
Introduction
Overweight and obesity in children are considered among the most significant global public health problems [1–3]. Obesity at a young age is considered to be a risk factor for cardiovascular morbidity and mortality [4]. Abnormal weight in early life predisposes not only to ischemic heart disease, but also to arrhythmias [5, 6]. Ventricular or supraventricular arrhythmia may occur sporadically, intermittently or permanently in children at any age from the fetal age [7]. Cardiac arrhythmias often resolve spontaneously during the child’s development, while others do not manifest any clinical symptoms, but may cause the development of cardiomyopathy or may develop into life-threatening arrhythmias and lead to sudden cardiac death [8–11]. Monitoring and analysis of a resting ECG and/or a 24-hour Holter ECG recording with recorded arrhythmia is essential in the diagnosis of arrhythmias as a potential cause of syncope, circulatory failure, as well as in assessing the risk of sudden cardiac death [12–15]. Changes in the period of ventricular repolarization – QT interval and TpTe (Tpeak-Tend) interval – allow the assessment of electrical instability of the heart muscle. In clinical diagnosis, electrocardiographic repolarization abnormalities with prolongation of QT and TpTe intervals (Tpeak-Tend) are important for assessing the risk of malignant ventricular arrhythmias. In the literature reports, the TpTe repolarization parameter seems to be a sensitive indicator of arrhythmogenesis [16–21]. There are few studies in the literature that have analyzed the ECG in obese children, and there are no studies involving children with arrhythmias taking into account the body mass index. The aim of the study was to compare the electrocardiological values of repolarization parameters in children with and without arrhythmias, depending on body weight.
Material and methods
Study data were obtained through a retrospective analysis of medical records of children hospitalized in the Department of Pediatric Cardiology of the Saint John Paul II Upper Silesian Child Health Centre in Katowice. Repolarization parameters were compared in children with excessive and normal body weight (assessed by BMI and Cole’s index) with ventricular and supraventricular arrhythmias (study group N = 88) and in children from the control group without diagnosed arrhythmias and with normal weight (N = 34). The repolarization parameters TpTe, QT peak and QT interval corrected Bazett (QTcB) and Fridericia (QTcF) formulas were measured in lead V5 of the 12-lead ECG. All anthropometric measurements were taken on the first day of hospitalization during the physical examination before starting the ECG.
When analyzing comparative characteristics, overweight and obese children were included in the group of children with ‘abnormal body weight’ (BMI index and Cole’s index).
Studied subjects
The study group consisted of 88 children (38 girls and 50 boys) aged 4 to 18 years (mean age: 13 ±5 years) with ventricular or supraventricular arrhythmias of unknown etiology (recorded in a standard ECG and in a 24-hour Holter ECG monitoring), and 34 children with chest pain admitted for diagnostic examinations excluding cardiovascular etiology served as a control group (22 girls and 12 boys) aged 4 to 18 years (mean age: 13 ±3 years).
None of the study group subjects (including controls) had a positive personal or family history of sudden cardiac death or structural heart disease on physical examination (or) Doppler echocardiography or exercise arrhythmias (Bruce protocol).
In order to participate in this study, patients with arrhythmias had to fulfill all the following inclusion criteria: ventricular or supraventricular arrhythmias in a standard ECG and in a 24-hour Holter ECG, previous diagnosis of arrhythmias in anamnesis and in the physical examination, without episodes of sudden cardiac death in relatives of the child before the age of 30, without inflammation and ion disorders (K, Ca, Mg), no use of drugs that change the repolarization period, and no use of stimulants (cigarettes, alcohol). For patients in the control group, the inclusion criteria were: no history of symptoms suggesting arrhythmias, no arrhythmias in the ECG and 24-hour Holter ECG, normal physical examination result, with normal echocardiographic results, normal laboratory test results excluding inflammation and ionic disturbances (K, Ca, Mg), negative family history of structural and electrophysiological abnormalities of the heart, no episodes of sudden cardiac death in the child’s relatives before the age of 30 years, no use of drugs that change the repolarization period, no use of stimulants (cigarettes, alcohol).
Anthropometric measurements
Body weight and height were assessed for all children in the present study. The children were tested in underwear and without shoes. Each measurement was taken as the average of three consecutive measurements. In children, body weight and height were measured in three repetitions. Body weight was measured with a Charder MS6110 medical scale with a height gauge HM202P (JAWAG, Morawica, Poland) with an accuracy of ± 100 g. Children’s height was measured with a stadiometer attached to the scale with an accuracy of ± 0.1 cm. Mean values of height and weight were obtained from the three measurements to calculate the body mass index (BMI = body weight in kg/height in m2), which was adjusted to the standards published by Cole et al. and Cole’s index (LMS) (I% = body weight × (standard body length)2/standard body weight × (body length)2 × 100) [22].
