Introduction
Communication skills play a pivotal role in healthcare systems and are recognised as a fundamental aspect of professionalism, significantly influencing the quality of care provided by general practitioners [1]. Effective communication and interpersonal skills are the cornerstone of successful medical practice and can have a profound impact on patient satisfaction, adherence to medical recommendations and health outcomes [2]. The doctor-patient relationship has evolved over time, transitioning from a paternalistic model to a patient-centred approach that respects patients’ needs, autonomy and preferences. Today, patient-centred care is becoming increasingly prominent in clinical practice, encouraging general practitioners to consider illness from the patient’s perspective [2]. Key communication skills include listening, providing clear and comprehensible health guidance and adapting communication style and responses to align with the patient’s needs, perceptions and emotions [3]. Given these developments, general practitioners and healthcare professionals are expected to proactively address patients’ expectations by employing effective communication strategies to explain diagnoses, conduct thorough examinations and formulate treatment plans. Moreover, general practitioners are required to demonstrate competencies such as delivering bad news sensitively, providing effective health counselling, communicating efficiently with patients’ families, dedicating sufficient time for consultations, maintaining professional and courteous manners and respecting patients’ emotions [4, 5]. The effectiveness of communication is shaped by multiple factors, including economic and cultural influences [6]. The quality of doctor-patient communication also depends on the nature of their relationship, which is, in turn, influenced by the personality traits of both parties. Ideally, general practitioners should consider their own personality traits when adapting their communication approach with patients. Within healthcare, communication is not only a clinical skill but also a therapeutic tool that fosters meaningful relationships and benefits all involved [7]. Research suggests that the communication skills of general practitioners do not always align with patient expectations [8]. Scientific literature indicates that doctors may underestimate the importance of effective communication [9]. Many general practitioners believe they possess adequate health communication skills and often overestimate their ability to communicate effectively with patients [10–12]. Additionally, general practitioners may be unaware of how patients perceive their communication practices. As a result, there might be discrepancies between how doctors and patients assess the quality of communication during consultations [13]. General practitioners emphasise the importance of medical knowledge and experience, as well as the role of competence and efficiency. They assess relationships based on their problem-solving abilities, usefulness, reliability and credibility. However, they often overlook the ‘softer’ aspects of interpersonal interactions, such as care and empathy, which are particularly important to patients. This misalignment of expectations can contribute to a loss of trust in the doctor-patient relationship [14]. A study conducted among general practitioners in Germany, Greece, Spain and Cyprus identified significant gaps in knowledge, skills and training related to health communication [15]. The analysis highlights multiple areas requiring improvement in doctor-patient communication, with verbal communication – particularly questioning and listening skills – identified as a key challenge [16]. Studies indicate that strong verbal communication skills, such as active listening, greeting patients and expressing gratitude for their cooperation, are essential to fostering effective communication with patients. Furthermore, an empathetic and compassionate attitude directly enhances patient satisfaction with medical consultations. Providing comprehensive information about a patient’s condition and treatment is crucial in ensuring they fully understand their diagnosis or therapy. These elements contribute to building trust and strengthening the doctor-patient relationship [17, 18]. Research conducted in the United States suggests that many patients withhold or misrepresent important health information when speaking with their doctors. In fact, 60–80% of Americans admitted to not being truthful about details that could be relevant to their health [19]. This highlights the critical role of effective communication and trust in maintaining or restoring health. In light of these considerations, this study aimed to identify both strengths and areas requiring improvement in interpersonal skills among Polish general practitioners, as well as to examine the factors influencing their communication skills.
Material and methods
Research tool
The study used a structured questionnaire consisting of two main sections: sociodemographic data and an assessment of communication skills. The sociodemographic section included questions about age, gender, years of professional experience, workplace location (urban or rural), average consultation time per patient, daily patient load, preferred type of consultation (in-person visit at a healthcare facility, home visit, or teleconsultation), and participation in soft skills training. Communication skills were evaluated using the validated Interpersonal Communication Skills Inventory (Learning Dynamics, 2002), which focuses on four key areas: Sending Clear Messages, Listening, Giving and Receiving Feedback, and Handling Emotional Interactions. Each of these areas was assessed through 10 questions, where participants scored between 0 and 3 points for each response, corresponding to ‘rarely’, ‘sometimes’, or ‘usually’. This resulted in a maximum score of 30 points per section. The interpretation of scores was as follows: 1–15 points: Areas requiring improvement; 16–21 points: Areas needing more consistent attention; 22–30 points: Areas of strength in communication skills. Reliability analysis of the tool yielded Cronbach’s a coefficients between 0.75 and 0.89 for all sections, indicating good internal consistency. The questionnaire underwent a pilot testing phase, aimed primarily at assessing the clarity of the questions and determining the time required for completion.
