Introduction
Iron deficiency is still a health problem in the world. The prevalence of iron deficiency anemia (IDA) in children under five is still high globally, in Southeast Asia and Indonesia, around 40% [1, 2]. In South Kalimantan, especially the city of Banjarbaru, the incidence of iron depletion, iron deficiency (ID), and IDA in infants aged 0–6 months is relatively high, namely 28.0%, 27.0%, 40.8% [3]. Iron deficiency anemia is crucial considering its long-term effects that can interfere with baby growth and development. Several studies have shown the impact of IDA on cognitive and behavioral deteriorations [4–7].
One of the IDA prevention efforts is the early detection of iron deficiency. Various laboratory parameters to detect iron deficiency include erythrocyte indices such as mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH), mean corpuscular hemoglobin concentration (MCHC), red blood cell distribution width (RDW), RDW index, Mentzer index, serum iron (SI), total iron-binding capacity (TIBC), transferrin saturation (TS), ferritin, soluble transferrin receptor (sTfR), hepcidin, peripheral blood smear, and bone marrow examination [8–11]. The limitations of the parameters mentioned above include the requirement of a large number of blood samples, high cost, the influence of inflammatory conditions, infections, diurnal phase, and being limited to certain health facilities [1, 12, 13].
One of the iron deficiency parameters that is easy, inexpensive to apply, and recommended by the American Academy of Pediatrics (AAP) is the reticulocyte hemoglobin equivalent (Ret-He), which assesses the amount of hemoglobin in reticulocytes [12, 14]. The Ret-He examination can detect iron deficiency before a decrease in hemoglobin (Hb) levels or anemia occurs.
This study aims to compare the Ret-He examination as a diagnostic parameter of ID and IDA in infants aged 1–4 months, with the diagnostic criteria of ID and IDA according to Ringoringo (2008) [3].
Material and methods
Study population
This study was a diagnostic test with 403 infants aged 1, 2, 3, and 4 months who met the inclusion and exclusion criteria at 10 Community Health Centers in Banjarbaru, South Kalimantan, from August 2020 to August 2021. The infants have breastfed. The inclusion criteria were infants aged 1–4 months who were declared clinically healthy by the in-charge doctor, and the infants did not suffer from major congenital abnormalities. Exclusion criteria were infants who had received/are receiving elemental iron therapy, suffered from hematological-oncological diseases at the time of blood collection, or the parents or guardians of the infants refused to participate in the study.
Before the research was carried out, the researchers conducted briefing and training on all research procedures, from baby recruitment and measurement of anthropometric parameters to blood collection to health workers. As a result, all procedures were carried out uniformly with the same perception. Nutritional status is assessed based on body weight (W) according to length (L), and it is divided into good nutrition and undernutrition. In this study, it was considered good nutrition if the z-score was –2 SD to +2 SD and undernutrition if the z-score was < –2 SD. W/age: normal (–2 ≤ Z ≤ +2SD), underweight (–3 ≤ Z < –2SD). L/Age: normal (–2 ≤ Z ≤ +2SD), short stature (–3 ≤ Z < –2SD) [15]. Ethical clearance was obtained from the Research Ethics Commission, Faculty of Medicine, University of Lambung Mangkurat Banjarmasin No. 272/KEPK-FK UNLAM/EC/VIII/2020.
Blood sampling
The infant’s parents were asked for informed consent to participate in the study. In addition, primary data were taken in the form of age, gender, weight, height, head circumference, birth history, parental education, parents’ occupations, economic status, and physical examination data to ensure the baby was in good health. A venous blood sample was taken by health personnel with a new 1 ml syringe from the median cubital vein for each infant. First, the blood sample was taken to the Idaman Hospital Banjarbaru Laboratory; then, Ret-He and complete blood count were examined using the Sysmex XN-450 Hematology Analyzer (Sysmex Corporation, Japan). Peripheral blood smear examination was performed using an Olympus microscope (Olympus CX23 Microscope Binocular Laboratory, Japan) by a pediatric hemato-oncologist in a blind manner.
