Introduction
Aortic stenosis is a progressive disease that causes compensatory mechanisms in the heart, including left ventricular hypertrophy and atrial augmentation. Degenerative valve disease is characterized by severe aortic valve calcification involving the leaflets, and the process may also involve the annulus.
In mitral valve degeneration, mitral annular calcification (MAC) may occur, particularly in patients with other degenerative calcifying diseases and well-known cardiovascular factors, such as diabetes, hypertension, hyperlipidemia, and metabolic disorders with calcium-phosphorus imbalance [1]. The calcification is usually located at the posterior mitral annulus, which may affect its whole circumference. The subvalvular apparatus of the mitral valve, mitral leaflets, and commissures are usually spared from calcification [1]; thus, less often, the function of leaflets is impaired, and stenosis occurs.
Recent studies have highlighted a relationship between hyperparathyroidism and cardiovascular disorders [2]. Elevated parathyroid hormone (PTH) levels have been associated with increased cardiovascular morbidity and mortality [2, 3], even in individuals without diagnosed hyperparathyroidism [4]. Several studies have demonstrated an association between increased PTH concentration and greater coronary artery calcification [5–7], both in patients with advanced chronic kidney disease and in those without kidney dysfunction. Moreover, hyperparathyroidism has been independently correlated with impaired coronary flow reserve [8]. The influence of PTH on heart failure development – including heart valve and muscle pathology – has also been reported [9–11]. Additionally, an association has been observed between PTH levels and the occurrence of atrial fibrillation in patients with aortic stenosis [12].
This study aimed to investigate the potential relationship between PTH levels and valvular calcification in patients with aortic stenosis undergoing transcatheter aortic valve implantation (TAVI). Additionally, the association between PTH and post-procedural outcomes was examined.
Material and methods
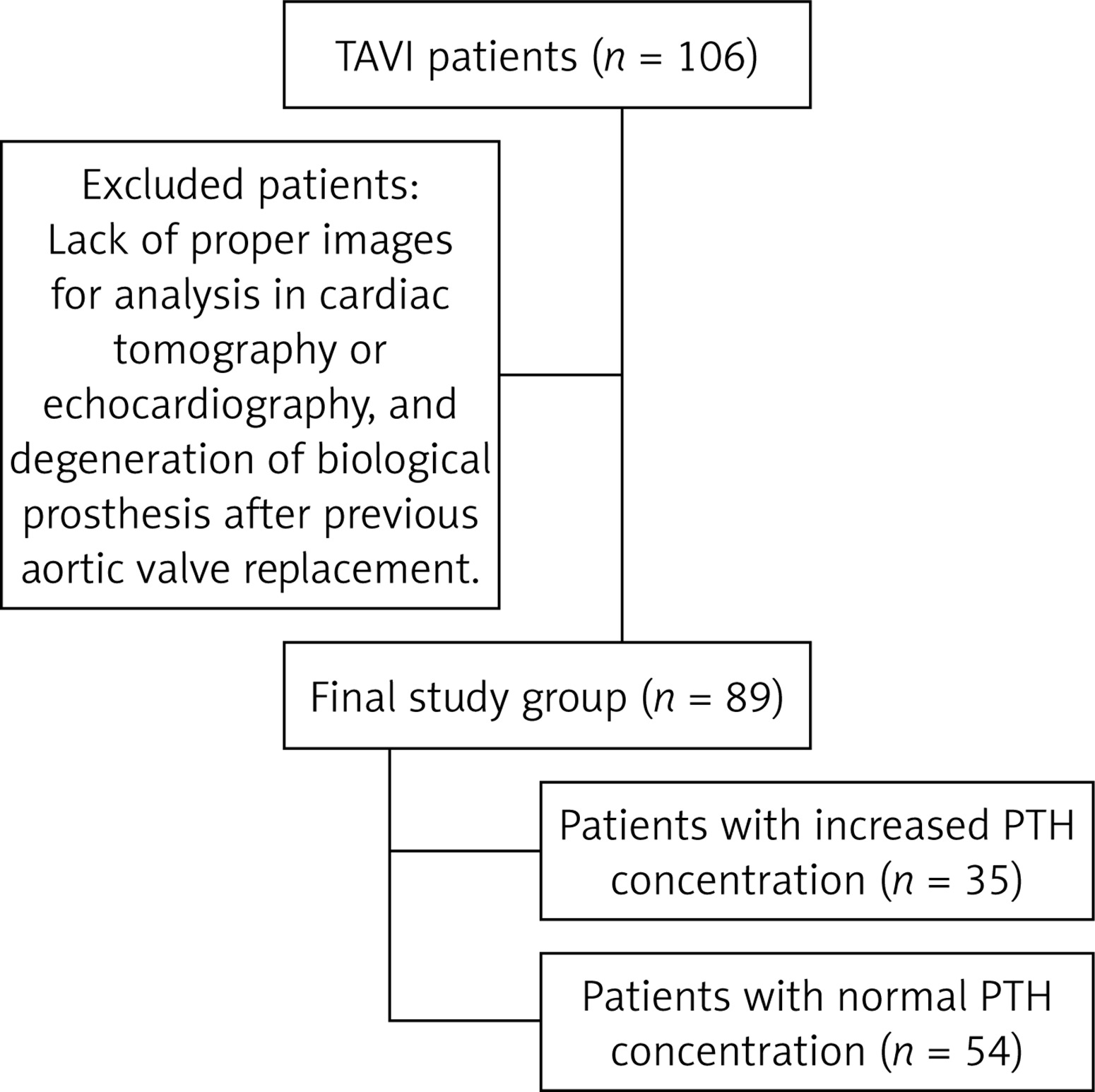
