Introduction
It is estimated that 20–40% of children experience some feeding difficulties [1, 2]. These problems are typically recognized in patients between 4 months and 6 years old [3]. Some children might experience feeding or eating difficulties due to motor problems [4]. Feeding difficulties are defined as patterns of oral consumption of solids and/or liquids which differ from the accepted norms. Feeding difficulty can manifest as partial or total food refusal, food selectivity (picky/fussy eating), food neophobia, and/or feeding disorders [2, 5, 6]. It is an umbrella term encompassing all feeding problems, regardless of etiology or severity [2]. There exist several classifications of etiology of feeding difficulties, but none of them are perfect [7]. Feeding difficulty can be categorized as one of the three following factors: organic (medical), nonorganic (behavioral), and mixed (coexistence of organic and nonorganic factors) [8–11]. The results of published studies indicate that the majority of feeding problems are related to mixed causes [10, 11], although the data about etiological factors are still limited.
During the first years of a child’s life it is crucial to maintain a well-balanced diet in terms of quantity (energy) and quality (proper delivery of macronutrients, vitamins and trace elements). It ensures optimal growth and development of the child, and according to the theory of nutritional programming, simultaneously can determine the state of the health during adulthood [12]. Notably, feeding difficulties experienced by a child might lead to impairment of the nutritional status [2, 12, 13].
Our study aimed to assess etiological factors and nutritional status in children with feeding difficulties admitted to the multidisciplinary nutritional team.
Material and methods
Design and study setting
A cross-sectional study was conducted. Participants were recruited from among children admitted to the tertiary referral center for the assessment of feeding difficulties from September 2013 to April 2019.
Study population
Children with feeding difficulties who were admitted to the Department of Pediatrics were enrolled in the study. Feeding difficulties included feeding disorders (F98.2; ICD-10-CM)/avoidant-restrictive food intake disorder (ARFID; 307.59; F50.89, ICD-11) and food selectivity (picky/fussy eating)/avoidant or restrictive eating (MB29.0; ICD-11). Feeding difficulties were diagnosed based on criteria defined in ICD-11. They were diagnosed by a minimum of two specialists via clinical interviews, in vivo observations of the mealtime, and analysis of video materials recorded at home during mealtimes.
Data collection
Part of the multidisciplinary nutritional team (psychologist, gastroenterologist and pediatrician) analyzed the patient’s medical records and feeding history in order to categorized the cause of feeding difficulty as nonorganic, organic or mixed. If feeding difficulties were determined to be related to a medical condition, they were classified as organic [14]. When no medical problems were identified, then the feeding difficulty was categorized as being of nonorganic etiology [14]. Mixed etiologies were identified when there was coexistence of organic and nonorganic factors [15]. Nutritional status was assessed using anthropometric measurements (weight, length/ height) according to WHO protocols [16, 17]. Weight was measured with an electronic scale (Radwag WPT 6/15D or Radwag 60/150W). Length in children < 2 years was measured with infantometer (Seca 416). Height (> 2 years) was measured using a stadiometer (Seca 213).
Data analysis
Data were analyzed using IBM SPSS Statistics (version 24). Descriptive statistics were used to present the study population characteristics. Child’s weight, length/height and body mass index (BMI) were converted into the standard deviation scores (z-scores) using the WHO Anthro (0–5 years) and WHO AnthroPlus (5–19 years) software [18, 19]. The data were interpreted based on WHO Global Database on Child Growth and Malnutrition recommendations [20, 21]. Underweight was defined as weight for age < –2 standard deviations (SD) of the WHO Child Growth Standards median, stunted growth as height for age < –2 SD of the WHO Child Growth Standards median, wasting as BMI < –2 SD of the WHO Child Growth Standards median, and overweight: weight for height > +2 SD of the WHO Child Growth Standards median [21].
Results
The data of four hundred and twenty-two children, referred to the hospital-based multidisciplinary feeding difficulties clinic in September 2013 – April 2019 in Warsaw, were analyzed. Characteristics of recruited population are included in Table I.
