Introduction
Globally, anaemia affects a population exceeding 1.9 billion individuals, resulting in a substantial health burden, including 52 million years lived with disability (YLDs). This condition accounted for 5.7% of all YLDs in 2021 [1]. Between 1990 and 2021, there was a notable disparity between reductions in YLDs due to anaemia and changes in its prevalence [2]. This discrepancy indicates a worldwide trend towards less severe cases of anaemia. However, progress in addressing anaemia has been notably inconsistent and rather slow [1].
According to the World Health Organization (WHO), in 2019 anaemia in children, defined as a decrease in haemoglobin levels to below 110 g/l (adjusted for altitude) [3], significantly contributed to the overall prevalence of chronic illness worldwide. In recent decades, anaemia has emerged as a prominent contributor to the burden of disability-adjusted life years (DALYs) among children under the age of 5 [4, 5].
Anaemia in children is associated with reduced cognitive and motor development as well as susceptibility to infections. This susceptibility to infections [6] – particularly severe ones, such as malaria – may increase the risk of mortality during children [7, 8]. Dietary iron deficiency is considered the primary cause of anaemia in children below the age of 5. However, haemoglobinopathies and other infectious diseases, such as HIV/AIDS and malaria, also play a significant role as contributing factors in regions where these conditions are prevalent [2].
Despite the complexity of the underlying causes of anaemia, most reduction efforts have concentrated mainly on iron delivery [9, 10]. Thus, it should come as no surprise that progress in decreasing the global anaemia burden has been slow and insufficient [2, 11].
There has been a notable increase in awareness regarding anaemia and its implications for the health and developmental outcomes of children over the past decade. In 2012, the 65th World Health Assembly [1] endorsed a set of six worldwide targets for maternal, infant, and young child nutrition, with the aim of achieving them by the year 2025. The first target is to reduce the global prevalence of stunting in children under the age of 5 by 40% [12]. The WHO and the United Nations Children’s Fund have suggested prolonging this target until 2030 in order to synchronise it with the United Nations’ Sustainable Development Goals (SDGs) [13]. However, little is known about the global progress made towards reducing anaemia in children since the SDGs were introduced.
Several studies have examined the prevalence of anaemia in children under the age of 5. However, these studies either relied on outdated data or did not focus on specific groups or geographical areas [14–16]. Limited research has attempted to provide up-to-date estimates of the global anaemia burden [1, 2].
Our objective was to examine the prevalence of anaemia in children aged 6–59 months from 2000 to 2019 on a global scale using WHO data. We further examined changes in its prevalence from 2000 to 2019. We analysed these data and stratified them by the present (2022) income levels of the studied countries. Overall, we attempted to comprehensively assess the complete magnitude of the prevalence of anaemia among children aged 6–59 months.
Material and methods
We analysed population-representative data from 189 countries and territories across all 6 WHO regions to estimate trends in anaemia prevalence among children aged 6–59 months from 2000 to 2019. The data were collected from the WHO’s Information System Database.
Inclusion criteria
We included data on anaemia prevalence if they were publicly available on the WHO’s website, if comprehensive data were provided for the period 2000–2019, and if the website included categorisations of each country’s income earned in 2022.
Data source
The data on anaemia prevalence that we consulted are publicly available on the WHO’s website (https://www.who.int/data/gho/data/indicators/indicator-details/GHO/prevalence-of-anaemia-in-children-under-5-years-(-)). The country income classification is publicly available on the World Bank’s website (https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups).
Analytical phase
Our analysis included four steps. The first phase included finding, evaluating, and obtaining data on the prevalence of anaemia. The second phase involved correlating this prevalence with each country’s income based on its categorisation by the World Bank as of 2022. The countries were classified into income groups based on their 2022 gross national income per capita as determined using the World Bank’s Atlas technique. The categories are as follows: low income: $1,045 or less; lower middle income: $1,046 to $4,095; higher middle income: $4,096 to $12,695; and high income: $12,696 or above.
