Introduction
Connective tissue diseases (CTD) is a disease characterized by autoimmune-mediated damage caused by circulating autoantibodies, which can affect multiple parts such as the skeleton, muscle, joints and blood vessels [1]. CTD includes rheumatoid arthritis, dermatomyositis, Sjögren’s syndrome, undifferentiated CTD, ANCA-associated vasculitis and systemic sclerosis, and is characterized by chronic inflammation of blood vessels and connective tissue [2, 3]. Interstitial lung disease (ILD) is a common complication of CTD and one of the main causes of death [4]. CTD-ILD presents a wide range of clinical manifestations. Symptoms can progress from a asymptomatic state to severe dyspnea, and the range of involvement can extend from a single organ of the respiratory system to multiple organs.
With the progression of the disease, patients may experience lung parenchyma destruction and progressive decline in lung function, which eventually threaten life [5]. Early and accurate diagnosis of CTD-ILD is essential to improve the prognosis of patients. However, due to the complexity and diversity of its clinical manifestations, clinicians face many challenges in early diagnosis, determination of treatment timing, and selection of appropriate therapeutic drugs [6]. Traditional diagnostic methods, such as clinical manifestations, imaging and laboratory tests, often lack specificity or sensitivity [7]. In recent years, with the development of biomarker research, serum tumor markers have gradually attracted attention as a class of important biomarkers. The ideal biomarkers should be non-invasive or minimally invasive, and should have high accuracy for disease prediction [8]. In the past, tumor markers were mainly used as important tools for the screening and diagnosis of common cancers, such as gastric cancer, breast cancer, and liver cancer.
In recent years, serum tumor markers have been revealed to have a certain relationship with the occurrence and development of CTD-ILD. Abnormal expression of these markers may be related to the inflammatory response, tissue damage, and repair process caused by CTD; however, the specific mechanism is not fully understood [9]. Carbohydrate antigen (CA) 125 (CA125) is widely distributed in human mesothelial cells, while CA153 is mainly secreted by human epithelial cells. Both of them are broad-spectrum tumor markers, whose serum levels are significantly elevated in patients with various malignant tumors such as ovarian endometrioma [10] and breast cancer [11]. Squamous cell carcinoma antigen (SCC) is a widely used and reliable marker of squamous cell carcinoma. ILD has been reported to have a higher risk of squamous cell lung cancer and a poor prognosis [12]. As key enzyme in glycolysis, neuron-specific enolase (NSE) catalyzes the conversion of glycerol 2-phosphate to phosphoenyl pyruvate, and has neuroprotective effects. Nervous system injury causes an increase in blood NSE levels, which can help damaged neurons survive. As an autoimmune disease, CTD affects the central nervous system. ILD can cause insufficient cerebral blood oxygen supply, and in severe cases, induce pulmonary encephalopathy, which aggravates the nervous system damage and leads to a further increase in blood NSE [13]. Carcinoembryonic antigen (CEA) is extracted from colon cancer and embryonic tissues, and used to be regarded as a specific marker for early diagnosis of colorectal cancer. Later, clinical studies found that it can also be elevated in tuberculosis, CTD, and nephrotic syndrome, so the specificity is poor [14].
Based on this, this study innovatively applied serum tumor markers to the diagnosis of CTD-ILD, in order to explore their expression characteristics in the disease and their relationship with clinical characteristics. Through this novel research perspective, we expect to be able to provide new biomarkers and diagnostic methods for early diagnosis of CTD-ILD, thereby improving the quality of life and prognosis of patients.
