of the specimens. Adenomas greater than 10 mm and/or containing 25% and more villous component and/or those with severe dysplasia were defined as advanced adenomas. Pathologists were blinded to CTC and EC results and the CTC results were concealed from the endoscopists.
Data analyses
The qualitative values of the commercial NKCA ELISA based test were evaluated for advanced colonic adenoma and CRC. The performance of the NKCA test was evaluated using the main statistical measures such as sensitivity, specificity, negative and positive predictive values, likelihood ratio, overall test accuracy, clinical utility index, and others. To define the optimal cut-off value of NKCA a receiver operating characteristic (ROC) curve was plotted. The maximum vertical distance between the 45° diagonal no chance line and the ROC curve (maximum value of Youden’s index) was referred for the optimal cut-off point. Pearson correlation analysis was used to determine the association between NK cell activity and socio-demographic characteristics, and health conditions of participants. We calculated odds ratios (ORs) for developing CRC with 95% confidence intervals (CIs) using conditional logistic regression models. We used a web-based calculator (https://www.psycho-oncology.info/cui.html) to calculate the clinical utility index (CUI). Results were considered statistically significant when p-values were less than 0.05. All statistical analyses were done using the SPSS software version 21.0.
Results
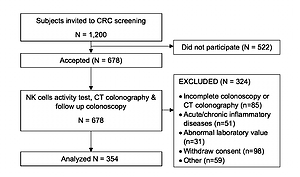
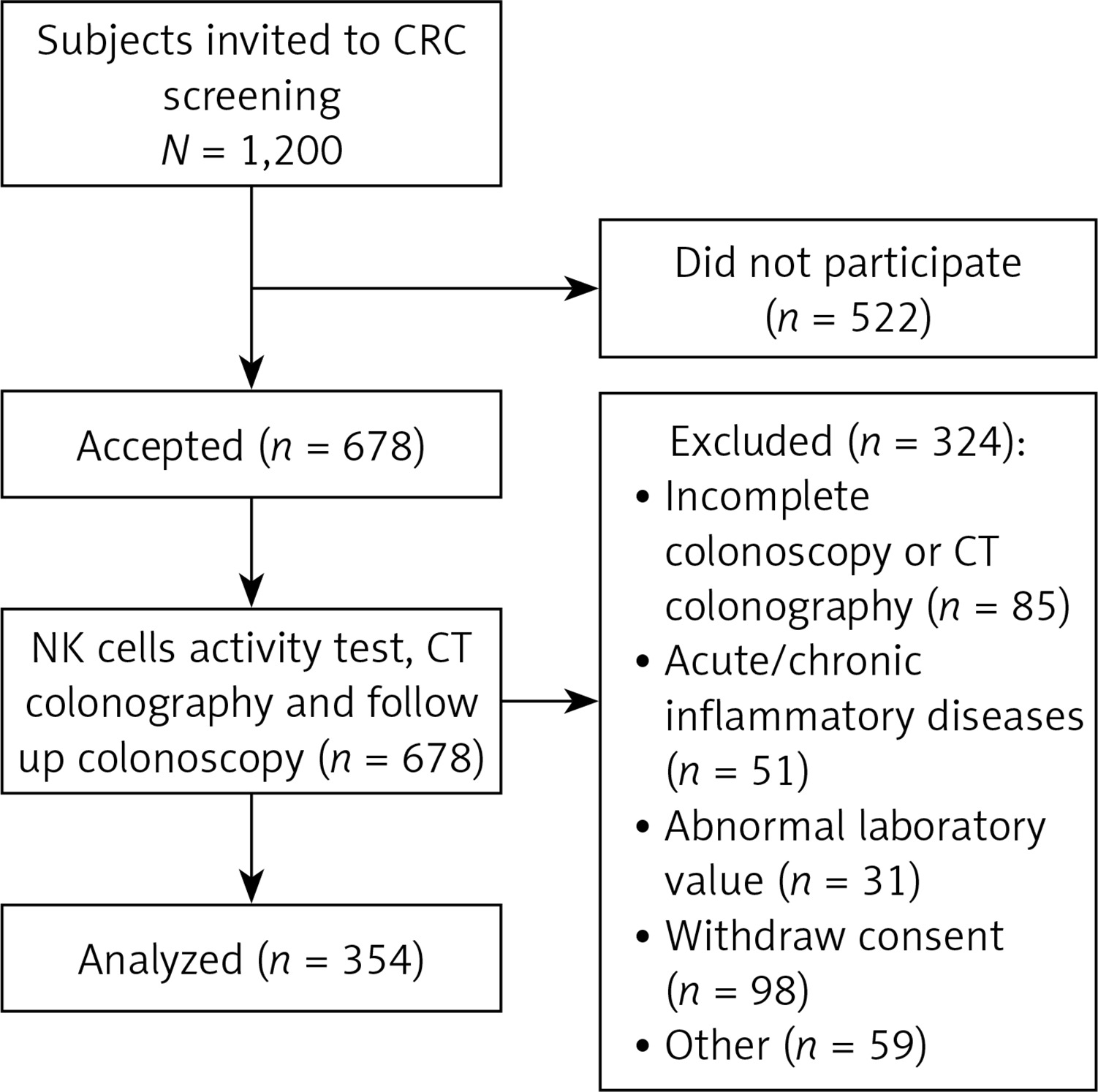
A total of 354 asymptomatic average risk individuals undergoing CTC screening in the city of Almaty (Kazakhstan) were enrolled in our study between June 2016 and July 2019 (Figure 1). The number of female participants was higher than males by 76.6% (226 vs. 128). Gender non-specific mean age was 58.5 years old, with male participants only slightly older than females (59.1 vs. 58.2 years old respectively). Table I provides the details on demographic and health status characteristics of the included cohort.
