Introduction
Excess body weight poses significant public health challenges worldwide, with rising prevalence and serious health consequences [1, 2]. Problems associated with excess body weight impose a substantial burden on healthcare systems and lead to high social and economic costs [3]. According to the World Health Organization (WHO), being overweight is defined as having excessive fat deposits, while obesity is classified as a chronic, complex disease characterized by excessive fat deposits that can impair health [4]. The negative effects of excess body weight on health-related quality of life are well documented [5, 6]. Along with its high prevalence, excess body weight has been linked to poorer physical, mental, and sexual health [7].
The approach to sexuality focuses mainly on medical aspects, often overlooking other equally important dimensions, such as subjective evaluations of sexual life, overall satisfaction levels, and perceptions of sexual performance [8, 9]. Sexual functioning can be described as the engagement of motivators such as sexual attraction and desire, while also considering the significance of health, psychosocial factors, and body image self-assessment [10, 11], all of which influence the evaluation of sexual life. It is closely linked to overall health and subjective well-being [12]. Furthermore, it represents a key component of psychosocial functioning and strongly correlates with overall quality of life [13]. Problems in this area may lead to mental health issues, reduced self-esteem, tension in interpersonal relationships, and negative effects on professional performance – including among the professional group of healthcare workers [14, 15]. Due to the physical, mental, and social demands of their profession, healthcare workers may be at higher risk of experiencing diminished sexual functioning [16–19].
Excess body weight is associated with sexual functioning, making it an important area of interest in public health [20]. Individuals with excess body weight are more likely to experience reduced libido, lower sexual satisfaction, erectile dysfunction, and negative body image, which are linked to lower satisfaction and decreased sexual activity [21, 22]. The potential mechanisms underlying the negative impact of excess body weight on sexual functioning are multifactorial and complex. These include the secretory activity of adipose tissue, the relationship between excess body weight and comorbidities affecting sexual health, hormonal imbalances, and psychological factors such as body image concerns, low self-esteem, and fear of rejection, all of which can lead to sexual dysfunction [23–26].
Given the increasing prevalence of overweight and obesity, a more comprehensive approach is necessary to analyze their relationship with sexual functioning. This approach should consider both direct and indirect mechanisms, including self-rated health and perceived physical attractiveness. Previous studies have primarily focused on sexual dysfunctions in women and erectile disorders in men. However, since sexuality involves multiple dimensions, including interactions between psychosomatic mechanisms inherent to individuals and the socio-cultural contexts in which they operate, it is essential to move beyond the analysis of purely physical sexual dysfunctions. Instead, a broader perspective on the components of sexual health should be adopted.
The aim of the present study was to examine the extent to which body weight impacts sexual life evaluation among healthcare workers in Poland, considering such mediating factors as self-rated health, perceived physical attractiveness, stress, and sleep disturbances.
Material and methods
Design of the study
A nationwide cross-sectional quantitative study was conducted in Poland between 21 February and 28 April 2022, as part of a project examining the health and health behavior of health care workers. The sampling frame consisted of a database of 2,894 hospitals and outpatient clinics across all of Poland’s 16 provinces (voivodships). The facilities were selected at random to ensure a representative distribution across demographic and healthcare structures in Poland. The analysis included staff from 99 randomly selected healthcare facilities nationwide, where the management consented to participate in the study. The study was conducted using a computer-assisted web interview (CAWI) supported by a paper-and-pencil interview (PAPI).
Participants
A total of 1,478 respondents from three main employment categories in healthcare facilities were included in the analysis (physicians N = 407, nurses N = 928, paramedics N = 143). The group sizes were diversified according to the project design assumptions, which specified the minimum target sample size, required representation of occupational groups, and geographic variation reflecting the employment structure in Polish healthcare [27]. Cases with missing data for any of the analyzed variables were excluded from the study. Consequently, respondents who did not respond to these variables were excluded from the analyses.
Questionnaire
Respondents provided anonymous answers to closed-ended questions, primarily on nominal or ordinal scales, as well as visual analog scales. Participation in the survey was voluntary, with respondents providing informed consent and having the option to withdraw at any time.