Material and methods
General data
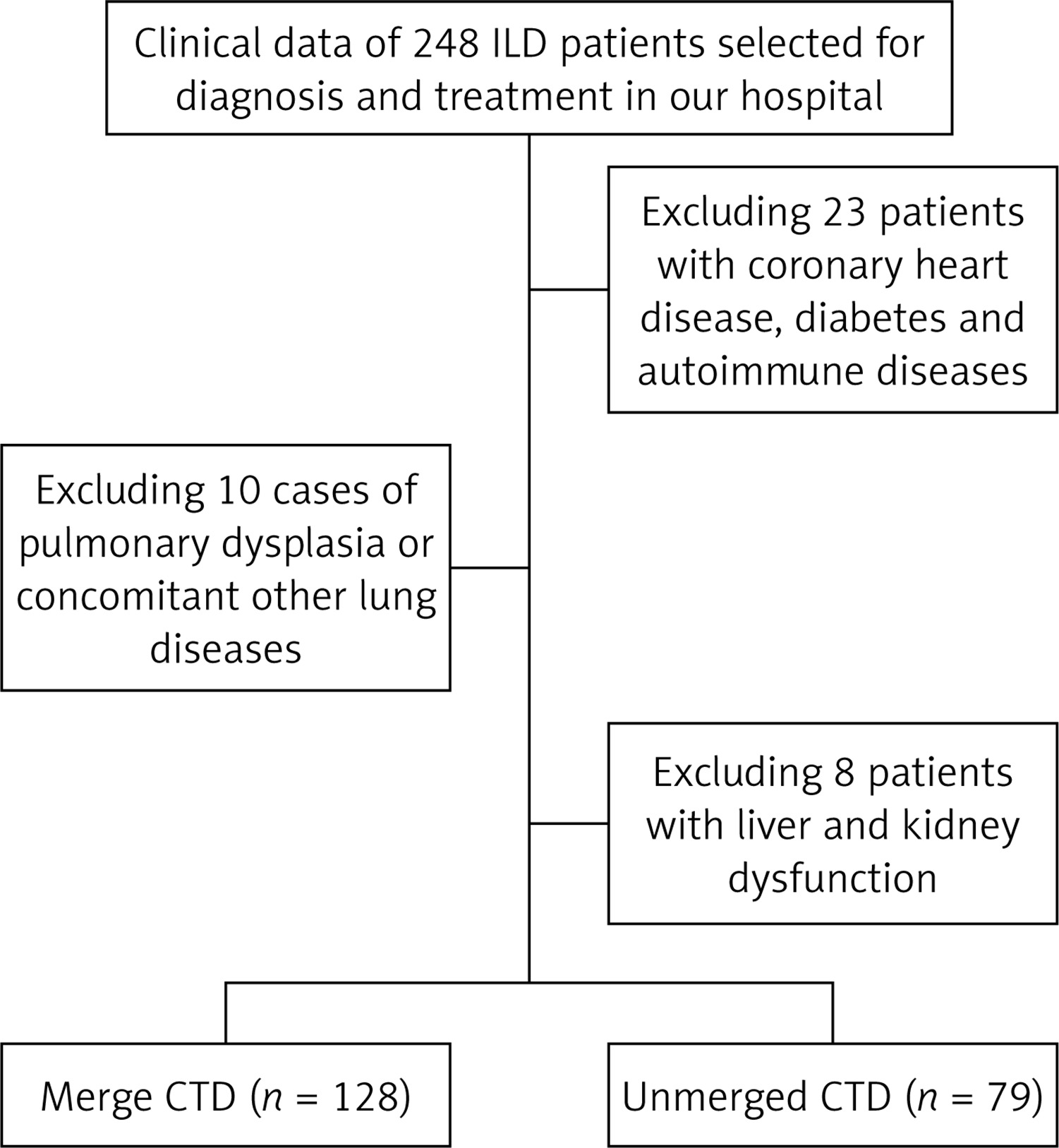
The clinical data of 207 patients with ILD diagnosed and treated in our hospital from January 2020 to December 2023 were retrospectively analyzed. The inclusion process is shown in Figure 1. Based on the presence of CTD, the patients were divided into the combined group (128 cases) and non-combined group (79 cases). In the combined group, there were 56 males and 72 females with the average age of 59.46 ±8.93 years (28–79 years). The average course of disease was 2.69 ±1.29 years, and the body mass index (BMI) was 21.41 ±2.88 kg/m2. In the non-combined group, there were 32 males and 47 females with the average age of 60.24 ±11.85 years (31–76 years). The average course of disease was (2.35 ±1.13) years, and the BMI was (22.02 ±3.46) kg/m2. There was no significant difference in general clinical data between the two groups (p > 0.05).
Among the 128 patients with CTD-ILD, there were 52 rheumatoid arthritis patients with ILD, 5 dermatomyositis patients with ILD, 41 Sjögren’s syndrome patients with ILD, 19 undifferentiated CTD patients with ILD, 8 ANCA-associated vasculitis patients with ILD, and 3 systemic sclerosis patients with ILD.