Table I
Characteristics of participants (n = 354)
CTC, EC, and histological examination detected 10 cases of CRC and 32 cases of AN. In addition, 6 cases of acute/subacute colitis were detected. According to both colonoscopy methods and histology results participants were subdivided into four groups: (1) control, (2) advanced colonic adenoma, (3) active colitis (AC), and (4) CRC.
A weak linear negative relationship was found between age and level of NKCA for males and for all participants in the control group (r = – 0.232 and r = – 0.185, respectively, p < 0.05). In women, there was a weak positive linear relationship between age and NKCA level, but the result was statistically non-significant (p = 0.84).
For the qualitative assessment, the median level of NKCA was 548.5 pg/ml for men and 500.0 pg/ml for women in the control group. The median NKCA was higher in non-smokers (544 pg/ml vs. 412 pg/ml in smokers; p = 0.03) and in physically active participants (653.5 pg/ml vs. 413 pg/ml in physically non-active; p = 0.02). The alcohol abusers had an NKCA level of 389 pg/ml, while the level for non-drinkers was 476 pg/ml (p = 0.12). NKCA level was higher in non-Asian participants compared to the Asian cohort including native Kazakhs, 514 pg/ml vs. 446 pg/ml (p = 0.04).
As shown in Table II, individuals with low NKCA were 6.84 times more likely to be diagnosed with CRC than those with a higher NKCA level (p < 0.001). Most significant differences of CRC prevalence in association with NKCA were present in females, 22.92 times the odds of having CRC vs. males. Thus, the difference was statistically significant only for females (p = 0.004).
Table II
CRC odds ratio according to NK cell activity (n = 354)
There was no statistically significant association of NKCA level and the prevalence of AN (OR = 0.62; 95% CI: 0.25–1.57, p = 0.314).
The median level of NKCA in CRC patients was 140 pg/ml (mean ± SD: 171 ±147). Patients with AC also had a decreased level of NKCA, 234 pg/ml (mean ± SD: 515 ±732). NKCA level in subjects with colonic AN was 392 pg/ml (mean ± SD: 425 ±257). In the control group, including C1 category by C-RADS, NKCA was higher in comparison with other groups, median 545 pg/ml (mean ± SD: 679 ±613). The difference of NK cell activity level between these four groups was significant, p < 0.05 (Table III).
Table III
NK cell activity level in participants with CRC, AC, AN and controls (n = 354)
| Groups | N (%) | Min. | Median | Max. | Mean | SD | P-value |
|---|---|---|---|---|---|---|---|
| Control | 306 (86.5) | 5.9 | 544.8 | 2516 | 679.3 | 613.0 | |
| AN | 32 (9.0) | 6.0 | 392.0 | 1009.7 | 424.8 | 257.3 | 0.04 |
| AC | 6 (1.7) | 75.5 | 234.1 | 572.7 | 515.1 | 731.9 | 0.14 |
| CRC | 10 (2.8) | 25.5 | 140.4 | 422 | 171.0 | 147.4 | 0.048 |
The calculation of Youden’s index based on ROC analysis determined the optimal NKCA cut-off value. In our study, the maximum Youden’s index (0.693) was achieved at the level of 200 pg/ml. The false negative rate of the test in the diagnosis of CRC at this cut-off point was 13%. The level of 200 pg/ml has also been validated from the previous trial as the optimal cut-off level [14].
Diagnostic power of the NKCA test is summarized in Table IV. Overall, the sensitivity of the test for CRC was significantly higher than that for AN, as well as for the combined CRC and AN group (71.4% vs. 20.7% and 35.7%, respectively). Accuracy of the NKCA test was 75.5% to detect CRC, with sensitivity of 71.4% and specificity of 75.6%. The accuracy of the test in diagnosing AN was 72.3%, with lower sensitivity compared to that for CRC, but relatively similar specificity (20.7% and 73.2%, respectively). Negative predictive value (NPV) of the NKCA test was high for all CRC, AN and combined CRC/AN groups (98.9%, 98.2 and 96.4% respectively).