One hundred six patients with severe symptomatic aortic stenosis who underwent TAVI between May 2021 and January 2022 in two high-volume structural heart centers, and had available PTH concentration measurements, were evaluated for study eligibility. Seventeen patients were excluded from the study, including 16 due to insufficient imaging for analysis in cardiac tomography or echocardiography and one due to degeneration of a bioprosthetic valve following a previous aortic valve replacement. Additionally, patients undergoing chronic dialysis therapy or those with primary parathyroid gland disorders were excluded from the analysis. Finally, 89 patients – 50 females, 56.2%, median (Q1–3) age of 77 (72-82) years – were included in the study (Figure 1). None had a history of endocrine disorders other than diabetes mellitus, nor were they receiving specific treatment for osteoporosis.
Demographics and clinical data were collected at admission, and blood samples were obtained before the procedure. Serum intact PTH concentrations were measured using an electrochemiluminescence immunoassay kit (Abbott Diagnostics, Abbott Park, IL, USA), with normal reference values ranging from 15 to 68.3 pg/ml.
Echocardiography was performed at admission by an experienced echocardiographer, following a standardized study protocol based on current guidelines for valvular disease management [13, 14]. Routine assessment included aortic stenosis severity based on maximum and mean systolic transvalvular gradients and effective orifice area. Left ventricular contractility and ejection fraction (LVEF) were also evaluated. Pulmonary artery systolic pressure was calculated. Mitral valve disease insufficiency was recorded. If MAC was observed, its grading was based on literature reports [1]. Post-procedural echocardiography was performed at discharge, assessing peak and mean transvalvular gradients as well as paravalvular leak (PVL). PVL was classified into four grades: none, mild, moderate, or severe.
TAVI was performed in the hybrid room under fluoroscopic and echocardiographic guidance by the same team of experienced operators. Transfemoral access was obtained either percutaneously or via surgical cut-down. In cases of severe calcifications, aortic balloon valvuloplasty preceded prosthesis implantation. The implanted aortic prostheses included Evolut R/Pro (Medtronic, Minneapolis, MN, USA), Sapien 3/Sapien 3 Ultra (Edwards Lifesciences, Irvine, CA, USA), Myval (Meril Life Sciences Pvt. Ltd., Gujarat, India), Navitor (Abbott Inc., IL, USA), and Accurate (Boston Scientific, Marlborough, MA, USA). The access site was closed using vascular closure devices or surgical techniques.