The third phase entailed assessing trends in anaemia prevalence over a 20-year period (2000–2019) at 5-year intervals (2000–2005, 2005–2010, 2010–2015, and 2015–2019) and comparing these trends with the income levels of the selected countries. Adopting a descriptive statistical method, we tested the assumptions of normality of variances using the Kolmogorov-Smirnov and Shapiro-Wilk tests. The Kruskal-Wallis test was used to analyse the associations between anaemia prevalence and income category. The fourth phase involved assessing the changes in anaemia prevalence from 2000 to 2019. We calculated the changes at 5-year intervals and compared the intervals based on the relative changes therein.
In this study, a small decrease in anaemia prevalence was defined as a relative decline of less than 3% over the two decades. A large decrease in anaemia prevalence is understood as a relative decline of more than 10% during the study period. We used Microsoft Excel and Graph Pad Prism for Windows (version 5.0, San Diego, CA; www.graphpad.com, SCR_002798). Additionally, to identify relevant research on our topic, we conducted a comprehensive search of the scientific databases Embase, IMEMR (EMRO), IndMED, Medline, and Web of Science for studies published between January 1, 2000, and September 1, 2023.
Results
Our analysis covered 189 countries. We used WHO data from the 6 regions distinguished by this organisation: Africa, the Americas, the Eastern Mediterranean, Europe, Southeast Asia, and the Western Pacific – to analyse the changes in anaemia prevalence among children aged 6–59 months between 2000 and 2019.
Prevalence of anaemia
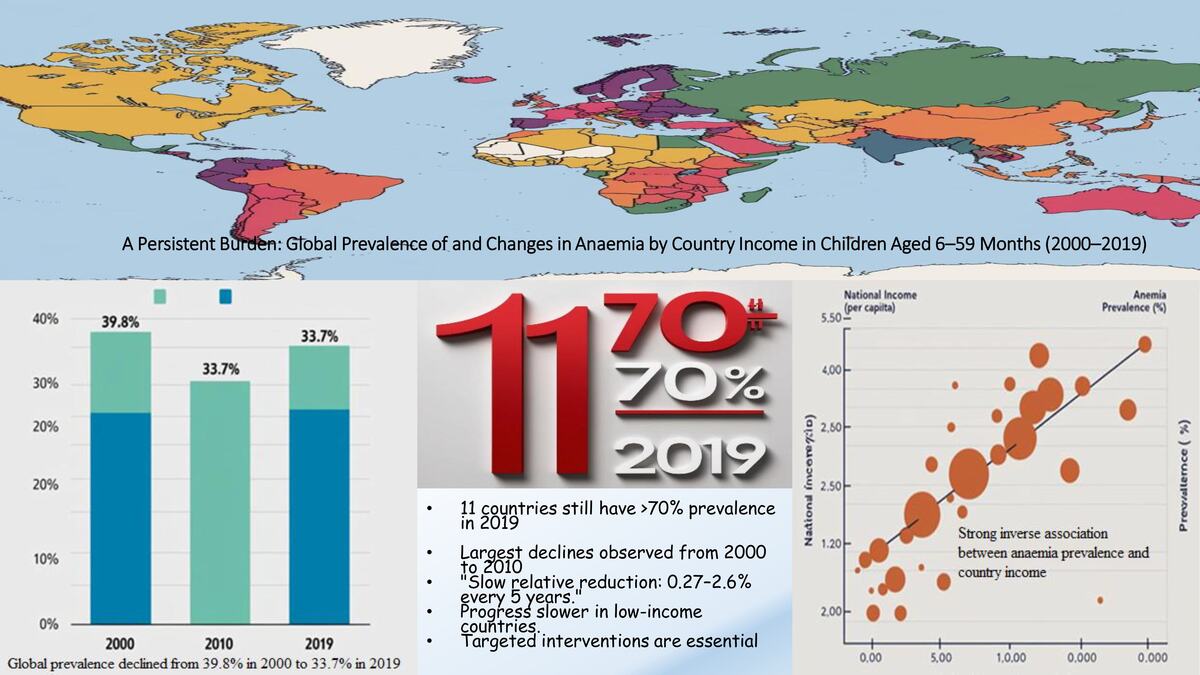
Anaemia prevalence differed across geographic regions, with the highest incidences observed in Africa and Southern Asia (Table I). In 2000, the prevalence of anaemia in children exceeded 80% in 9 countries in Western and Central Africa and Yemen. The prevalence exceeded 70% in an additional 19 countries in Eastern, Western, and Central Africa. By 2019, no country had a prevalence higher than 80%, but the prevalence exceeded 70% in 11 countries (Yemen and 10 countries in Western and Central Africa). At the other extreme, the prevalence in the USA lingered around 6% from 2000 to 2019.