The criteria for diagnosis of ID and IDA based on Ringoringo’s 2008 criteria are as follows [3]:
1. Hb levels are less than the lower limit of the normal value for infants’ Hb levels at a certain age (1 month 13.2–13.8 g/dl; 2 months 11.6–12.3 g/dl; 3 months 11.3–11.9 g/dl; 4 months 11.5–11.9 g/dl).
2. Peripheral blood smear showing microcytic and/or hypochromic cells.
3. RDW is greater than the lower limit of the average RDW value for infants at a certain age (1 month 15.9%; 2 months 14.7%; 3 months 13.8%; 4 months 13.5%).
4. Mentzer index > 13, where the Mentzer index = (MCV)/RBC.
5. RDW index > 220, where the RDW index = (MCV)/RBC × RDW.
6. MCV is less than the lower limit of the normal MCV value at a certain age (1 month 92.4–93.4 fl; 2 months 85.5–86.6 fl; 3 months 79.5–80.7 fl; 4 months 75.8–77.1 fl).
It is called iron deficiency anemia when it meets criteria 1 and 2 and at least one of the four criteria 3, 4, 5, and 6. Iron deficiency in infants aged 1–4 months is established when the Hb level is normal and diagnostic criterion 2 is met plus at least one of the four criteria 3, 4, 5, 6.
Results
This study involved 403 infants aged 1, 2, 3, and 4 months. The characteristics of all infants can be seen in Table I. The complete blood count (CBC) and Ret-He results can be seen in Table II. Table III shows the prevalence of ID and IDA in infants aged 1–4 months of 10.9% and 58.6%, respectively. Table IV shows the Ret-He cut-off values for ID and IDA at 1, 2, 3, and 4 months of age with sensitivity, specificity, positive predictive value, and negative predictive value.
Table I
Characteristics of 403 infants aged 1, 2, 3 and 4 months
Table II
Mean values of complete blood count and Ret-He for infants aged 1, 2, 3 and 4 months
Table III
Prevalence of iron deficiency (ID) and iron deficiency anemia (IDA) in infants aged 1–4 months
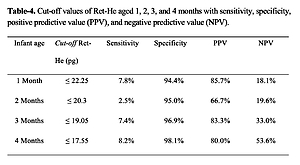
Table IV
Cut-off values of Ret-He aged 1, 2, 3, and 4 months with sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV)
| Infant age | Cut-off Ret-He [pg] | Sensitivity | Specificity | PPV | NPV |
|---|---|---|---|---|---|
| 1 month | ≤ 22.25 | 7.8% | 94.4% | 85.7% | 18.1% |
| 2 months | ≤ 20.3 | 2.5% | 95.0% | 66.7% | 19.6% |
| 3 months | ≤ 19.05 | 7.4% | 96.9% | 83.3% | 33.0% |
| 4 months | ≤ 17.55 | 8.2% | 98.1% | 80.0% | 53.6% |
Discussion
This study recruited 403 infants aged 1, 2, 3, and 4 months which were taken consecutively from 10 Community Health Centers in Banjarbaru City, South Kalimantan, considering the high incidence of iron deficiency and IDA in infants, especially under 6 months in Banjarbaru City [3]. A total of 100% of the subjects were included in the data analysis. From the characteristics of the infants in Table I, the average birth weight is 3062 g, birth length is 49.5 cm, and birth head circumference is 33.3 cm. The total number of infants with underweight is 26 (6.5%), short stature is 39 (9.7%), and undernutrition is 24 (6.0%). The number with a history of preterm birth was 19 (4.7%) infants and LBW 38 (9.4%) Infants. Risk factors for iron deficiency in infants are prematurity, birth weight, and nutritional factors [9, 11, 12].