Computed tomography
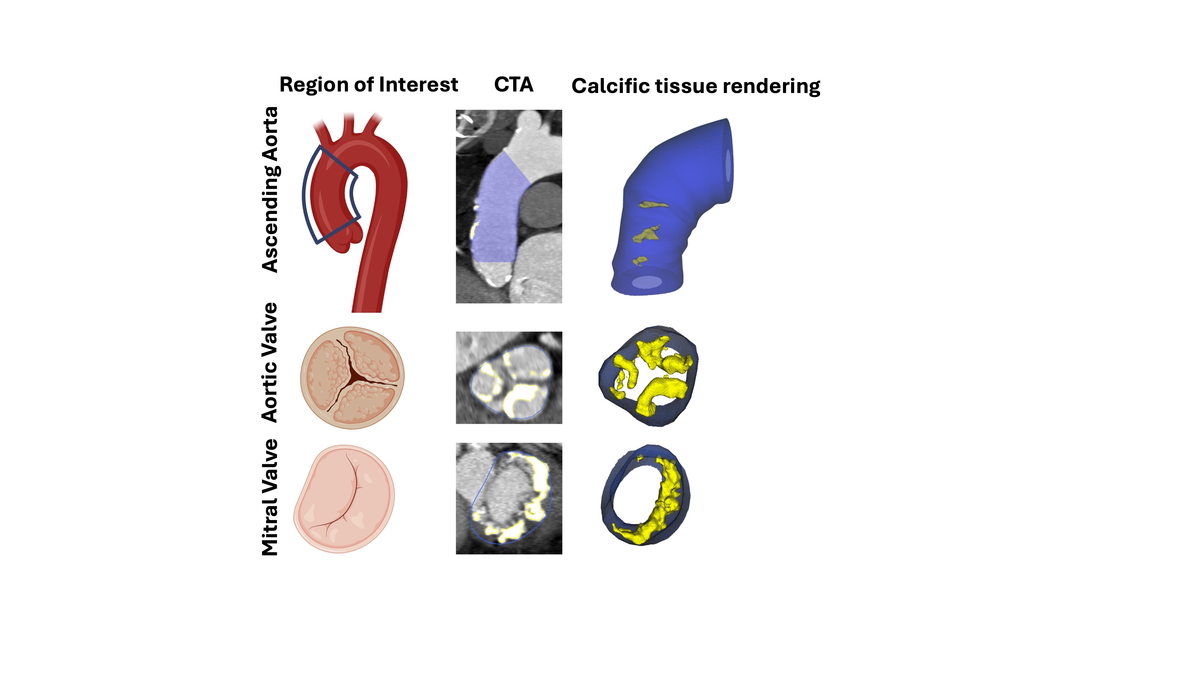
In all patients, contrast-enhanced multislice computed tomography was performed before TAVI. Quantitative evaluation of calcific tissue was conducted over the three regions of interest – ascending aorta, aortic valve, and mitral valve – using semiautomated software (Autoplaque, version 2.51; Cedars-Sinai Medical Center) and a standard mediastinal window (width, 400 HU; level, 40 HU) [15, 16]. The ascending aorta was defined as the segment between the sinotubular junction and the innominate artery. The threshold for calcified plaque was calculated by fitting a Gaussian curve to the image histogram from the aortic regular blood pool (defined by placing a circular region of interest within the ascending aorta) after adjusting with the proximal-to-distal luminal contrast enhancement distribution in the analyzed vessel. The aortic valve was defined as the region between the lower coronary ostium and the virtual basal ring formed by the hinge points of each aortic valve. The mitral valve region was adjusted using a short axis view of the mitral annulus and a stretched view with the exclusion of aortic and left ventricular outflow tract calcium. For calcific tissue quantification in valves, a Gaussian curve was fitted to the smoothed image histogram, the peak value corresponding to normal contrast in the aorta was computed, the lower threshold was set as the 99.7 percentile of blood pool CT attenuation, and all tissue above this threshold was considered calcific.