Table I
Prevalence of anaemia in children aged 5–59 months across continents from 2000 to 2019
Correlating prevalence with country income
According to the World Bank’s data, 86% of the countries in Africa and 73% of the nations in Southern Asia, where anaemia prevalence was high, have low or lower middle incomes. In contrast, the lowest occurrences were reported in the Americas and Europe, where most countries (between 88% and 92%) have high or upper middle incomes. In general, 42% of countries worldwide have a per capita income below $4,255, placing them in the low- to middle-income category, which has an impact on the health of their residents (Table II).
Table II
Income distribution among continents
[i] Economies by county income from the World Bank classification for the fiscal year 2022 distributed around the continents. Gross national income (GNI) per capita less than or equal to $1045 is considered low income; GNI per capita between $1046 and $4095 is considered lower middle income; GNI per capita between $4096 and $12,695 is considered upper middle income; and GNI per capita of $12,696 or more is considered high income. Each column’s numbers correspond to a country’s income.
Our analysis revealed a highly significant correlation between prevalence of anaemia and country income (p < 0.001). This significance was persistent throughout the study period (2000–2019) and within each 5-year interval (Table III). The high-income group had a low anaemia prevalence, and conversely, the low-income group had a high prevalence. The highest incidences of anaemia were observed in Africa and Southern Asia.
Table III
Analysis of anaemia prevalence in children by income group across different periods using Kruskal-Wallis H test
Trends in anaemia prevalence from 2000 to 2019
Over the 20 years examined, the prevalence of anaemia in children under 5 years of age decreased in most countries, especially between 2000 and 2010. European nations exhibited a smaller decline in anaemia rates compared to Africa and the Americas, where there was a more pronounced fall in its prevalence (Figure 1). In 2000, Africa had the highest frequency of anaemia among children at 67.6%, but this continent achieved a decline of over 10% by 2019.