Based on Table III, it can be seen that the prevalence of iron deficiency in infants aged 1–4 months is 10.9%, and the prevalence per category of age 1 month, 2 months, 3 months, and 4 months is 13.9%, 9%, 13%, and 7.8%, respectively. The prevalence of IDA in infants aged 1–4 months was 58.6%, and the prevalence per age category of 1 month, 2 months, 3 months and 4 months was 68.3%, 71%, 55%, and 40.2%, respectively. The prevalence of IDA in this study is higher than the prevalence of IDA among children under five in the world, 39.8%; and in Indonesia, 38.4% (in 2019) [16]. A prospective cohort study of 211 newborns in Banjarbaru showed that the incidence of IDA in infants aged 0 months, 1 month, and 2 months was 11.8%, 10.9%, and 11.3%, respectively [3]. The high prevalence of ID and IDA in this study may be related to the time of the study during the COVID-19 pandemic, which indirectly impacted the socioeconomic community and nutrition of pregnant-breastfeeding mothers.
Reticulocyte hemoglobin equivalent indicates the adequacy of iron in the bone marrow because this test measures Hb in reticulocytes or iron input in red blood cells during erythropoiesis [17, 18]. The cut-off value is between normal and abnormal or positive and negative test results. The cut-off value is determined using the ROC curve, which is a graph that depicts the trade-off between sensitivity and specificity [19]. Based on Table IV, the cut-off value of Ret-He for detecting ID and IDA in infants aged 1, 2, 3, and 4 months was 22.25 pg, 20.3 pg, 19.05 pg, and 17.55 pg, respectively. In this study, there was no significant difference in the cut-off value of Ret-He in iron-deficient infants compared to IDA infants. The cut-off value of Ret-He at the age of 3–4 months is significantly lower than at the age of 0–2 months. This is similar to Löfving’s study, which found that the cut-off value of Ret-He was significantly lower in infants aged 4 months, namely 25.6 pg compared to 27.4 pg at birth and 28.1 pg at 28–72 h [20]. The lower cut-off Ret-He value indicates that iron deficiency and IDA increase with growth, when there is a change in iron metabolism according to the phase of the physiological development of the baby [4].
To date, no definite cut-off value of Ret-He has been reported for detecting iron deficiency and IDA in infants, especially those under 6 months of age. Ret-He Cut-off values vary. This study is the first one to report the cut-off value and the role of Ret-He for detecting iron deficiency and IDA in infants under 6 months of age in Indonesia. The Ret-He cut-off value for iron deficiency in newborns regardless of gestational age was 25 pg [21]. Ret-He cut-off values for term infants aged 2 days, 4 months, and 12 months were 31.6 pg, 29.2 pg, and 29.0 pg, respectively [22]. In premature and low birth weight (LBW) infants, including LBW (< 1500 g) aged 4 days, the cut-off value of Ret-He was 28.4 pg [22]. Ret-He cut-off values for infants < 34 weeks of gestation and birth weight < 2000 g at birth, 4 weeks of age, 9 weeks of age, 11 weeks of age, and 15 weeks were 31.5 pg, 30.1 pg, 27.5 pg, 26.9, 26.4 pg, respectively [23]. The cut-off value of Ret-He for IDA in infants aged 6–60 months is 23.1 pg [14]. The difference in the cut-off value of Ret-He in this study compared to the studies mentioned above may be due to variations in the characteristics of the study subjects and risk factors that increase the prevalence of iron deficiency.
Tables IV shows the sensitivity, specificity, positive predictive value, and negative predictive value of the Ret-He cut-off in determining ID and IDA for the age categories of 1 month, 2 months, 3 months, and 4 months. Some studies show that Ret-He is excellent for detecting iron deficiency [18, 24–27]. Suari’s study to detect IDA with a Ret-He cut-off value of 23.1 pg at the age of 6–60 months had a sensitivity of 88%, specificity of 25%, positive predictive value of 34%, and negative predictive value of 82% [14]. The Lorenz study to detect iron deficiency with a Ret-He cut-off value of 29 pg in corrected infants aged 3–4 months (< 32 weeks and < 1500 g) had a sensitivity of 85%, specificity of 73%, positive predictive value of 33%, and negative predictive value of 97% [21]. The Torsvik study with a Ret-He cut-off value of 26.9 pg in 4-month-old infants had a sensitivity of 91% and a specificity of 79% [28].