Statistical analysis
The Shapiro-Wilk test was used to evaluate the data distribution. Normally distributed data were presented as mean and standard deviation (SD). Non-normally distributed data were expressed as the median and 25th–75th percentiles (Q1–Q3). Categorical variables were presented as numbers and percentages. Student’s t-test was used for normally distributed variables, while the Mann-Whitney test was used for non-normally distributed variables. Kruskal-Wallis ANOVA was used for multigroup analysis. Categorical data were compared with Fisher’s exact test. Correlation analysis (Pearson or Spearman, where applicable) was used to describe the correlation between the variables. Statistical analysis was performed using JASP software (JASP Team; 2020. Version 0.13.1), and p ≤ 0.05 was considered statistically significant.
Results
All 89 patients presented severe calcified aortic stenosis. The population was burdened with significant co-morbidity rates, including coronary artery disease (n = 34, 38.2%), among whom 32 patients had previously undergone coronary angioplasty (n = 32, 36%); diabetes or pre-diabetes (n = 40, 44.9%); arterial hypertension (n = 71, 79.8%); chronic obstructive pulmonary disease (COPD) (n = 12, 13.5%); atrial fibrillation (n = 30, 33.7%); and chronic kidney disease defined as glomerular filtration rate (GFR) < 60 ml/min/1.73 m2 (n = 41, 46%). Ten patients had previously undergone pacemaker implantation (11.2%). Increased PTH concentration (over 68.3 pg/ml) was observed in 35 (39.3%) patients.
Echocardiographic results
All patients presented with severe aortic stenosis, with a mean (SD) peak aortic gradient of 89.4 (24) mm Hg, a mean (SD) mean aortic gradient of 56.6 (16.2) mm Hg, a median (Q1–Q3) aortic valve area (AVA) of 0.6 (0.6–0.7) cm2, and a median (Q1–Q3) LVEF of 53.6 (50–60)%. In 30 (33.7%) patients, MAC was recorded.
PTH concentration correlated weakly positively with peak aortic gradient (p = 0.034, Pearson’s r = 0.225).
There was no correlation between PTH and mean aortic gradient (p = 0.142, Pearson’s r = 0.157), LVEF (p = 0.322, Spearman’s rho = –0.106), or pulmonary artery systolic pressure (p = 0.638, Spearman’s rho = 0.058). Patients with echocardiographic features of MAC did not differ significantly in PTH concentration (median (Q1–Q3) 61.6 (42.9–84.3) vs. 61 (47.5–81.2) pg/ml, p = 0.788).
Increased PTH concentration was associated with a higher peak aortic gradient (p = 0.024), as presented in Table I.
Table I
Echocardiographic characteristics of patients with increased and normal PTH concentrations
CT results
Mitral valve mean calcific tissue attenuation (p = 0.004), aortic valve mean calcific tissue attenuation (p < 0.001), and ascending aorta mean calcific tissue attenuation (p < 0.001) differed between patients with increased and normal PTH concentrations (Figure 2, Table II).