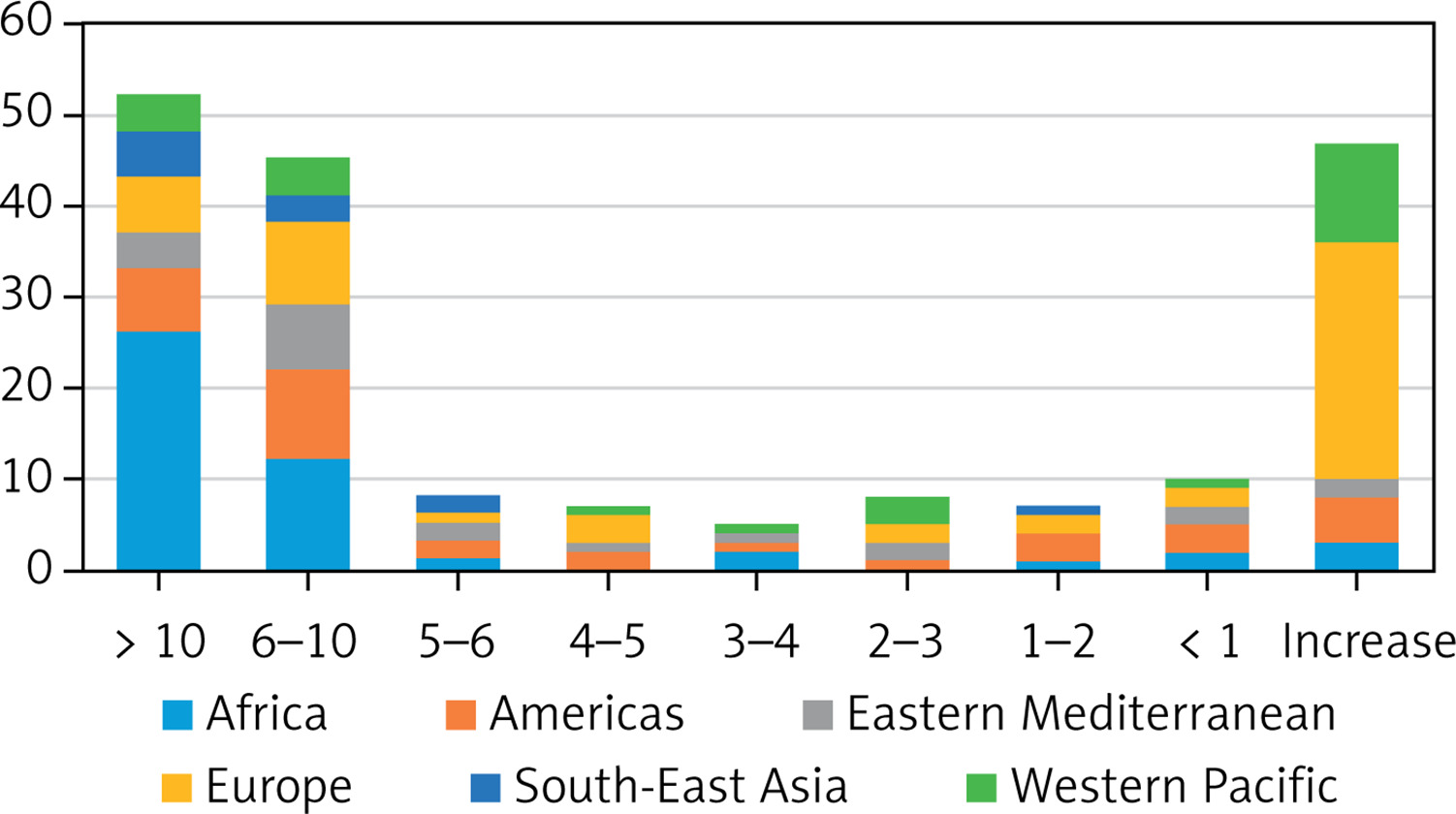
Figure 1
Variation in anaemia prevalence in children aged 5–59 months among continents in 19 years (2000–2019). The abscissa axis represents the percentage of decrease/increase in anaemia (%), while the ordinate axis shows how many countries attained each trend over a study period
Furthermore, in Africa, there was a notable decrease in anaemia among children between 2000 and 2010. From 2000 to 2005, 74% of the countries on this continent experienced a fall of at least 2%, while from 2005 to 2010, this number increased to 81%. Between 2000 and 2005, 15 African nations (32% of the continent) experienced a ≥ 5% decrease in the prevalence of anaemia among children aged 6–59 months.
Of the 10 nations in Southern Asia, 91% experienced a decrease of at least 3% between 2000 and 2005. In the Americas, there was a reduction of just over 2% in approximately 47% of countries from 2005 to 2010 and from 2010 to 2015. In the Mediterranean region, 40.9% of children had anaemia in 2000, and this prevalence dropped by 6.2% by 2019. In the Pacific countries, the decline in prevalence among this age group was more than 2%, with rates of 20%, 24%, and 28% from 2000 to 2005, 2005 to 2010, and 2010 to 2015, respectively.
Changes in anaemia prevalence from 2000 to 2019
Disparities in anaemia prevalence were more pronounced at the country level. Out of 189 countries, 61 reported a prevalence of more than 40% in children. In no country was the prevalence of anaemia less than 5% in 2019 (Table I). By 2019, Mali had the highest prevalence in Africa, at 79%, while Seychelles had the lowest, at 30.6%. In the Americas, Haiti had the highest prevalence, at 60.1%, while the United States had the lowest, at 6.1%. In the Eastern Mediterranean, Yemen had the highest prevalence, at 79.5%, while Kuwait had the lowest, at 19.8%. In Europe, Tajikistan had the highest prevalence, at 37%, while Iceland had the lowest, at 11%. In Southeast Asia, India had the highest prevalence, at 53.4%, while Thailand had the lowest, at 24.9%. In the Western Pacific, Kiribati had the highest prevalence, at 49.4%, while Australia had the lowest, at 13.3%.