Study framework
The study was designed and reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. The study was conducted during the fourth quarter of 2024 using the CATI (computer-assisted telephone interview) method. The sample size was calculated to be a minimum of 371 general practitioners, based on a sample size calculator. The inclusion criterion was that participants must be active general practitioners working in primary healthcare facilities (both public and private) in Poland. Additional study assumptions included: A comparable number of physicians from public and private healthcare facilities, and The sample size in each voivodeship should be proportional to the number of respondents in that region.
Recruitment of respondents
The phone numbers were randomly drawn from a database containing doctors’ contact details. A total of 3,865 calls were made, of which 2,956 were unanswered, 31 were follow-up calls made at the respondent’s request for a different time (successful), and 27 were follow-up calls during interrupted interviews due to the respondent’s return to their duties (successful). Out of 870 successful contacts, 851 individuals met the eligibility criteria. However, 19 individuals were excluded due to retirement, and 179 refused to participate despite meeting the eligibility criteria. Additionally, 72 interviews were interrupted during the process. Ultimately, 600 completed interviews, with all survey questions answered, were included in the final analysis. Incomplete responses (n = 72) were excluded, and no data imputation was performed. To assess the potential for bias, a comparative analysis was conducted between the complete and incomplete responses, focusing on age and gender. The relatively low response rate may be attributable to the substantial workload and cognitively demanding nature of physicians’ professional duties, a factor that warrants consideration when interpreting the study results. Despite the rigorous selection process, the study acknowledges the potential for selection bias, as participation was limited to general practitioners who could be contacted and who consented to participate. Furthermore, the use of self-assessment in evaluating communication skills may have introduced bias due to the subjective nature of respondents’ perceptions of their abilities.
Ethical considerations
Before participating in the study, each respondent was informed about its scientific nature and the possibility to discontinue the interview at any time. In accordance with bioethical guidelines, ethical approval was not required for this study, as it was non-invasive and did not meet the criteria for a medical experiment under Polish law.
Statistical analysis
Descriptive statistical analysis was performed to summarize the data. Non-parametric tests were used to analyse the results. The Mann-Whitney U test was employed to compare two independent groups, while the Kruskal-Wallis test was used for comparisons involving more than two groups. Statistical analyses were conducted using Statistica 13.3 (StatSoft) and R 4.3.1, with statistical significance set at p < 0.05.
Results
The majority of respondents were women (60.3%), and one in three respondents (30.4%) was aged between 41 and 50 years (Table I). Most respondents had between 11 and 30 years of professional experience. The respondents most commonly worked in cities with fewer than 200,000 (41.8%) inhabitants. The vast majority (92.5%) considered in-person consultations to be the most effective and preferred form of patient consultation. For more than half of the respondents (53.0%), the average consultation time per patient ranged between 10 and 15 min. Two-thirds (66.3%) believed this consultation time was sufficient. More than half (56.3%) of the respondents reported seeing an average of over 30 patients per day (Supplementary Table SI). The vast majority (98.5%) of respondents believe that a doctor’s communication skills are important for patients. Most primary care doctors (94.5%, combining responses rated as ‘very good’ and ‘good’) assessed their communication skills positively. The survey revealed that just over 60% of doctors had not participated in training, conferences or workshops aimed at enhancing doctor-patient communication. The overwhelming majority (97.2%) of respondents agreed that practical communication training specifically designed for doctors is necessary. The maximum possible score on the Interpersonal Communication Skills Inventory was 120. The average score achieved by respondents was 72 points. Women scored significantly higher than men: 73.1 vs. 70.3 points (Table I). Doctors who rated their communication skills as poor or very poor scored higher (82.5 points) than those who rated them as good or very good (72.3 points). A significant difference in scores was also observed in relation to the assessment of the adequacy of consultation time. Doctors who considered the consultation time to be sufficient scored lower than those who perceived it as insufficient (70.6 vs. 74.8 points).