Figure 2
Box plot of mean calcific tissue attenuation in aortic valve (I), mitral annulus (II), and ascending aorta (III), measured in patients with increased PTH concentration over 68.3 pg/ml (1) and among normal values (0). The box plot shows the minimum and maximum values [whiskers], median [black line] and interquartile range [box] values for each variable. Outliers are shown with black points
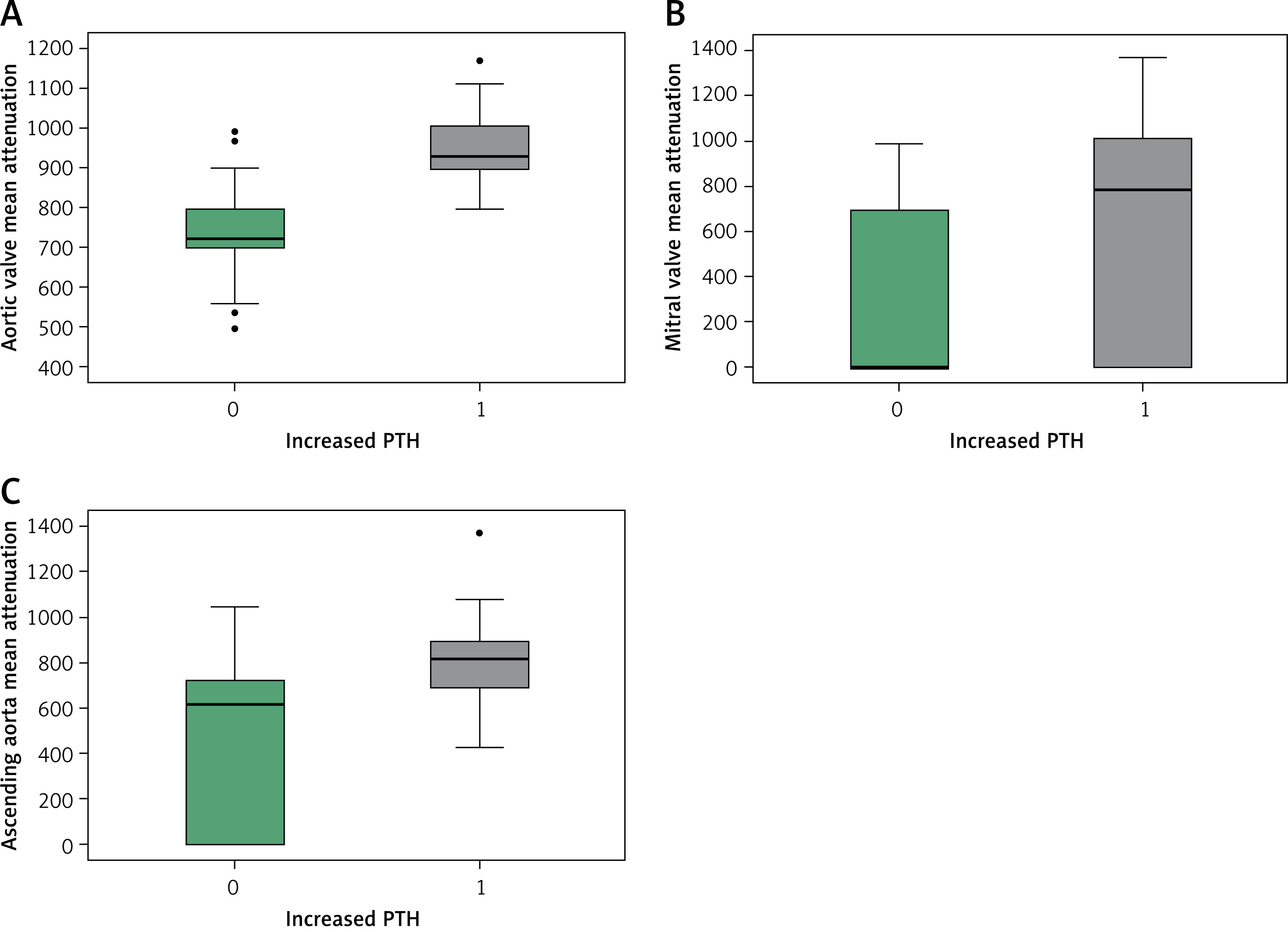
Table II