Research tools
In the present study, a subset of questions from the questionnaire was selected for analysis. The main outcome variable was a composite index of sexual life evaluation, based on two questions developed by the research team. These questions were part of a broader block addressing various aspects of life, including satisfaction with one’s sexual life, sexual performance, and sexual capabilities.
Responses were recorded using a five-point Likert scale, ranging from “very good” to “very poor,” with an option to decline answering or skip the question for participants who had so far not become sexually active in their lives. The composite index ranged from 2 to 10 points, with higher scores indicating a better evaluation of sexual life. According to principal component analysis (PCA), this total index is homogeneous, with both factor loadings at 0.93, and demonstrates good internal consistency (Cronbach’s α = 0.93).
The independent variables were defined such that higher levels indicated greater dysfunction.
Body weight
The study included a question about current body weight in kilograms and height in centimeters, allowing for the calculation of BMI using the formula: weight divided by height squared (kg/m2). The following BMI categories were applied: 18.5–24.99 for normal weight, 25–29.99 for overweight, and >30 for obesity.
Self-assessment of health problems
Subjective health problems were assessed using a question from the same set of items that evaluated different aspects of life, including the dependent variable. The response options were standardized and grouped into three categories by combining the most extreme answers (very good + good rating and bad + very bad rating).
Body image self-assessment
Another question from the same block focused on participants’ subjective evaluations of their own physical attractiveness, which served as an indicator of body image self-assessment. Responses were recoded into three categories by combining the most extreme answers (very good + good rating and bad + very bad rating).
Stress
Stress levels were measured using the 4-item Perceived Stress Scale (PSS-4), also known as Cohen’s scale [28]. The scale includes five response categories, ranging from “never” to “very often”, based on experiences during the past month. The total score ranges from 0 to 16 points, with higher scores reflecting higher stress levels (two items were reverse-coded in this respect). According to PCA analysis, the scale is not homogeneous, with factor loadings of 0.91 and 0.92, respectively, and a single-factor reliability score of 0.57.
Sleep
Sleep disturbances over the past month were evaluated using the 4-item Jenkins Sleep Scale (JSS-4). Responses ranged from “0” (not at all) to “5” (22–31 days). Total scores for sleep disturbances range from 0 to 20, with higher scores indicating more frequent sleep disturbances [29]. According to PCA analysis, the scale is homogeneous, with factor loadings from 0.84 to 0.92, and demonstrates good internal consistency (Cronbach’s α = 0.90).
In addition, demographic and social characteristics were included in the analyses: sex, age, relationship status, and occupation.
Statistical analysis
The factor structure of the applied scales was evaluated using PCA, and their reliability was assessed with Cronbach’s α.
In univariate analysis, correlations between continuous, quasi-continuous, or ordinal variables were examined using Spearman’s coefficient. For comparisons of means, the nonparametric Mann-Whitney U test (for two independent samples) or the Kruskal-Wallis H test (for three independent samples) was applied. In the latter case, post hoc multiple comparisons with Bonferroni correction were also performed.
For multivariate analysis, a hierarchical linear regression model was estimated for the dependent variable – the sexual life evaluation index. Results from the four steps of the analysis were presented as unstandardized betas with 95% confidence intervals (CI), and model fit was assessed using the coefficient of determination (R2).
To identify complex pathways of relationships between variables, structural equation modeling (SEM) without latent variables was used. The models analyzed the direction of hypothetical relationships, the significance of path coefficients, root mean square error of approximation (RMSEA) with 95% CI, comparative fit index (CFI), normed fit index (NFI), and relative fit index (RFI). Modification indices (MI) were also considered, adding potential connections as needed, but without correlating error terms. The model for the entire sample was modified until all non-significant paths were eliminated and MI values fell below 4. Separate models for men, women, and healthcare worker groups were estimated using the same framework without further modifications, to highlight any non-significant relationships between variables. The analysis also examined matrices of total, direct, and indirect effects.