Table IV
Diagnostic accuracy of NKCA in diagnosing colonic AN and CRC with the cut-off value of the test 200 pg/ml (n = 354)
The NKCA test demonstrated a good utility for ruling out AN and CRC with a negative CUI of 0.741 (95% CI: 0.697–0.774) and 0.664 (95% CI: 0.626–0.702), respectively, while the positive CUI was very poor – 0.053 (95% CI: 0.018–0.096) vs. 0.011 (95% CI: 0–0.110) for AN and CRC respectively. It should also be noted that the probability that subjects with a low NKCA level truly have CRC or AN is very low (PPV – 7.8% and 1.3%, respectively).
Discussion
To the best of our knowledge, our study was the first to evaluate the association of NKCA level with prevalence of CRC and AN in an average risk population undergoing CTC screening. The NKCA test showed good accuracy to detect CRC and AN; however, the sensitivity and specificity were lower than previously published results [14]. Specifically, in the Canadian trial, which included subjects with high risk for CRC, the NKCA test had 87.0% sensitivity and 60.8% specificity in diagnosing CRC, with PPV and NPV of 5.7% and 99.4%, respectively.
Low sensitivity of the test to detect AN and very poor positive CUI values for both CRC and AN limit the clinical utility of the NKCA test as a primary screening test for CRC and AN. However, high NPV of the test in both conditions in our study suggests its potential ability to rule out the disease, even with an average risk for CRC.
Our study demonstrated that the likelihood of CRC is very low in average risk population, if NKCA is above 200 pg/ml. At the same time, the risk of having malignant colonic neoplasms is 6.84 times higher in participants with NKCA below 200 pg/ml. Previously, it has been shown that subjects with low NKCA were at 10 times higher risk of being diagnosed with CRC than those who had values greater than 200 pg/ml [14]. But then again, the included subjects in that study were different and not entirely comparable.
The present study demonstrated that CRC patients had decreased IFNG secretion by NK cells. Tallerico et al. observed that differentiated CRC cells were highly resistant to NK cells [23]. In the previous study it was found that CRC tissues had low density or no infiltrating NK cells when the cancer tissue was evaluated immunohistochemically [24]. However, the authors found increased density of infiltrating NK cells in colonic adenoma tissue than in surrounding normal mucosa. Our findings revealed that participants with AN had a lower median NKCA level than did healthy controls. Therefore, we propose that colonic adenomas do not fully escape from NK cell-mediated immunosurveillance, as the NK cells can still migrate to adenoma tissue, as the study of Halama et al. demonstrated [24], but the function of the cells are obviously impaired. However, to date, there are no data to conclude that high serum NKCA level or high density of infiltrating NK cells in adenoma tissue can prevent adenomas from transforming into CRC or slow that process down. Therefore, analyzing the impact of NKCA on colonic AN is important in order to find ways of creating a cancer-protective environment and to develop anti-cancer drugs.
In addition, our results support healthy habits in reducing risk of colonic neoplasia, even in individuals at average risk for CRC. We have found that exercisers had a higher NKCA level than physically inactive participants. These results are congruent with previously established data on increased anti-cancer immunity with regular physical activity [25–27]. We also found that NK cell activity was higher in non-smokers than smokers. As for the alcohol consumption, the median level of NKCA was lower in this group than in smokers and physically inactive participants. These facts deserve special attention as they suggest that smoking and excessive alcohol use can cause reduced immunity, and, consequently, increased risk of cancer. Conversely, increased NKCA might have a protective effect against malignant cells. Recently, Legaz et al. ascertained that the presence of killer cell immunoglobulin-like receptors expressed on the surface of NK cells has a protective effect against alcoholic cirrhosis, which is the main risk factor for hepatocellular carcinoma [28]. However, these hypotheses must be supported by further research.
Our findings further showed that gender and ethnicity might be linked to the risk of CRC, given lower NKCA in female participants and those of Slavic descent. This is similar to the previous epidemiological study demonstrating 4 times higher prevalence of CRC in Slavic ethnic residents of Kazakhstan compared to the Asian population [29].
Several limitations of our study must be noted. The main limitation was a small sample size. Also, we used questionnaires to exclude active infections and other health conditions that can affect NKCA, but no laboratory testing was used for confirmation. In addition, the prevalence of CRC and AN was low in our cohort, which is expected given the average risk for the included individuals. This also might be a reason why PPV of the test was low in our study. Finally, we observed a decreasing NKCA level with increasing age, suggesting that individuals outside the 45–75 age group may have different levels of NKCA. Thus, these differences may limit the generalizability of the study to populations of other age groups.
In conclusion, our results suggest that the NKCA test can be used as a potential biomarker to identify subjects at high risk for CRC among the general population. In addition, high level of NK cell function, regular exercise, lack of smoking and alcohol consumption habits might be linked to a lower risk of CRC detection in average risk population.