Characteristics of patients with increased and normal PTH concentrations in CT examination
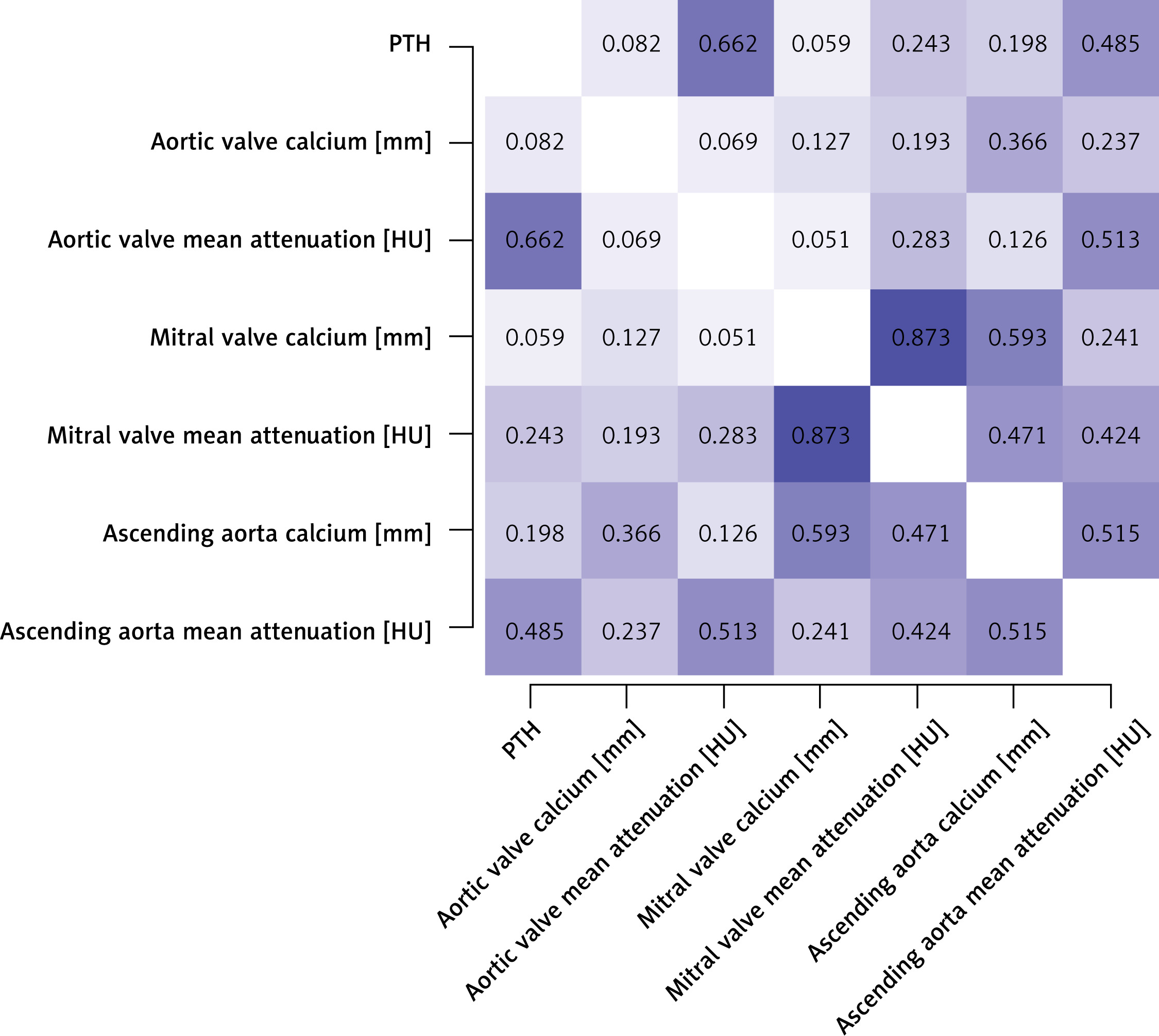
PTH concentration correlated positively with aortic valve mean calcific tissue attenuation (p < 0.001, Spearman’s rho = 0.662), mitral valve mean calcific tissue attenuation (p = 0.022, Spearman’s rho = 0.243), and ascending aorta mean calcific tissue attenuation (p < 0.001, Spearman’s rho = 0.485) (Figure 3).