SPSS 29.0 and AMOS 29.0 (IBM Corp. Released 2024. IBM SPSS Statistics for Windows, Version 29.0. IBM Corp., Armonk, NY, USA) were used for data analysis. A significance level of p < 0.05 was adopted for all tests.
Results
Demographics and sexual life evaluation index
The basic demographics of the analyzed sample are presented in Table I. The sample had the largest proportion of nurses (62.8%), followed by physicians (27.5%), and the smallest group consisted of paramedics (9.7%). The high proportion of women (77.6%) reflects the employment structure in Polish healthcare facilities. The average age of respondents was 46.74 years, with the highest average age observed among nurses (48.12 years) and the lowest among paramedics (37.68 years). The majority of respondents were over 50 years old (46.1%) (respondents over 65 years constituted 2.1% of the total sample) and were currently in a relationship (88.3%). Respondents with excess body weight accounted for 54.7% of the sample.
Table I
Sexual life evaluation index by socio-demographic characteristics and BMI
Table I also shows the average evaluation of sexual life across different respondent groups. The overall mean index for the entire sample was 7.51 ±1.86. Statistically significant differences (p < 0.001) were found in relation to all factors except sex, where the result was borderline. Higher sexual life evaluations were reported by respondents aged 20–29, those in relationships, paramedics, and those with normal BMI.
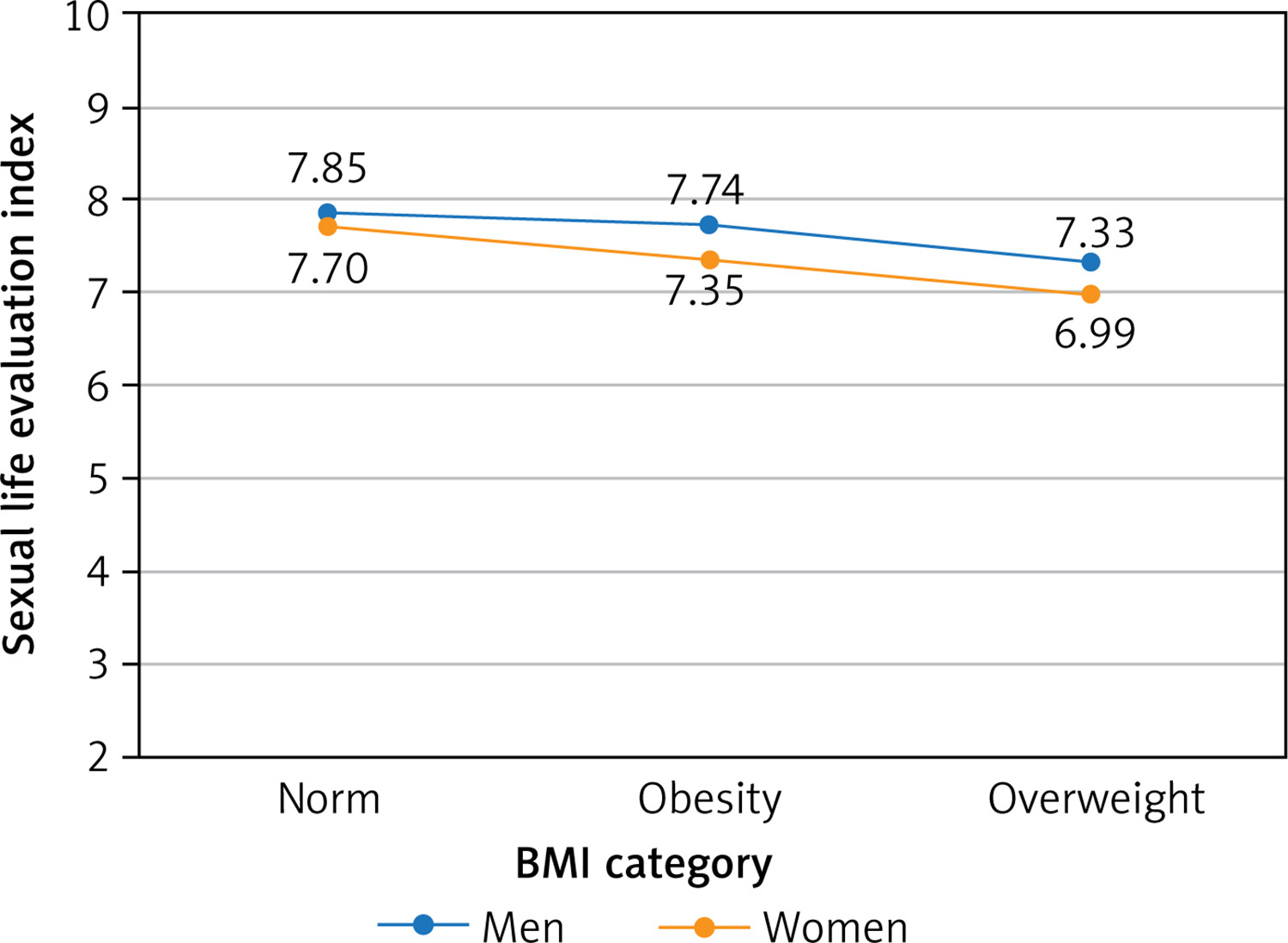
Given the main focus of the present study, it is important to highlight the differences between BMI groups, particularly the consistent decline in sexual life self-assessment with increasing levels of excess body weight (p < 0.001). Post hoc analysis revealed significant differences between all three group pairs – normal weight vs. overweight (p = 0.012), normal weight vs. obesity (p < 0.001), and overweight vs. obesity (p = 0.016).
Figure 1 plots the sexual life evaluation index by BMI, divided by sex. Women in all BMI categories rated their sexual lives lower than men, with sex differences being significant in the overweight group (p = 0.036). Despite a clear downward trend observed in both sexes, statistically significant differences between BMI groups were found only among women (p < 0.001).
Sexual life evaluation based on socio-demographic characteristics, BMI, and life assessment
