Cardiovascular disease (CVD) is the leading cause of death in the United States (US) and worldwide. Though in the last few decades, overall CVD-related mortality has decreased, CVD-related health disparities among various ethnic groups have widened drastically [1]. Early interventions for the treatment of hypertension are beneficial in preventing CVD and organ damage [2]. Although there are lifestyle modifications and numerous pharmacologic agents that have been proven effective, blood pressure (BP) control rates among African American (AA) patients treated for hypertension remain suboptimal [3].
When looking at hypertension (HTN) rates worldwide, AAs and whites tend to have similar rates [4]. However, when only looking at the US, there is a clear racial disparity. Under the criteria using the 140/90 mm Hg threshold, AAs are noted to have a higher burden of HTN (40.3%) compared to white (27.8%), Asian (25.0%) or Hispanic (27.8%) adults [5]. Compared to whites, AAs have a 30% higher likelihood of dying from CVD [6], are 50% more likely to have a stroke [6], and 70% more likely to die from a stroke [7, 8].
Behavioral lifestyle interventions are essential in controlling HTN and lowering BP levels. HEALS (Healthy Eating and Living Spiritually) Med-Tech is an efficacy-proven faith-based lifestyle program that incorporates interactive technology enhanced HTN control methods [9]. This 12-month program prioritizes HTN management in high-risk AAs presenting at primary care clinics. Further, the program aimed to empower and support the AA community to take steps to obtain better control of their BP [10].
The 12-month HEAL Med-Tech program findings in high-risk AAs with uncontrolled HTN presenting at Norfolk primary care clinics in Virginia (VA) will be presented here.
Methods. Study population. We conducted a randomized controlled trial of peer-facilitated HEALS Med-Tech, a behavioral lifestyle program, compared to the usual care on high-risk AAs with uncontrolled HTN, presenting at a primary clinic in an urban, low-income neighborhood of Norfolk, Virginia (VA). The procedures followed in this study are in accordance with ethical standards for human research and were approved by the Institutional Review Board (IRB) of Eastern Virginia Medical School (EVMS), Norfolk, VA. The urban Norfolk area around EVMS is among the most under-resourced communities of Hampton Roads, reporting some of the most significant HTN-related disparities [11]. The clinic serves over 17,000 patients annually, with six healthcare providers on staff, including physicians, nurse practitioners, and pharmacists. The clinic also houses a Healthy Living Center (HLC), a facility devoted to increasing health awareness and education in the Norfolk community [12]. (Supplementary, Methods).
Statistical analysis. Our previous HEALS studies in AAs suggested that the magnitude of differences in BP change was sufficient to allow estimation of sample size requirements for this study. Based on these considerations, we calculated a sample of 60 participants (n = 30 in each group), which allowed > 80% power with the type-1 error level at 0.5 to detect a difference of approximately 8 mm Hg change in SBP between groups at 3 and 12 months. This assumes a standard deviation (SD) change in SBP at 3 months of 3% based on preliminary data from our previous HEALS study. A conservative attrition rate of up to 20% was assumed. A sample size of 60 participants (n = 30 in each arm) would have 80% power to detect a 10 mm Hg difference in the SBP between treatment arms at 3 and 12 months, assuming a rate of loss-to-follow-up of 15%. All statistical analyses were conducted by the study biostatistician using SAS version 9.4 (SAS Institute, Cary, NC). Descriptive statistics, including mean (with 95% confidence interval), median (with interquartile range), minimum and maximum values, standard deviation (SD), and frequency, were utilized to summarize the data. The Shapiro-Wilk W test [13] was utilized to test the normality of continuous variables. A mixed model for repeated measurements (MMRM) [14] was employed to evaluate changes in both primary (SBP) and secondary (DBP and weight) outcomes.