In 2019, 11 countries reported the highest level of anaemia in children, defined as a prevalence of greater than 70%, whereas the 2 countries with the lowest burdens (Guatemala and the United States) had prevalence of less than 10%. Malaysia suffered the most significant increase, as its prevalence in 2019 was almost 4.4% higher than in 2000. The prevalence of anaemia among children increased in 7 countries.
Based on our analysis of the WHO’s dataset, 9 nations experienced a small decrease by 2010, followed by a slight increase up to 2019 (Figure 2). On the other hand, 10 nations experienced a notable decrease followed by a notable increase, resulting in a return to levels that were worse than or similar to those reported between 2000 and 2005 (Figure 3). Our findings indicate that 75% (142/189) of all nations and 92.4% (72/80) of low- and middle-income countries (LMICs) saw a decline in the average prevalence of anaemia. Globally, the prevalence declined from 39.8% to 33.7% between 2000 and 2019 (Table II).
Figure 2
Fluctuation in prevalence of anaemia among children aged 5–59 months in countries that experienced a small decrease until 2010, followed by a slight increase up to 2019
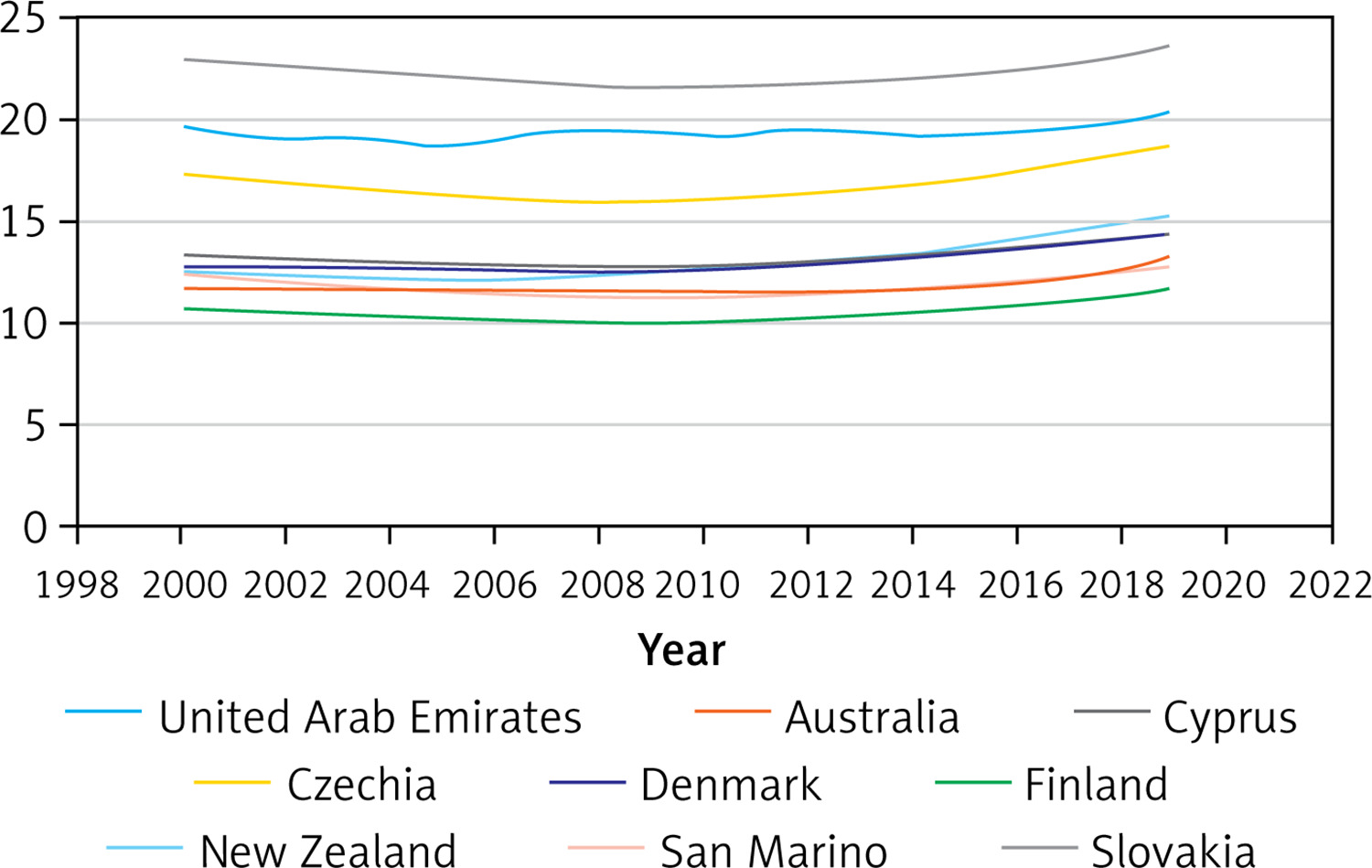
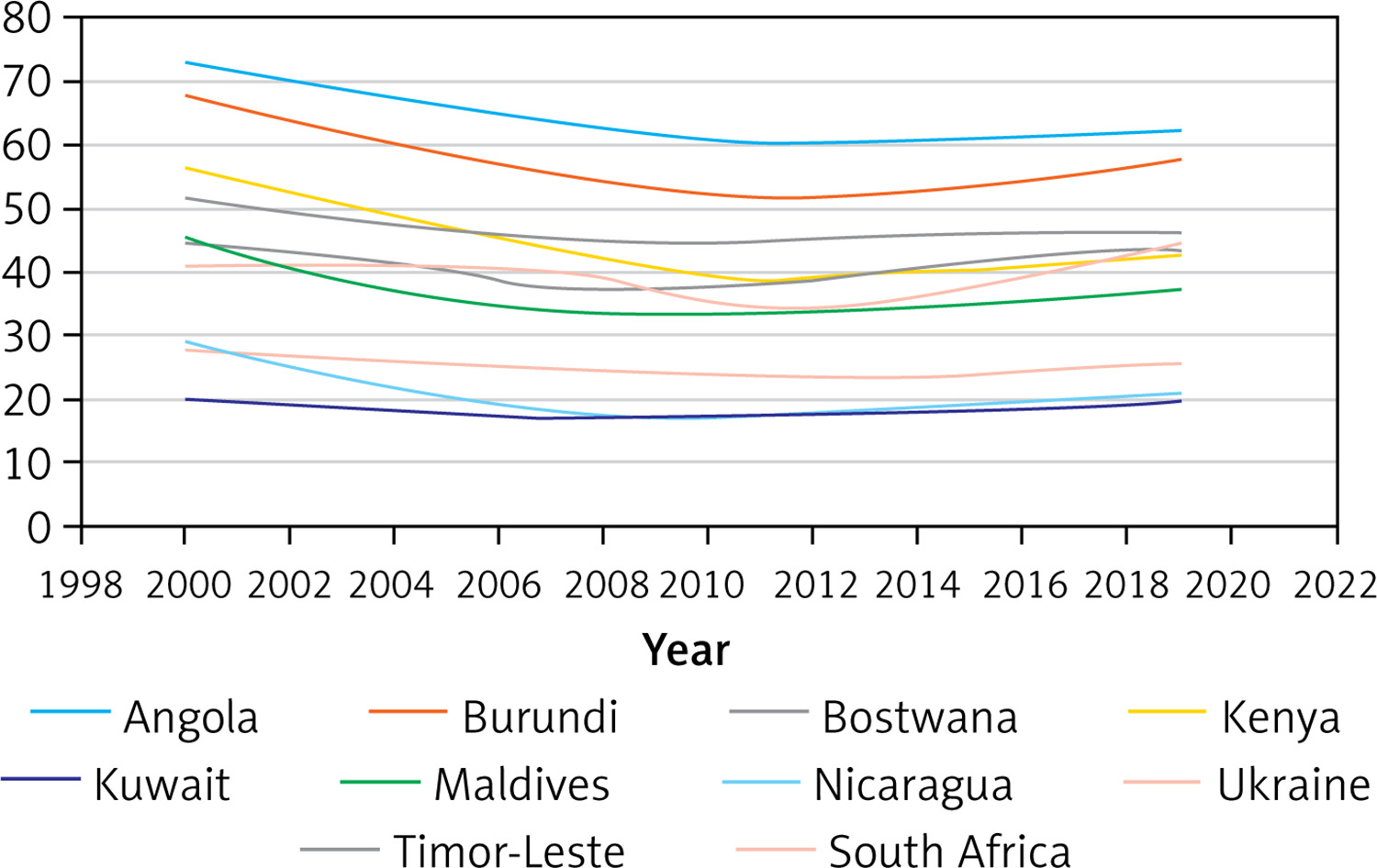
Figure 3
Fluctuation in prevalence of anaemia among children aged 5–59 months in countries that experienced a notable decrease followed by a notable increase from 2000 to 2019
Relative reductions in total anaemia prevalence in children have been slow, with worldwide average reductions of around 0.27–2.6% every 5 years since 2000. The declines in anaemia prevalence were larger in the period 2000–2010 than in 2010–2019. Southeast Asia and Africa had the largest relative declines. In the study period, the highest level of anaemia reduction (relative reductions of 10%–27%) was observed in 52 countries.