Table I
Points scored on the Interpersonal Communication Skills Inventory by characteristics of the surveyed doctors (source: own calculations)
| Overall communication skills | ||||
|---|---|---|---|---|
| Variables | Response categories | Mean score and standard deviation | Kruskal-Wallis test result | P-value |
| Age | 30–39 | 71.8(14.7) | 2.6547 | 0.6172 |
| 40–49 | 71.0 (15.7) | |||
| 50–59 | 72.1 (15.6) | |||
| 60–69 | 72.9 (15.9) | |||
| > 70 | 75.3(18.4) | |||
| Years of professional experience | < 10 | 71.8 (15.0) | 3.0268 | 0.5533 |
| 11–20 | 71.5 (15.7) | |||
| 21–30 | 71.0 (16.0) | |||
| 31–40 | 73.8 (13.7) | |||
| > 40 | 74.8 (18.6) | |||
| Workplace location | Rural | 69.5 (15.8) | 5.9863 | 0.7465 |
| City < 200 k inhabitants | 72.5 (15.6) | |||
| City 200–500 k inhabitants | 71.6(16.0) | |||
| City > 500 k inhabitants | 73.1 (15.4) | |||
| Self-assessment of communication skills | Very good, good | 72.3 (15.5) | 9.0895 | 0.01062* |
| Average | 63.4 (14.6) | |||
| Poor, very poor | 82.5 (22.9) | |||
| Average consultation time per patient | < 10 min | 71.6 (14.6) | 0.83259 | 0.8417 |
| 10–15 min | 72.0 (16.1) | |||
| 15–20 min | 72.8 (15.7) | |||
| > 20 min | 70.8 (14.4) | |||
| Average daily patient load | 1–10 patients | 67.9 (16.3) | 5.3842 | 0.1457 |
| 11–20 patients | 70.5 (16.0) | |||
| 21–30 patients | 71.0 (14.8) | |||
| > 30 patients | 73.2 (15.8) | |||
| Variables | Response categories | Mean score and standard deviation | Mann-Whitney U test result | P-value |
| Gender | Male | 70.3 (15.3) | 47303 | 0.04194* |
| Female | 73.1 (15.8) | |||
| Sufficient consultation time | Yes | 70.6 (15.2) | 46483 | 0.001735* |
| No | 74.8 (16.2) | |||
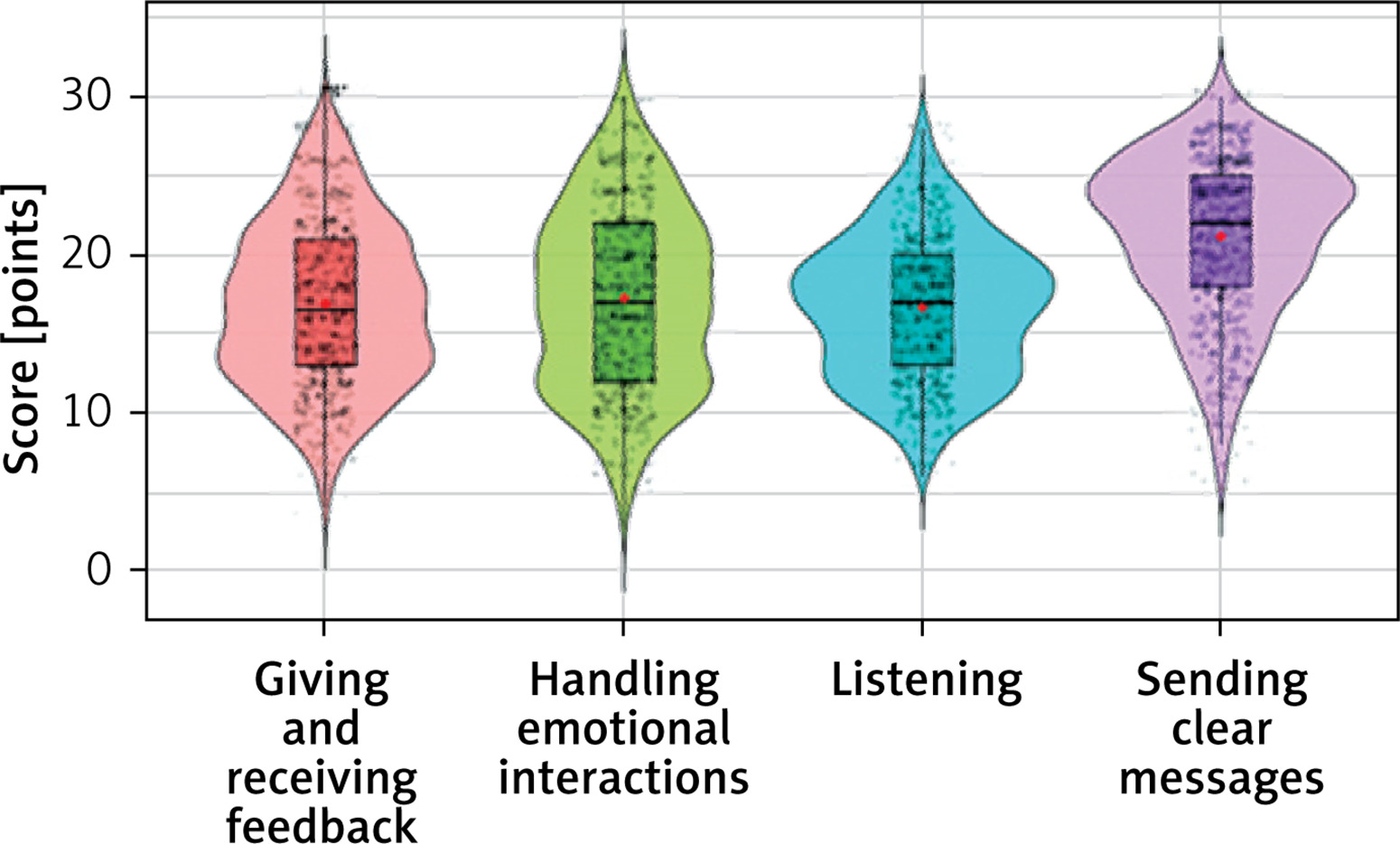
An analysis of the individual areas of communication skills revealed that the strongest area of communication skills among doctors was, in particular, Sending Clear Messages (Table II, Figure 1). For the remaining communication skills, particularly in Listening and Giving and Receiving Feedback, respondents scored lower.
Table II
Communication skills of general practitioners: average scores for surveyed areas – descriptive statistics (source: own calculations)
Figure 1
Communication skills of general practitioners: average scores for the assessed areas (source: own calculations)
Sending clear messages
The analysis revealed significant differences in the communication skills of general practitioners in the area of Sending Clear Messages, based on factors such as age, years of professional experience and average consultation time (Table III). Older doctors (aged 70 and above, as well as 60–69 years) obtained significantly higher scores in Sending Clear Messages compared to younger doctors (30–39 years). Doctors with more years of experience (31–40 years and over 40 years) scored significantly higher compared to those with fewer years of experience (< 10 years) (p = 0.001). Doctors who considered the consultation time to be sufficient had significantly lower scores in Sending Clear Messages compared to those who felt the consultation time was too short (p = 0.004).