Results. A total of 68 African American participants were recruited and screened, and consented to the study. Of these, 61 (50 females and 11 males) were randomly assigned to the HEALS Med-Tech intervention or usual care groups (31 and 30 participants, respectively). The mean age was 62.8 ±10.8 years. Most participants had a family history of heart disease (90%), and many had a history of cardiovascular disease (89%) and diabetes (26.5%). 66% of participants had completed high school and 36% were college graduates (Supplemntary Table SII).
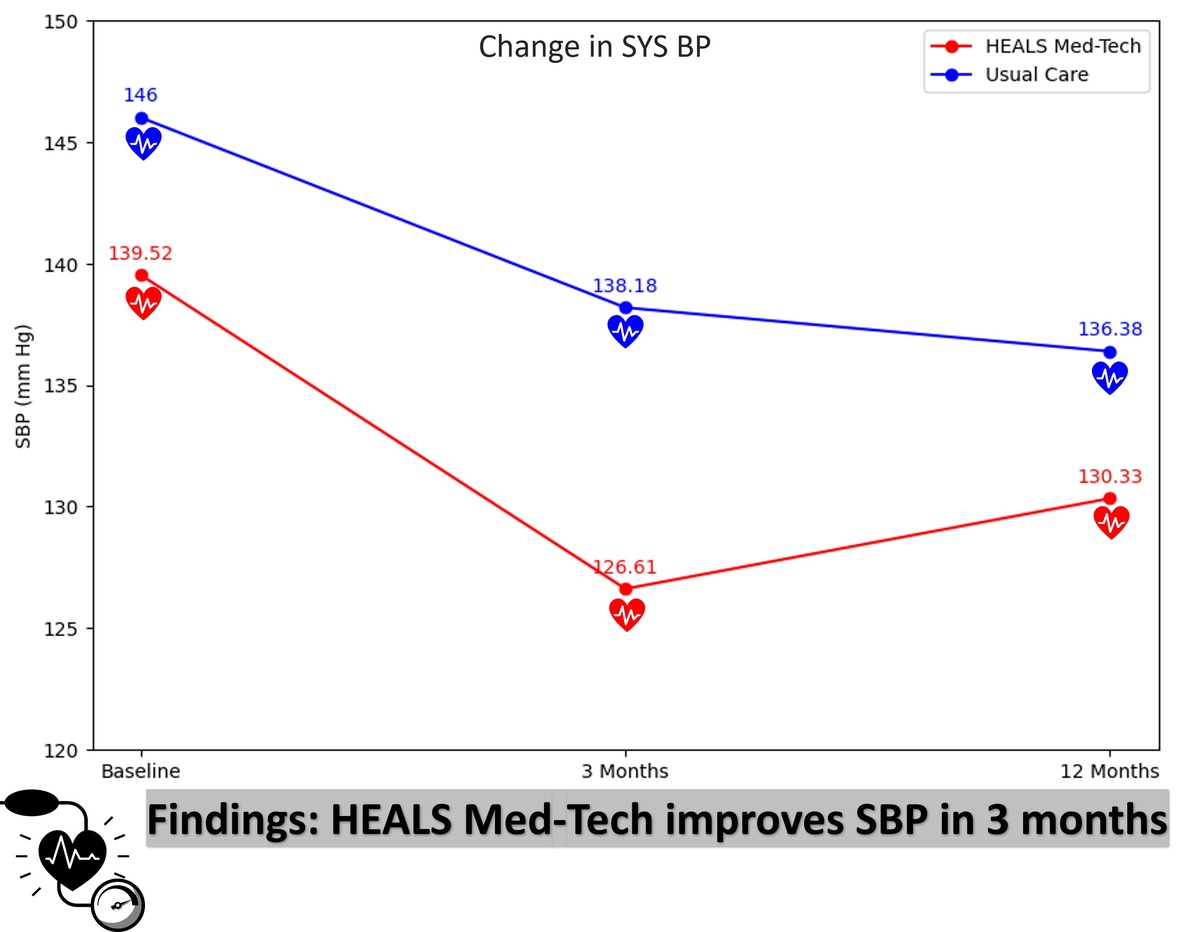
The HEALS Med-Tech group showed a greater reduction in SBP and DBP compared to the usual care group at the end of the first 3 months of the intervention. Specifically, the HEALS Med-Tech group showed a decrease in SBP by 12.95 mm Hg compared to 7.82 mm Hg in the usual care group (p = 0.008, Supplementary Figure S3) from the baseline. Similarly, the HEALS Med-Tech group showed a decrease in DBP by 4.34 mm Hg, compared to 0.36 mm Hg in the usual care group (p = 0.034, Supplementary Figure S4) from the baseline. Moreover, the HEALS Med-Tech group had borderline blood pressure values at the start of the study. This can influence the extent to which their blood pressure may be reduced by the intervention, as they are starting from a lower baseline. The control group had higher systolic blood pressure values at baseline, although not statistically significant (p = 0.089). The p-value indicates that there is a 8.9% probability that the observed difference occurred by chance alone, which is insufficient to claim a significant difference. The higher baseline systolic blood pressure may also be indicative of the diversity in our participant pool and opens a conversation on individualized treatment approaches.