Discussion
In this study, we examined changes in the prevalence of anaemia in children aged 6–59 months in 189 countries from 2000 to 2019. We found that the average prevalence declined in 75% (142/189) of all countries and in 92.4% (72/80) of LMICs during this period. Globally, the prevalence of paediatric anaemia declined from 39.8% to 33.7% from 2000 to 2019. However, relative reductions in total prevalence in this age group have been slow, with average declines worldwide of around 0.27–2.6% every 5 years since 2000. This slow reduction points to challenges and serious public health problems, especially in low-income counties.
This study’s findings are consistent with those of prior research, indicating that, while anaemia rates have improved modestly, the progress is steady. This improvement can be attributed to the establishment of healthcare programmes, nutritional programmes based on food fortification, and general public health interventions [17–21]. Nations that have implemented enriched dietary programmes combined with increased access to health services and micronutritional supplements have achieved significant drops in anaemia prevalence. For example, research shows that the implementation of food fortification and iron supplement programmes in Sub-Saharan Africa [22–24] and Southeast Asia [25–27] resulted in a significant decrease in anaemia prevalence, particularly in the early 2000s, which is consistent with our findings.
Many studies, including ours, have found that the global decline in anaemia incidence varies by region. For example, a study by the World Bank found that while anaemia prevalence has declined globally, the rate of reduction varies by region, and the decline is less significant among children under the age of 5 years [2, 28, 29]. These observations demonstrate that a diversity of factors influence the occurrence of anaemia, indicating the importance of implementing targeted interventions. These interventions should be tailored to the local anaemia burden and the country’s conditions.