Post-procedural prosthesis function and related complications
PTH concentration did not correlate with postprocedural mean (p = 0.516, S rho = –0.078), or peak (p = 0.960, Spearman’s rho = 0.006) transvalvular gradients.
PTH concentration did not differ in subgroups with no (64.1 (48.5–83.7) pg/ml), mild (58.3 (39.5–77.1) pg/ml), or moderate (77.2 (60.6–87.1) pg/ml) PVL (p = 0.910). Increased PTH did not differentiate the subgroups (0.479).
New pacemaker implantation occurred in 14 patients. After excluding patients with previous pacemaker implantation (n = 10), subgroups with new implantation (n = 14) and without pacemaker implantation (n = 65) did not differ in PTH concentration (61.9 (56.2–70.1) vs. 60.1 (43–84.1) pg/ml, p = 0.842). The increased PTH group did not differ from the normal PTH group in pacemaker implant rate (0.549).
Discussion
The study revealed associations between PTH concentration and characteristics of valvular and aortic calcifications. This suggests two important considerations: first, a potential role of PTH in the pathophysiology of valvular disease progression, particularly in the development of calcium deposits in intracardiac and arterial tissues; and second, the possible utility of PTH as a non-invasive marker of calcific load in valvular heart disease, which could help track the progression of valvular stenosis and aortic degeneration. However, PTH concentration was not useful in identifying patients at higher risk for of PVL or pacemaker implantation. Finally, given the association between PTH and valvular degeneration, further studies are warranted to explore the potential for pharmacological interventions targeting PTH in these patients.
Based on the results of our study, PTH may influence the development of calcific aortic stenosis and mitral annulus calcifications. While we did not assess PTH concentration in patients without aortic stenosis, we observed higher peak transaortic gradients in patients with abnormal PTH concentrations. Additionally, a weak but positive correlation was found between PTH serum concentration and peak systolic transaortic gradient. Increased PTH concentration was specifically associated with more prominent calcific tissue attenuation in all examined regions. We hypothesize that this observation reflects the progression of mitral annulus and aortic root calcification during the development of aortic valve disease. The association appears not to relate to the volume of calcific tissue but rather to its attenuation or density, suggesting a potential link between PTH and the inflammatory response. Aortic stenosis is a progressive fibrocalcific and inflammatory process characterized by monocyte and macrophage infiltration into valvular tissues, the release of a cytokine cascade, and the subsequent progression to cardiac fibrosis and calcification. This may explain the observed relationship between increased PTH levels and calcific tissue characteristics [17]. As previously reported [18], we observed an increased monocyte-to-lymphocyte ratio in patients with aortic stenosis and impaired contractility.
Valvular aortic pathology involves both inflammatory and mechanical pathomechanisms. Valvular endothelial cells respond morphologically to shear stress [19], undergoing changes due to alterations in mechanical and hemodynamic stimuli. Certain valvular lesions develop preferentially on the leaflet side, exposing these parts to different mechanical forces. Notably, velocity gradients are different between the two sides of the leaflet: the inflow surface experiences a strong pulsatile, unidirectional shear stress, while the outflow surface is subjected to much lower recirculating shear stress [19]. Additionally, differences in ventricular and aortic pressure waves create varying profiles for the valvular leaflets and large arteries. As a result, the endothelium on each side of the leaflet experiences different strain patterns. Sclerotic valvular pathology shares similarities with atherosclerosis as the endothelial cells’ protective role against interstitial cell activation and calcium accumulation is compromised in a mineral-rich extracellular environment [20]. Valvular endothelial cells become activated with increased expression of monocyte adhesion receptors (VCAM-1, ICAM-1, E-selectin) [21]. It is likely that PTH interferes with these inflammatory processes, promoting increased calcium deposition in altered tissue. PTH receptors are present within the cardiovascular system, including vasculature and heart [22]. PTH induces oxidative stress and necrotic cell death by promoting mitochondrial calcium excess, which subsequently leads to myocardial fibrosis and calcification [23]. The results of our study suggest that PTH is associated with abnormal calcium load in cardiac tissues, rather than the extent of calcifications.