Additionally, the HEALS Med-Tech group showed a significant reduction in SBP of 9.19 mm Hg at 1 year (p = 0.013). However, the reduction in DBP in the HEALS Med-Tech group of 1.67 mm Hg was not statistically significant (p = 0.406). Further, within the HEALS Med-Tech group, the SBP reductions were sustained, but when compared with the usual care arm, there was no statistically significant difference in SBP at 1 year (p = 0.193). Despite the HEALS Med-Tech group having numerically lower blood pressures at the end, the differences were not statistically significant (p = 0.193 for systolic, p = 0.3 for diastolic). This suggests that while there might be a numerical difference, we cannot confidently attribute this to the intervention due to the high p-values. Similarly, no changes in weight within and between the two groups were seen at 3 and 12 months of the study (Supplementary Figure S5).
Discussion. This study demonstrated that a behavioral lifestyle intervention program led by peer facilitators combined with a telehealth approach is effective in significantly reducing SBP over a 1-year period compared to the usual care arm, further fostering the acceptability of behavior change interventions among marginalized AAs. Previous behavioral change studies aimed to reduce hypertension among African American populations through community-focused programs or technology-based interventions. However, most of these studies have not combined both aspects into one intervention like the HEALS-Med Tech study. Furthermore, most of these studies have not shown sustained effects beyond 9 months.
The FAITH study, which used faith-based therapeutic lifestyle changes (TLC) delivered by lay health advisors in black churches, found that the intervention group had a significantly greater SBP reduction compared to the control group at 6 months [15]. Like HEALS Med-Tech, this study primarily focused on delivering HTN control healthcare with the use of lay people. However, the FAITH study did not include any form of technology as a major component of its intervention.
A technology-based HTN program was evaluated by Still et al. and did not prove to be effective in reducing blood pressure in both groups [16]. This study highlights that technological approaches alone are not effective in reducing hypertension. The HEALS Med-Tech program shows that a combination of a behavioral lifestyle intervention and telehealth approaches can effectively reduce blood pressure.
A mixed methods pilot study assessing a clinical pharmacist-led mobile health-based approach to manage uncontrolled hypertensive patients via real-time monitoring over 12 weeks proved to be effective [17]. Like HEALS Med-Tech, this study focuses on bidirectional intervention and supports both home blood pressure monitoring and medication adherence for patients with uncontrolled hypertension; however, HEALS Med-Tech shows the need for guidance from CHAs, which provides additional behavioral and emotional support.
The HEALS Med-Tech program offers a unique and innovative approach to addressing HTN control and prevention in AA communities by combining a culturally tailored, group-based lifestyle intervention led by trained lay health counselors with a telehealth program. The results of this study demonstrated that the HEALS Med-Tech intervention was effective in significantly reducing SBP after 1 year, showing the potential acceptability of behavior change interventions among marginalized AAs.