Although the prevalence in some countries decreased consistently over the study period, others exhibited a subsequent increase, particularly after 2010. Examples of this trend can be found in Malaysia, France, and the Netherlands. This increase in anaemia prevalence could be attributed to socioeconomic instability or economic changes that affect healthcare funding and access, maternal anaemia [30], and changes in nutritional habits [31]. Changes in anaemia prevalence require additional research at the national or regional level to investigate more closely what local factors influence these changes and how they do so.
In LMICs, particularly in Africa and Southeast Asia, insufficient access to healthcare facilities and an unstable food supply contribute to anaemia’s high incidence. These regions have experienced challenges in ensuring a consistent food supply, which could lead to a lack of critical nutritional elements, such as iron, folic acid, and vitamin B12 [1, 2, 32, 33]. Furthermore, the high prevalence of infectious diseases, such as endemic schistosomiasis, contributes to the increased prevalence of anaemia in these regions [34, 35]. Sickle cell disease is prevalent among children in Sub-Saharan Africa and Asia [36, 37]. Thus, addressing schistosomiasis and sickle cell disease could be the primary focus of efforts to reduce anaemia in these areas. In Sub-Saharan Africa, HIV/AIDS was the second leading cause of YLDs due to anaemia during the study period. Anaemia caused by malaria was most prevalent in the central, eastern, and western areas of Sub-Saharan Africa, ranking as the second or third leading cause of the YLD burden in each of these regions [1].