Table III
Scores in the Interpersonal Communication Skills Inventory for Sending Clear Messages by selected characteristics of the surveyed general practitioners (source: own calculations)
Listening
The analyses revealed significant differences in the level of communication skills among general practitioners in the area of Listening, as related to: their subjective assessment of communication skills, the average consultation time per patient and participation in training that supports communication skills (Table IV). Respondents who rated their communication skills as average, good or very good scored significantly lower in Listening than those who rated their communication skills as poor or very poor (p = 0.005). Doctors who stated that the time allocated for visits was sufficient had significantly lower scores in Listening compared to those who felt the consultation time was too short (p = 0.014). General practitioners who participated in communication training for doctor-patient interactions scored significantly lower in Listening than those who did not participate in such training (p = 0.001).
Table IV
Points scored in the Interpersonal Communication Skills Inventory in Listening, according to selected characteristics of the surveyed general practitioners (source: own calculations)
Giving and receiving feedback
The results demonstrate significant differences in the communication skills of doctors in the area of Giving and Receiving Feedback, based on: self-assessment of communication skills, gender, average consultation time per patient and participation in training supporting doctor-patient communication (Table V). Women scored significantly higher in Giving and Receiving Feedback compared to male respondents (p = 0.024). Respondents who rated their communication skills as average, good or very good had significantly lower scores in Giving and Receiving Feedback compared to those who rated their skills as poor or very poor (p = 0.048). Doctors who stated that the time allocated for a visit was sufficient had significantly lower scores in Giving and Receiving Feedback compared to those who believed the consultation time was too short (p = 0.005). Respondents who reported participating in training supporting communication had lower scores in Giving and Receiving Feedback compared to those not participating in such training (p < 0.001).