Table I
Characteristics of children with feeding difficulties
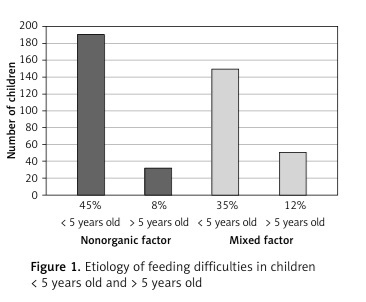
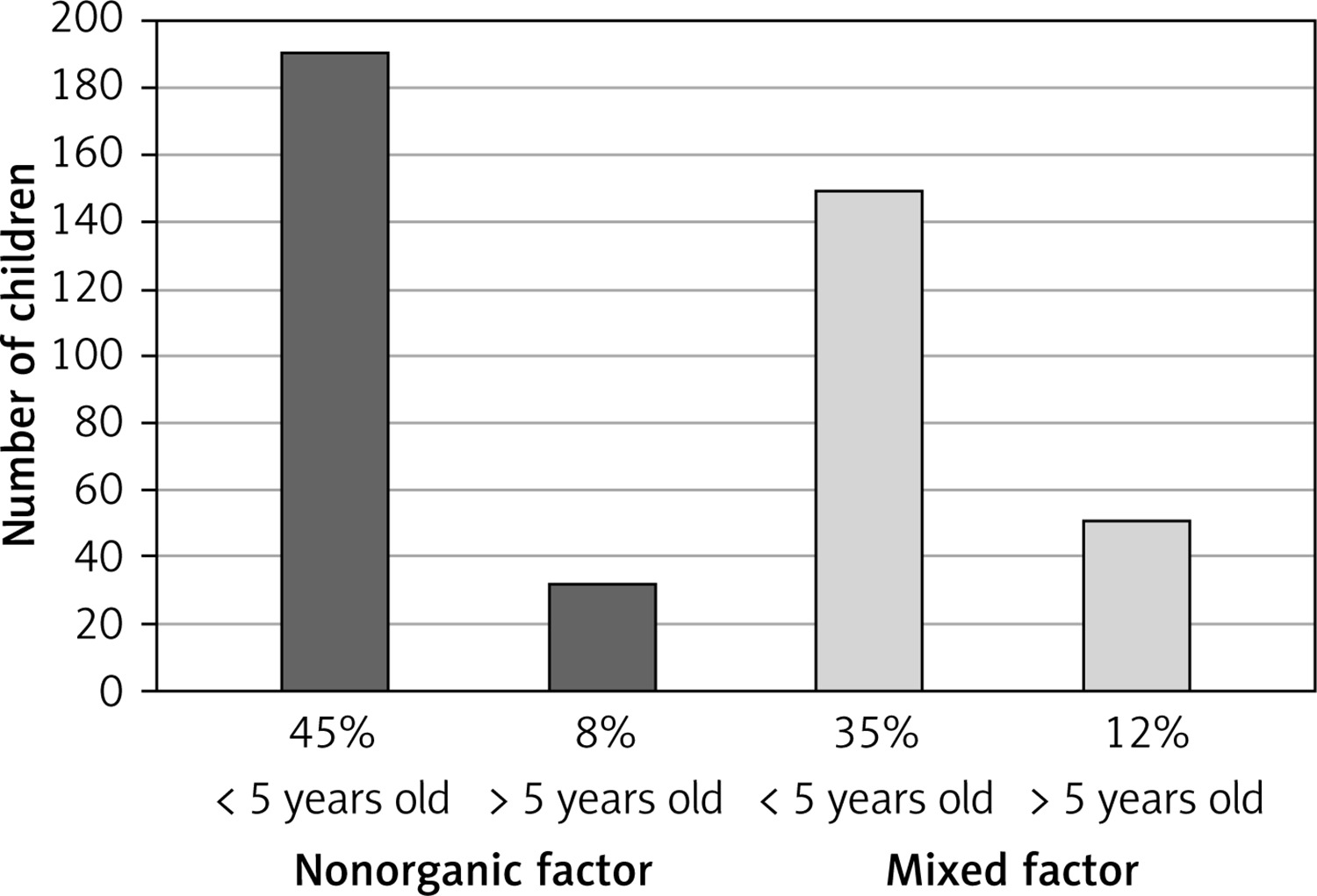
The analyzed data showed that in 222 patients (53%) feeding difficulties were related to behavioral factors only, whereas 200 patients (47%) were affected by mixed factors: organic and behavioral. The most frequent organic causes related to the feeding difficulties were gastroenterological disorders (19.19%), allergy (9.24%), cardio-respiratory problems (2.37%), neurological problems (1.89%), nephrological problems (1.42%), genetic disorders (1.42%), endocrine problems (0.95%), and laryngological problems (0.48%). More than one medical problem was reported by 44 patients (10.43%). Thirty-one patients were diagnosed with autism spectrum disorder, whereas 15 of those patients displayed feeding difficulties due to medical components such as allergy or gastroenterological disorders.
Most patients (n = 339) with feeding difficulties were between 0 and 5 years old. Only 83 patients were older than 5 years (Figure 1).
Underweight (weight < –2 z-score) was observed in 72 patients (17.60%), stunted growth (length/height < –2 z-score) in 45 (10.66%), wasting (BMI < –2 z-score) in 63 (14.93%), and overweight (BMI > + 2 z-score) in 5 (1.18%). Both underweight and stunted growth were observed in 18 patients (4.27%), underweight and wasting in 26 patients (6.16%), stunted growth and wasting in 1 (0.24%). Underweight, stunted growth and wasting were observed in 5 patients (1.18%). Additionally, 5 patients were fed enterally during admission to the feeding clinic.