The results of this study are different from several previous studies. First, this study shows high specificity, meaning that the Ret-He examination is suitable for confirming iron deficiency/IDA or detecting that an infant is not sick. Second, a high positive predictive value means that the probability of true iron deficiency/ADB is high if the Ret-He test results are below the cut-off value for age. Low sensitivity means that Ret-He cannot be used for screening tests. This study’s difference in sensitivity, specificity, positive predictive value, and negative predictive value compared to previous studies may be due to variations in the research subjects used (related to gestational age, birth weight, prematurity). In addition, it may also occur due to differences in the cut-off value of Ret-He taken from statistical analysis.
Infants are an age group that is prone to iron deficiency. Early detection and prompt treatment of iron deficiency in this group can prevent complications due to IDA. Ret-He is one of the parameters recommended by the AAP to detect iron deficiency before a decrease in Hb occurs. This test assesses the adequacy of iron in the bone marrow during erythropoiesis [17, 18]. The Ret-He examination is sensitive and specific to detect iron deficiency and IDA [21, 25, 27]. In addition, it is the only marker of red blood cells detected before iron deficiency occurs in the brain [29]. This examination does not require a particular blood sample because the examination has been integrated with the CBC examination with an automated hematology analyzer [18, 25]. This easy, inexpensive examination does not require large blood samples (< 0.5 ml of blood) [13, 21], is available in many health facilities, and is not affected by infectious/inflammatory factors such as other iron parameters (ferritin, SI, TIBC, and TS) [29]. Ret-He examination in infants is also not affected by perinatal stress [21].
Ret-He also correlated well with iron deficiency parameters such as Hb, MCV, MCH, MCHC, SI, TS, ferritin, TIBC, sTfR, reticulocyte count, Mentzer index, RDW index, and erythrocyte protoporphyrin [5, 12, 21, 22, 30]. The diagnostic power of Ret-He for detecting iron deficiency without anemia is higher than that of serum ferritin and Hb (sensitivity 70–94%, specificity 72–80%) [17], and superior to ferritin or the zinc protoporphyrin/heme ratio in neonates [31]. Several studies of Ret-He to detect iron deficiency in infants have shown a sensitivity of 70–94%, specificity of 72–80%, positive predictive value of 33–34%, and negative predictive value of 82–97% [14, 17, 21].
The use of Ret-He in detecting iron deficiency in infants is still limited because there is no definite cut-off value of Ret-He in infants [31]. In addition, there has been no similar research conducted in Indonesia, so the cut-off value of Ret-He in this study can be used as basic health data. Ret-He cut-off values vary according to infant age, birth weight, and prematurity [21–23]. In this study, only Ret-He cut-off assessment was carried out at 1, 2, 3, and 4 months of age, associated with the high prevalence of iron deficiency and IDA at that age in the city of Banjarbaru.
Due to this research being a community-based study that took place during the COVID-19 pandemic, parents are afraid to bring their children for immunization at the Community Health Center for fear of contracting COVID-19. So it is not easy to carry out repeated monthly blood tests on time from 1 month, 2 months, 3 months, and 4 months. Then, the study design allowed the Ret-He cut-off values to be established for overt IDA based on the Ringoringo (2008) criteria in infants. However, the Ret-He cut-off values in infants’ subclinical ID are likely to differ. A further study should be conducted with a prospective cohort design to obtain the Ret-He cut-off of iron deficiency.
Furthermore, this study did not further analyze the birth weight, prematurity, and other risk factors that could influence the incidence of iron deficiency. However, this can be used as an idea for further research.
In conclusion, Ret-He examination can detect ID and IDA in infants aged 1–4 months with high specificity and positive predictive value.