Similar to aortic calcification, our study showed the relationship between increased PTH and calcific tissue attenuation in the mitral valve and ascending aorta. This suggests that PTH may exert a similar effect on other cardiac and arterial regions. In an animal study, Neves et al. [24], demonstrated the development of significant aortic medial calcification and coronary calcification in rats following high infusions of synthetic PTH. Undoubtedly, the mechanisms through which PTH acts in different regions of the cardiovascular system and drives calcification require further investigation.
The secondary aim of the study was to analyze the relationship between PTH concentration and post-procedural outcomes. Although PTH levels were associated with characteristics of valvular calcification, they did not correlate with the post-procedural risk of paravalvular leak (PVL) or pacemaker implantation. Previous studies have highlighted the impact of aortic valve calcification on the increased risk of PVL and conduction disturbances [25]. However, our study found no differences in PTH concentration between patients with and without these post-procedural complications. It is important to note that the increase in PTH was associated with calcific tissue density, rather than its volume, which may partly explain these findings. Additionally, other factors, such as the size and type of prostheses, could influence the outcomes.
Based on our study results, we hypothesize that medications affecting PTH concentration may play a role in managing aortic stenosis. Given the calcific and inflammatory nature of aortic stenosis, which shares pathophysiological similarities with atherosclerosis [26], several therapies proven effective in coronary artery disease [27, 28] have also been explored in aortic stenosis [29, 30]. However, the significant benefits of statin use in coronary artery disease have not been mirrored in valvular disease, as shown in randomized clinical trials such as SEAS, SALTIRE, and ASTRONOMER [31, 32]. Interestingly, recent reports emphasize the role of lipoprotein(a) (Lp(a)) in the progression of aortic stenosis [33, 34]. Genetic variation in the Lp(a) locus lead to elevated plasma Lp(a) levels, which have been associated with a 2-fold increased risk of aortic valve calcification [35]. A post-hoc analysis of the ASTRONOMER study revealed that patients in the highest tertile of Lp(a) levels had a faster echocardiographic progression of aortic stenosis and needed surgery more often [36]. As a result, novel therapies targeting the reduction of Lp(a) levels are being tested for their clinical effectiveness.
In light of our findings, we hypothesize that strategies aimed at modifying abnormal PTH concentration could help prevent calcium accumulation and slow the progression of calcification or valvular pathology. In experimental animal studies, evocalcet, an oral calcimimetic agent that inhibits PTH secretion from parathyroid gland cells, was shown to prevent ectopic calcification in the aorta [37]. Conversely, a case report highlighted the rapid progression of aortic stenosis during treatment with teriparatide, a recombinant form of PTH [38].
A key limitation of our study is the lack of subgroups with normal valves or moderate aortic stenosis and varying PTH concentrations, as well as the absence of long-term follow-up with sequential PTH measurements to assess its influence on the progression of valvular calcification. Additionally, the varying sizes and types of implanted prostheses may have influenced the analysis of post-procedural outcomes.
In conclusion, increased PTH concentration is associated with calcific tissue attenuation but not calcium volume, suggesting that PTH may influence the degree of calcium accumulation in degenerated regions. PTH could potentially serve as a biomarker of calcific loading in valvular heart disease. However, PTH concentration does not appear to be linked to the rate of complications following TAVI.