A summary of data on the nutritional status of both groups (organic and mixed) is presented in Table II.
Table II
Nutritional status in the pediatric population with feeding difficulties
| Child’s age | Nonorganic factor | Mixed factor | ||||||
|---|---|---|---|---|---|---|---|---|
| Underweight | Stunted growth | Wasting | Overweight | Underweight | Stunted growth | Wasting | Overweight | |
| < 5 years old, n | 36 | 22 | 32 | 2 | 26 | 18 | 27 | 1 |
| > 5 years old, n | 5 | 2 | 4 | 0 | 5 | 3 | 0 | 2 |
There were no differences in means of z-score for weight, length/high and BMI between nonorganic and mixed causes. Anthropometric parameters (z-scores) for each factor are presented in Table III.
Table III
Anthropometric parameters (z-scores) for nonorganic vs. mixed factors of feeding difficulties
Discussion
The results of the current study showed that approximately half of the patients had isolated nonorganic feeding difficulties. The remaining children exhibited feeding problems due to mixed factors. Our results differ slightly from other published research [8, 10, 11]. We observed a higher proportion (52%) of patients with isolated nonorganic feeding difficulties. In studies by Burklow et al. [11] and Budd et al. [10], nonorganic factors were observed in 12% and 10% of children respectively. We were unable to identify children with isolated organic factors, whereas other studies found that 15–26% of children had organic feeding difficulties [10, 11]. This difference might be related to the fact that the current study was conducted in a tertiary referral center for the assessment of feeding difficulties. A majority of those patients were already diagnosed with feeding difficulties where organic factors had been ruled out or treated. Similarly to other publications, we found mixed etiology in a substantial proportion of patients [8, 10, 11]. Those results may suggest that medical symptoms are accompanied by behavioral food refusal, developed at a later point due to unpleasant experiences with feeding/eating during illness.
Problematic behaviors occurring during the mealtime may be maintained by environmental factors [22, 23]. In order to overcome a child’s feeding difficulties, caregivers may try various strategies which reinforce those problems. Problematic behaviors would be maintained by negative and/or positive reinforcement. The mealtime context during the child’s illness might be associated with pain or aversive experience, which may lead to engaging in food refusal and inappropriate behaviors (e.g. tantrums, pushing away spoon). Termination of the mealtime might be one of the responses of parents/caregivers [23]. A child learns that inappropriate mealtime behaviors produce escape from eating. A mealtime termination as a negative reinforcement of feeding problems results in increasingly inappropriate mealtime behavior in the future. Additionally, a child might engage in inappropriate mealtime behavior when it leads to access to tangibles, including highly preferred activities such as toys, movies, or attention. Continuation of that kind of dealing with problematic behaviors might increase them even more in the future. In this context, the positive reinforcement also maintains refusal behaviors [22, 24]. It should be added that from the parent/caregiver perspective stopping the child’s inappropriate, difficult behavior is a powerful positive reinforcement for the termination of the mealtime. As a result, the parent/caregiver is likely, probably sooner than later, to end the mealtime. Thus, both the child’s and the caregiver’s behaviors are being reinforced, and the problem not only persists, but probably grows with time.
In our study we found that regardless of the etiology approximately 15% of children with feeding difficulties had BMI < –2 z-score. We could not identify any publications assessing nutritional status in children with feeding difficulties regardless of the primary cause that would enable us to compare the data. Our results showed that detailed assessment of nutritional status should be one of the standards of care for children with feeding difficulties. The crucial part of the diagnostic and intervention process is cooperation between many specialists (pediatrician, gastroenterologist, psychologist, nutritionist, speech therapist) and the child’s caregivers.
The strength of our study was a relatively large sample size. During the diagnostic process, we had access to the patients’ detailed medical records and the data were complete. Moreover, the classification of feeding difficulties and etiology was done by at least two specialists: a medical doctor and a psychologist. Our study was conducted as a single-center study, which limits generalization of its results to other populations. However, given the limited number of treatment centers for feeding difficulties in our country, our recruited population might be representative. The cross-sectional design of our study does not prove causality. Another potential limitation of the study might be measurement error. However, all the measurements were done to minimize this problem; they were conducted using calibrated scales [25] always in the morning, following WHO protocols.
It is still unclear why some children with medical problems, despite receiving standardized therapy, develop behavioral problems. Additionally, the association of the parental BMI with the child’s BMI and feeding difficulties and nutritional impairment should be explained. This issue needs to be addressed in further studies.
In conclusion, the current study focused on etiology and nutritional status in children with feeding difficulties. An isolated behavior component was present in more than half of our patients. Moreover, we observed that organic feeding difficulties always coexisted with a behavioral component. The nutritional impairment was detected in some patients regardless of etiology. Therefore it is crucial to start complex treatment in all patients with feeding difficulties as soon as possible to prevent potential health problems in the future.