The children were divided according to their nutritional status, once in reference to BMI and the second to Cole’ index. According to BMI, underweight was defined as children with a value below the 5th percentile, slimness between the 5th and 25th percentile and obese as a value above the 95th percentile. Taking into account Cole’s index, it was assumed that children with the index value below 75% are characterized by wasting, and children with the index value > 110% are overweight [23].
Electrocardiography
Standard ECG recordings were made in the supine position on the recorder model AT2 plus Schiller AG (Baar, Switzerland). Measurements were made manually in the fifth precordial lead (V5) of the 12-lead ECG. The analyzed measurements were the average of three consecutive QRS-T evolutions with a paper travel of 50 mm/s and a standard feature amplitude of 1 mV = 1 cm. In the analysis of the repolarization period, the duration of individual repolarization parameters and the amplitude were assessed. From three consecutive QRS-T evolutions, RR intervals, total repolarization time (QT interval) and TpTe interval (Tpeak-Tend) were determined and recorded under magnification with a magnifying glass using a distance stepper. The total period of QT repolarization was determined from the beginning of the Q wave to the end of the T wave, defined as the point of return of the descending arm of the T wave to the isoelectric line, excluding the U wave [24, 25]. Corrected QT duration for heart rate (QTcB) was calculated using the Bazett (QT/√RR) and Fridericia (QT/RR1/3) formula [26, 27]. In the case of two T-wave peaks, the first T-wave peak was taken into account in the measurements [28–30]. All measurements were analyzed blindly by two independent investigators with uniformity tests without access to the results obtained and clinical data. The highest quality ECG was analyzed without network interference with the exception of the flat T wave. 24-hour Holter was performed in all children (n = 122).
Statistical analysis
The calculations and graphs used in the article (except for minor modifications) were made in Statistica software (version 13.1, StatSoft Poland). In the statistical analysis tests for two independent samples and a test for five independent groups were used. The proposed tests depend on the normality of the distribution of the studied characteristic in the considered groups. If the test of normality of distribution in the groups under study did not show statistically significant differences with the normal distribution, a parametric test (the t-test for two independent samples) was used. Otherwise, non-parametric tests (Mann-Whitney U test or Kruskal-Wallis test) were used. The results are presented in the corresponding tables. All tables include the arithmetic mean and the standard deviation for each sample, as well as the p-value for a given test. A significance level of 0.05 was adopted in the statistical analysis. For p-values less than 0.05, statistically significant differences in the study populations can be inferred.
Results
Most children had normal weight (ventricular arrhythmias – n = 33, 71.7% (BMI), n = 24, 52.1% (Cole’s index), supraventricular arrhythmias – n = 29, 69% (BMI), n = 27, 64.2% (Cole’s index)). According to Cole’s index, 37 (30.3%) children with arrhythmias were overweight, while the BMI index indicated overweight in 22 (18%) children of this group. All children in the control group had normal weight (Table I).
Table I
Nutritional status in children with ventricular and supraventricular arrhythmias according to weight assessed by body mass index (BMI) and Cole’s index
The duration of the TpTe, QTcB and QTcF intervals were significantly longer in the group of children with arrhythmias and with abnormal weight compared to the values of the TpTe, QTcB, and QTcF intervals of the control group with normal weight according to the BMI index (Table II).
Table II
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with arrhythmias with abnormal weight and children from the control group with normal weight according to BMI index
The durations of TpTe, QTcB and QTcF intervals were significantly longer in the group of children with arrhythmias and with abnormal weight compared to the values of the TpTe, QTcB, and QTcF intervals of the control group with normal weight according to Cole’s index (Table III).
Table III
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with arrhythmias with abnormal weight and children from the control group with normal weight according to Cole’s index
Only the duration of the TpTe interval was significantly longer in the group of children with ventricular arrhythmias and with abnormal weight compared to the value of the TpTe interval of the group of children with supraventricular arrhythmias and abnormal weight according to the BMI index (Table IV).
Table IV
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with ventricular arrhythmias with abnormal weight and children with supraventricular arrhythmias with abnormal weight according to BMI index
The durations of TpTe and QTcF intervals were significantly longer in the group of children with ventricular arrhythmias and with abnormal weight compared to the values of the TpTe and QTcF intervals of the group of children with supraventricular arrhythmias and with abnormal weight according to Cole’s index (Table V).