Table II presents potential relationships between the analyzed continuous, quasi-continuous, and ordinal variables.
Table II
Spearman’s correlations (rho) between analyzed variables
Sexual life evaluation, as a positively oriented variable, showed a significant negative correlation with age, health assessment, physical attractiveness assessment, stress, sleep, and BMI (p < 0.001). The strongest correlations with sexual life evaluation were observed for health problems and two additional factors – impaired body image self-assessment and sleep disturbances.
In contrast, BMI showed a significant positive correlation with age, health problems, and impaired body image self-assessment (p < 0.001).
Variability in sexual life evaluation
Table III presents four regression models. Each model was adjusted for sex, relationship status, and occupation, which were recoded into two dummy variables (data not shown here).
Table III
Hierarchical linear regression* for variability in sexual life valuation index
In Model 1, BMI and age were identified as significant predictors of sexual life evaluation (R2 = 0.065; p < 0.001).
In Model 2, an additional variable – health problems self-assessment – was introduced, leading to a substantial increase in R2 (0.270). BMI and age remained significant predictors.
Model 3 incorporated two more variables – stress and sleep – which resulted in a slight further increase in R2 (0.291), without altering the significance of other parameters.
Finally, Model 4 added impaired body image self-assessment, which significantly improved the model fit, as measured by R2 (0.365). The inclusion of this new factor – perceived physical attractiveness – eliminated BMI as a predictor of variability in sexual life evaluation. Additionally, the β coefficient for age increased, whereas it decreased for other independent variables.
In the next step, a path model was estimated to identify the more complex mechanism of relationships between the analyzed variables, distinguishing between direct and indirect effects. This analytical approach corresponds to the estimation of a set of regression equations in which BMI can be the dependent or independent variable, also indirectly influencing the variability of the sexual life assessment index. For the defined path model estimated for the entire sample, the results showed cmin/df = 1.140, and the fit indices were as follows: RMSEA = 0.017 (95% CI: 0.000–0.042). The NFI, RFI, and CFI values were 0.996, 0.983, and 0.999, respectively.