Table V
Points obtained in the Interpersonal Communication Skills Inventory in Giving and Receiving Feedback by selected characteristics of the surveyed doctors (source: own calculations)
Handling emotional interactions
The level of communication skills among doctors in Handling Emotional Interactions varied significantly, depending on: self-assessment of communication skills, participation in training supporting doctor-patient communication and opinions regarding the need for practical communication training dedicated to doctors (Table VI). Participants who rated their communication skills as average, good or very good scored significantly lower in Handling Emotional Interactions compared to those who rated their skills as poor or very poor (p = 0.015). Doctors who reported participation in communication training for doctors scored lower in Handling Emotional Interactions than those who had never participated in such training (p = 0.019). Doctors who recognised the need for practical communication training achieved higher scores in Handling Emotional Interactions compared to those who did not perceive this need (p = 0.043).
Table VI
Points obtained in the Interpersonal Communication Skills Inventory in Handling Emotional Interactions by selected characteristics of the surveyed general practitioners (source: own calculations)
Discussion
This study found that the strongest communication skill among the respondents was Sending Clear Messages. Similar findings were reported in a Lithuanian study on healthcare professionals [20]. Interestingly there is evidence that doctors who expressed uncertainty about diagnoses and lacked the competence to provide thorough explanations experienced lower levels of patient trust and a reduced adherence to treatment effectiveness among patients [21].
In another Polish study, it was found that the most highly rated aspects of communication included allowing the patient to speak without interrupting (50.4%), speaking in a way that the patient could understand (47.6%) and paying attention to the patient (47.2%). According to patients’ opinions, doctors frequently neglected key aspects of communication, such as encouraging them to ask questions (28.4%), involving them in shared decision making (29.2%) and discussing the next steps of treatment (35.2%) [22]. These aspects can be classified as elements related to Giving and Receiving Feedback, which in this study also emerged as an area requiring improvement.
Listening was identified as the weakest communication skill among the surveyed general practitioners. Research indicates that some general practitioners struggle with active listening. Engaging in active and reflective listening requires general practitioners to attend to the emotional and personal aspects of a patient’s condition [23]. Effective listening, along with sufficient time dedicated to it, positively impacts accurate information exchange, verification, and socio-emotional communication in healthcare settings [24]. Patients highly value being heard, taken seriously and understood. Medical professionals should not only attend to physical symptoms but also acknowledge patients’ emotions and the broader context of their concerns. However, listening as a clinical skill remains largely neglected in medical training. Existing communication programmes primarily emphasise what to say rather than how to listen [25].
Depending on the specific area of communication skills assessed, factors influencing the observed differences in results included: gender, age, years of experience, self-assessment of communication skills, perception of the adequacy of consultation time, the perceived need for practical communication training and participation in training programmes that support patient-doctor communication.
The study showed that female general practitioners achieved significantly higher scores in Giving and Receiving Feedback, compared to their male counterparts. Other studies also suggest that female doctors tend to be more empathetic and possess better communication skills than males. This aligns with the current findings, where female general practitioners were noted to better empathise with patients’ situations, understand their concerns, listen patiently and respond effectively [8]. In primary care, female practitioners are often expected to spend more time with patients, pay more attention to them and display greater empathy. This is because women are socially perceived as more nurturing, caring and expressive, compared to men. On the other hand, male communication styles tend to be more direct and task-oriented, with expectations that they will demonstrate authority and leadership, which may make it harder for patients to ask questions. However, this approach can sometimes be seen as distant and indifferent, potentially hindering effective patient-doctor communication and shared decision making [26, 27].
In this study, general practitioners who rated the consultation time with patients as insufficient demonstrated better communication skills in three out of four areas: Sending Clear Messages, Giving and Receiving Feedback and Listening. It appears that consultation time plays a crucial role in patient-doctor communication. Doctors who spent three additional minutes per consultation showing interest and asking about patients’ family and well-being were perceived as having better communication skills compared to those who consulted in a shorter time frame [28–30]. Furthermore, short consultations were found to contribute to polypharmacy, antibiotic overuse and poor patient-doctor communication [30]. Doctors with shorter consultations also reported higher levels of burnout, due to a lack of personal achievement and a sense of lower productivity, especially in the context of treating patients with multimorbidity.