Table V
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with ventricular arrhythmias with abnormal weight and children with supraventricular arrhythmias with abnormal weight according to Cole’s index
Only the duration of the TpTe interval was significantly longer in the group of children with ventricular arrhythmias and with normal weight compared to the value of the TpTe interval of the group of children with supraventricular arrhythmias and normal weight according to the BMI index (Table VI).
Table VI
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with ventricular arrhythmias with normal weight and children with supraventricular arrhythmias with normal weight according to BMI index
Only the duration of the TpTe interval was significantly longer in the group of children with ventricular arrhythmias and with normal weight compared to the value of the TpTe interval of the group of children with supraventricular arrhythmias and normal weight according to Cole’s index (Table VII).
Table VII
Characteristics of QT, QTp, TpTe, QTcB and QTcF intervals in the group of children with ventricular arrhythmias with normal weight and children with supraventricular arrhythmias with normal weight according to Cole’s index
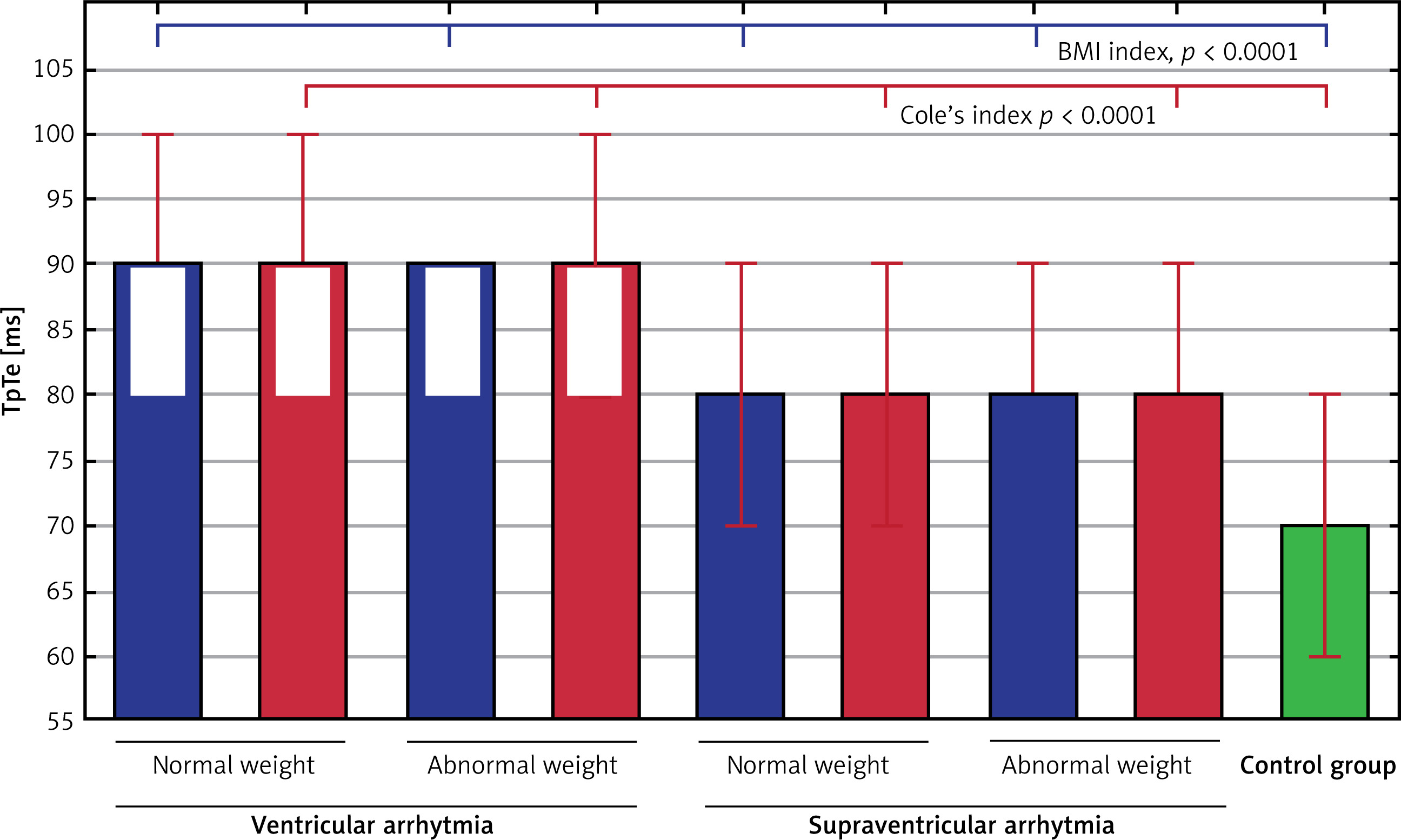
There were no significant differences (TpTe interval: using BMI and Cole’s index) in the group of children with ventricular arrhythmias with abnormal body weight and children with the same arrhythmias with normal weight, as well as in the group with supraventricular arrhythmias in terms of weight in the TpTe interval (using BMI and Cole’s index) and the QT, QTp, QTcB and QTcF intervals with their corrected values. Moreover, there were statistically significant differences in the TpTe interval between the 5 groups: children with ventricular and supraventricular arrhythmia with abnormal and normal weight, as well as the control group depending on BMI and Cole’s index (Figure 1).