Our findings are consistent with those of previous research, which has reported a high prevalence of anaemia in LMICs, indicating a strong association between anaemia prevalence and income level [19, 38]. Anaemia can result from nutrition-specific factors, such as inadequate intake or poor absorption of micronutrients; non-nutritional factors; or a mix of both, with each influenced by socioeconomic determinants [38]. In children under 5 years old, dietary iron deficiency is the primary cause of anaemia. However, haemoglobinopathies, various infectious conditions, and malaria all play significant roles in areas where these diseases are common [39, 40]. Population-based interventions to reduce and treat paediatric anaemia should consider infectious conditions in both the community and the individual.
Reducing the prevalence of anaemia is critical in promoting children’s health. Despite reported improvements, this prevalence remains high in the world’s poorest countries, posing a challenge to healthy early childhood development and diminishing academic performance [38, 41]. Comprehensive data on trends in each determinant would be necessary to determine the impact of nutritional and non-nutritional factors on regional variations in anaemia. Population-based data on micronutrient deficiencies are especially needed, as the lack of such information hinders our ability to accurately determine national and regional trends in the prevalence of these deficiencies [42].
To further decrease the prevalence of anaemia, a mix of programmes targeting the viral and dietary factors that contribute to low haemoglobin levels is necessary. To effectively address anaemia in all its variants, it is essential to have a thorough understanding of the distinct factors that contribute to anaemia in specific locations, including at the sub-national level. The WHO and other entities have provided detailed plans for controlling anaemia, including key recommendations and suggestions [43, 44].
Our analysis indicates a high frequency of anaemia in children globally, which is consistent with prior estimates [2, 45]. However, prior assessments of anaemia prevalence in children under 5 years of age have yielded higher rates than ours. These variations can be partially attributed to the inclusion of district data in the World Bank dataset, which offers a more comprehensive perspective. Our findings also confirm prior research that has revealed a global decline in anaemia prevalence among children [2, 16, 45]. Nevertheless, numerous countries, especially those categorised as LMICs, still exhibit a high frequency of anaemia.
This study’s main strengths include its use of comprehensive data from the WHO, which cover 20 years across 189 nations; the analysis of estimated trends in anaemia prevalence estimates by country and region; and the focus on children aged 6–59 months, which enabled a more detailed analysis.
Implications.
Some progress has been made in reducing the prevalence of anaemia. However, there are major gaps in our knowledge of the global situation and in the data on what changes are needed. Overall, anaemia among children aged 6–59 months remains a problem worldwide. Our analysis confirms that the prevalence of anaemia in this age group is a significant public health concern. Moreover, our findings point to a slow decline in prevalence among this age group. Sustained public health efforts are necessary to reduce anaemia prevalence, and such efforts should target countries with high prevalence.
Limitations.
Although this study offers useful insights regarding the prevalence of anaemia reduction in children, it has limitations. Our analysis mainly relied on existing WHO data. Data collected from different locations and countries may differ in terms of accuracy and completeness. This could produce bias in the final outcomes. WHO data are collected at the national level and lack individual information (e.g. on height, weight, body mass index, educational level, and other demographic factors). Additionally, data on serum ferritin, soluble transferrin receptors, and transferrin saturation were unavailable, and information on malaria, inflammation, infection, sickle cell disease, haemoglobinopathies, and other causes of anaemia was not investigated.
In conclusion, our analysis shows that the prevalence of anaemia in children aged 6–59 months has declined globally. However, relative reductions in total anaemia prevalence have been slow. We found a strong association between the prevalence of anaemia and country income. This prevalence remains high in LMICs. This confirms that the prevalence of anaemia in children is indeed a significant public health concern. Income-based interventions to counter paediatric anaemia should be considered, and further research is required to gain a deeper understanding of its precise causes.