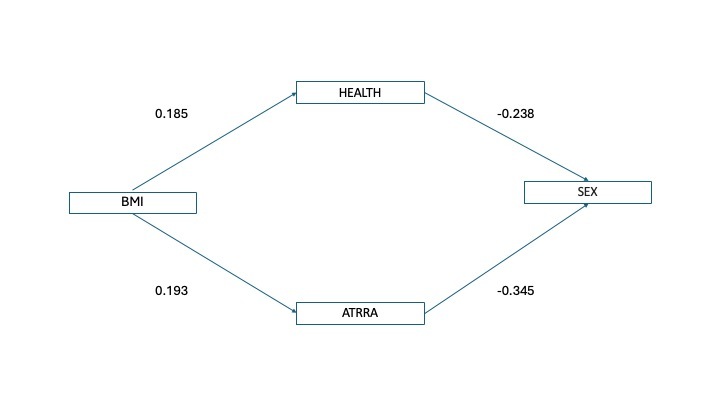
As presented in Table IV and illustrated in the graphical representation of the model (Figure 2), the structure consists of six interconnected linear equations. Age, as a non-modifiable factor, acts solely as an independent variable, while sexual life evaluation is treated as the only dependent variable, without influencing the variability of other variables. In the resulting model, sexual life evaluation has five significant predictors. BMI is determined only by age and is indirectly associated with sexual life evaluation, primarily through its link to physical attractiveness assessment. Sleep and stress levels are also associated with sexual life evaluation.
Table IV
Standardized regression weights for SEM models in the general population

Of particular note is the negative assessment of physical attractiveness, which was found to have four significant predictors and emerged as the strongest factor influencing variability in sexual life evaluation.
The matrices of indirect and direct effects (Appendix 1, Supplementary Tables SI–SIII) indicate that while physical attractiveness has the strongest direct effect on variability in sexual life evaluation (–0.345), health problems produce the strongest indirect effect (–0.197). However, the second most important factor generating an indirect effect is BMI (0.150), which is the only variable with a zero direct effect (Table IV). A comparison of gender specific SEM models is provided in Appendix 2.
Discussion
This study evaluated the relationship between body weight and sexual life evaluation in healthcare workers in Poland, using both linear modeling and direct and indirect associations. While numerous studies suggest a link between increased body weight and impaired sexual functioning, only a few have conducted extensive analyses of both direct and indirect relationships [20, 30–32]. In the path model, five factors were directly correlated with variability in sexual life evaluation: impaired body image self-assessment, health assessment, elevated stress levels, sleep disturbances, and age. Our findings indicate that body weight is associated with sexual functioning through an indirect relationship with self-rated health and physical attractiveness.
Health issues among healthcare workers, including those related to excess body weight, are particularly important for public health, as they can impact their ability to provide patient care [33]. In our study, the average BMI was 26, which aligns with findings from other studies, where the average BMI among healthcare workers was 25.4 [34]. Additionally, our results show that BMI was significantly positively correlated with both age and self-rated health (p < 0.001). Furthermore, weight gain among healthcare workers has shown an upward trend, exacerbated by the COVID-19 pandemic and its negative effects on both physical and mental health [35].
Global prevalence data indicate that reduced sexual life evaluation, including lower sexual functioning, represents a significant public health issue [36]. In our bivariate analysis, higher BMI was associated with poorer sexual life evaluation (p < 0.001), which is consistent with other studies [20, 24]. However, self-rated health and physical attractiveness proved to be stronger differentiators of sexual life evaluation than BMI (p < 0.001). In our study, hierarchical regression analysis showed that adding health assessment and physical attractiveness to the model eliminated BMI as a predictor of variability in sexual life evaluation. This suggests that these variables may play a mediating or moderating role in this correlation. These findings align with other studies evaluating the relationship between body weight and sexual functioning, where health factors and physical attractiveness were identified as key variables influencing this association [20, 23–25]. The results of the hierarchical model prompted further exploration of these connections.