Figure 1
Statistically significant differences (p < 0.0001) in TpTe intervals among the 5 groups: children with ventricular and supraventricular arrhythmia with abnormal and normal weight, as well as control group (green color) depending on BMI index (blue color) and Cole’s index (red color). Values [ms; millisecond] are shown as the median, the quartiles and the range for each group
Discussion
Compared to obese adult studies there are few studies on ECG changes in obese children. There are many studies focusing mainly on a group of young athletes to assess the risk of sudden cardiac death, without reference to anthropometric measurements [31–35]. In clinical diagnosis, electrocardiographic repolarization abnormalities with prolongation of QT and TpTe intervals (Tpeak-Tend) are important for assessing the risk of malignant ventricular arrhythmias [16–21].
Our study showed a significantly longer duration of TpTe, QTcB and QTcF intervals in children with cardiac arrhythmias (ventricular or supraventricular) regardless of body weight (assessed by BMI and Cole’s index) compared to healthy children. Similarly, previous studies by Sun et al. and Leotta et al. showed that the QTc interval was not associated with obesity in a healthy population of children [36, 37].
In the study of Yıldırım Yıldız et al., involving 81 obese children, prolongation of the QT/QTc interval in the electrocardiogram at an early age was demonstrated in obese children [38]. Similarly, in studies by Paech et al., a significant prolongation of the QTc and TpTe intervals was observed in obese healthy children compared to healthy lean children [39]. Radbill et al. observed that obesity was independently associated with the occurrence of postoperative arrhythmias in children with congenital heart defects [40]. Santini et al. presented different results, showing a significantly higher incidence of minor ECG abnormalities in underweight children and a lower incidence in obese children [41]. In subsequent studies by Paech et al., involving 53 healthy obese children and 43 lean children from the control group, no differences between the groups in the ECG recording were found, and no ECG abnormalities were recorded in healthy obese children [42].
Kiess et al. noted that the results of research on the effect of obesity in children on the ECG recording so far are inconsistent. This may be due to the fact that the pathological changes in the ECG present in obese adult patients are not so far observable in childhood [43].
Our study showed significant prolongation of the TpTe interval (using BMI and Cole’s index) and QTcF (only Cole’s index) in children with ventricular arrhythmias with abnormal body weight compared to children with supraventricular arrhythmias with abnormal body weight (Tables IV and V). Comparing children with normal weight between the ventricular and supraventricular groups, significant prolongation of only the TpTe interval was observed (using the BMI and Cole’s index) (Tables VI and VII).
In our study, it was also observed that Cole’s index seems to be a more sensitive parameter than BMI, in accordance with a previous study by Abartes et al. [23].
The repolarization parameter TpTe interval is often assessed in the pediatric population [14, 16–21, 30, 44]. However, to our knowledge, there are no scientific reports in the literature indicating a relationship between the parameters of the repolarization period in the group of children with cardiac arrhythmias (ventricular or supraventricular) and body weight (based on BMI and Cole’s index). These are novel findings in obese children with cardiac arrhythmias, and no similar data have been found in available publications to date. Clinical usefulness of the TpTe in children with ventricular and supraventricular arrhythmias and excessive body weight seems to be an interesting issue. However, it requires further research, especially on larger groups of obese children with cardiac arrhythmias, taking into consideration the sex and age of patients.
In conclusion, in children with ventricular arrhythmia, only the TpTe parameter was significantly longer compared to children with supraventricular arrhythmia and children without arrhythmia, regardless of body weight. In children with arrhythmia, regardless of body weight, the TpTe parameter should be measured in addition to routine QT. Further studies on a larger scale are needed to assess the clinical importance of the TpTe interval in children with arrhythmias and excessive body weight.