This study found that medical professionals with longer years of experience demonstrated better communication skills, but only in the area of Sending Clear Messages, compared to those with less experience. No significant differences were observed in other communication areas in relation to years of practice. Interesting findings were reported in the study by Kruse et al., which revealed that medical students with significantly less professional experience exhibited higher levels of empathy than experienced doctors. This suggests a decline in perceived empathy as professional experience increases [31].
Conversely, another study indicated that greater professional experience was associated with improved communication skills [32]. In the same study, however, no association was found between respondents’ age and their communication skills. This result contrasts with our own findings, as older practitioners demonstrated better communication skills compared to younger doctors, specifically in Sending Clear Messages. Results regarding the influence of age and professional experience on communication are inconsistent across studies. For example, another study highlighted that younger doctors excelled in two key areas: obtaining and providing information and discussing subsequent treatment steps with patients. Greater experience does not necessarily lead to better communication skills. Older doctors, who have been in practice longer, may be more prone to emotional burnout. Therefore, although they have more experience in patient-doctor communication, they may not necessarily communicate more effectively [33].
In all four areas of communication skills examined, overall self-assessment of communication skills proved to be a significant factor. Interestingly, the results suggest that the surveyed doctors were not fully aware of their communication abilities. This contrasts with other research findings, where doctors tend to overestimate their communication skills [34]. This discrepancy may be attributed to differing perspectives between patients and doctors regarding what constitutes effective communication. Patients often favour a psychosocial model of communication, while doctors more commonly apply the biomedical model [35].
Scientific literature highlights the importance of intensively training patient-doctor communication skills, both during undergraduate medical education and throughout postgraduate training [1]. Our study found that respondents who reported no need for further communication training scored lower in communication skills, particularly in Handling Emotional Interactions. Although communication skills are influenced by various personal factors, research indicates that these abilities can be enhanced through targeted training and experience [2].
Building on the communication findings of this study, the results indicate a clear need for systemic changes in Poland and across Europe that place greater emphasis on the quality of health communication, patient education, and shared understanding as integral components of prevention strategies. Strengthening clinicians’ communication competencies and ensuring sufficient time and structural support for meaningful interactions between patients and clinicians are closely aligned with the recommendations of the European Program for Prevention (EPP), which calls for the immediate implementation of proven, evidence-based preventive measures within routine care [36]. In this context, health education is a critical tool for improving health literacy, supporting fact-based decision making, and countering misinformation and disinformation, thereby enhancing trust and patient experience, an effect also observed with supportive services in hospital care [37]. To make these gains durable, periodic training in communication should be mandated and repeated as part of compulsory professional training required of medical personnel, with protected time and organizational support; repeated training also strengthens clinical effectiveness by improving adherence, safety, and outcomes. Taken together, these findings both support and can be further reinforced by the EU Safe Hearts Plan, as they highlight communication and education as foundational enablers of effective cardiovascular prevention, while coordinated EU level initiatives provide a structural framework that amplifies the implementation of EPP principles through consistent, communication-centred preventive policies.
The main limitation of the study is that data were obtained solely through self-reporting by doctors, which introduces the risk of systematic bias, particularly self-assessment bias and social desirability bias. Physicians may overestimate their communication skills or respond in ways they perceive as socially acceptable, rather than providing an accurate reflection of their behaviour. Interestingly, the results revealed that doctors who rated their communication skills as poor or very poor actually achieved higher objective scores, potentially indicating the presence of the reverse Dunning-Kruger effect – where more competent individuals are more critical of their own abilities. To enrich the findings, it would be valuable to include the perspective of patients regarding doctors’ communication skills. Additionally, the study considered a limited range of factors that may influence doctor-patient communication. Given the complex and multifaceted nature of this interpersonal dynamic, further research could broaden the analysis by exploring personal factors that may affect doctor-patient communication.
In conclusion, the results suggest that the surveyed doctors may lack full awareness of their communication skills. This highlights the need for the introduction of standardised diagnostic assessments in this area, alongside the implementation of targeted training programmes focusing on patient-doctor communication. The results may have broader relevance for primary care systems where physician-patient communication is a key determinant of care quality.