The remainder of this discussion section primarily focuses on self-rated health and physical attractiveness, as these factors were most strongly associated with BMI and sexual life evaluation.
In our study, 29.1% of respondents reported a lower health assessment, including 9.3% who indicated serious health problems. Given its ability to predict mortality and morbidity, self-rated health is a critical indicator of population health [33, 37]. Our path model demonstrated that health assessment had a strong direct association with variability in sexual life evaluation (–0.238), consistent with previous studies [20, 24].
Another key variable in our study is physical attractiveness (body-image self-assessment). Self-assessment reflects self-worth, encompassing beliefs about oneself and emotional reactions to those beliefs [38]. As such, self-assessment can act as a predictor of life satisfaction, representing self-value in specific contexts and environments. Western studies on physical attractiveness have largely focused on body appearance, particularly weight and body shape [39], which are core components of body image [40]. In our study, 13.1% of respondents reported impaired physical attractiveness assessment, while 27% had moderately impaired assessments. Additionally, higher BMI was associated with lower body image ratings (p < 0.001), a finding in line with other studies showing BMI’s influence on perceptions of physical attractiveness [41]. Weaver and Byers [42] found that women who view themselves as more attractive report higher sexual satisfaction, likely due to greater confidence and comfort in intimate relationships. These findings are consistent with a meta-analysis by Cash and Pruzinsky, which identified positive body image as a key predictor of high sexual satisfaction [43]. In our study, the path model demonstrated that physical attractiveness assessment had the strongest direct relationship with variability in sexual life evaluation (–0.345). These results are supported by prior studies, which showed that body image and self-perceived attractiveness strongly correlate with overall life satisfaction, including sexual satisfaction, by enhancing self-esteem and emotional well-being [44, 45]. These findings reinforce that a positive body image, including views of genital appearance and self-perception, is associated with higher sexual satisfaction and better sexual life evaluation. This highlights the need for interventions aimed at improving body image and addressing cultural pressures related to appearance [46].
In our study, other factors potentially influencing sexual life evaluation were also identified. Age was negatively associated with sexual life evaluation through lower self-rated attractiveness. Older age is also linked to poorer health outcomes, higher risk of sexual dysfunctions, and a greater number of individuals without romantic partners, which may further impact sexual functioning [47]. Sleep disturbances also play a key role in human health, including mental, physical, and sexual health. Greater sleep disturbances were associated with poorer sexual life evaluation, while better sleep was linked to higher scores [48, 49]. Elevated stress levels also emerged as a significant factor negatively influencing sexual life evaluation, consistent with previous research [50]. Finally, sex differences were observed, with women reporting poorer sexual life evaluations as BMI increased (p < 0.001).
This study was cross-sectional in design; therefore, causal relationships could not be established. However, the use of structural equation modeling (SEM) enabled the identification of complex pathways between key variables and allowed for the determination of influence trajectories. The sexual life evaluation index was based on two questions that are not part of a validated scale. Nevertheless, these questions have been successfully used since 1997 in cyclical studies on sexuality and health. The analyses also did not consider the presence of comorbidities, which may affect sexual functioning. However, self-rated health, one of the key variables, is closely related to the occurrence of comorbidities [37].
Further research should include longitudinal studies to better illustrate cause-and-effect relationships. Future studies assessing the relationship between body weight and sexual functioning should consider changes in body weight as a key indicator and examine the interactions of these factors in more depth. Additionally, future research should include a detailed assessment of sexual functioning using validated scales to capture a more comprehensive picture of the relationships involved.
In conclusion, excess body weight is associated with numerous chronic diseases, lower self-esteem, and reduced sexual life evaluation. Our study provides a comprehensive analysis of the correlation BMI and sexual life evaluation, exploring both direct and indirect associations, while accounting for self-rated health and physical attractiveness. The findings highlight a strong link between body weight and sexual life evaluation, primarily mediated by self-rated health and, in particular, physical attractiveness, which emerged as the strongest predictor in our study. In the future, educational programs addressing sexual health should be developed and implemented among individuals with excess body weight as part of treatment strategies.