Inclusion criteria: (1) patients with coexisting ILD met the guidelines for the diagnosis and treatment of interstitial pulmonary fibrosis [15]; (2) the diagnosis was confirmed by imaging examination; (3) patients with clinical manifestations such as cough, chest tightness, pulmonary rales, and shortness of breath; (4) patients with complete clinical data. Exclusion criteria: (1) patients with coronary heart disease, diabetes and autoimmune diseases; (2) patients with pulmonary hypoplasia or other pulmonary diseases; (3) patients with malignancies and infectious diseases; (4) patients with liver and kidney dysfunction.
The contents of the general information section were based on the retrospective analysis of ILD patients diagnosed and treated in our hospital from January 2020 to December 2023; therefore, the data were accurate and reliable. Patients’ grouping, inclusion criteria, and exclusion criteria were strictly set to ensure the scientific validity of the study.
Clinical data collection
Clinical manifestations: The clinical manifestations included rash, arthralgia, dry mouth and eyes, chest pain, fatigue, fever, cough, shortness of breath after activity, Raynaud’s phenomenon, and oral ulcers.
Imaging manifestations: The imaging findings were detected by imaging examinations and analyzed by experts, including ground-glass opacity, reticular opacities, fiber stripe opacities, and other imaging characteristics.
Laboratory indices: Laboratory indices included albumin, C-reactive protein, total protein, globulin, and white blood cell count.
Serum tumor markers: Serum tumor markers included α-fetoprotein (AFP), CA125, CA153, SCC, CEA, NSE, and cytokeratin 19 fragment (CYFRA21-1).
Statistical analysis [16]
SPSS v23.0 software was used to analyze the data. Measurement data were expressed as mean ± standard deviation (x ± s), and t-tests was used for comparison between groups. Count data were presented as (cases, %), and analyzed by chi-square tests between groups. ROC curve analysis was used to assess the clinical value of single and combined serum tumor markers for the diagnosis of CTD-ILD. P < 0.05 was considered statistically significant.
Results
Analysis of clinical characteristics of the two groups
In a detailed comparison of the clinical characteristics of the combined group and the non-combined group, there were significant differences in the manifestations of arthralgia, rash, Raynaud’s phenomenon, dry mouth and dry eyes between the two groups. In the combined group, there were 54 patients with arthralgia, 26 patients with rash, 59 patients with Raynaud’s phenomenon, and 32 patients with dry mouth and dry eyes, accounting for 42.19%, 20.31%, 46.09%, and 25.00%, respectively. In the non-combined group, there were 12 patients with arthralgia, 5 patients with rash, 14 patients with Raynaud’s phenomenon, and 10 patients with dry mouth and dry eyes, accounting for 15.19%, 6.33%, 17.72%, and 12.66%, respectively. Statistical analysis showed that the differences in these symptoms between the two groups were statistically significant (p < 0.05), indicating that ILD-CTD patients were more likely to have these clinical manifestations. There were no significant difference in age, BMI, course of disease, gender, oral ulcer, fatigue, fever, cough, shortness of breath after activity, chest pain, ground-glass opacities, reticular opacities, and fibrotic stripe opacities between the two groups (p > 0.05, Table I).
Table I
Analysis of clinical characteristics in both patient groups (cases, %)
Comparative analysis of laboratory indicator levels between the groups
There were no significant differences in the levels of C-reactive protein, globulin, and white blood cell count between the combined group and the non-combined group (p > 0.05). The levels of serum albumin and total protein in the combined group were significantly lower than those in the uncombined group. The serum albumin in the combined group was 32.79 ±6.79 g/l, and that in the non-combined group was 37.37 ±4.02 g/l (t = 5.433, p < 0.001, Table II). The total protein in the combined group was 62.53 ±8.85 g/l, and that in the non-combined group was 68.58 ±7.79 g/l (t = 4.997, p < 0.001, Table II). This may be related to the chronic wasting disease characteristics of CTD patients, leading to decreased nutritional status of the body.
Table II
Comparative analysis of laboratory indicator levels between the two groups (x ± s)
Analysis of serum tumor marker levels between the groups
The serum tumor markers in the combined group were CA125 39.85 ±4.23 U/ml, CA153 31.53 ±8.92 U/ml, CEA 6.96 ±1.28 ng/ml, SCC 2.18 ±0.75 ng/ml, and NSE 18.19 ±2.31 ng/ml, which were significantly higher than those in the non-combined group (p < 0.001, Table III). The abnormal elevation of these tumor markers may be related to the inflammatory response and fibrotic process of CTD-ILD.
Table III
Analysis of serum tumor marker levels in two groups of patients (x ± s)
ROC curve analysis
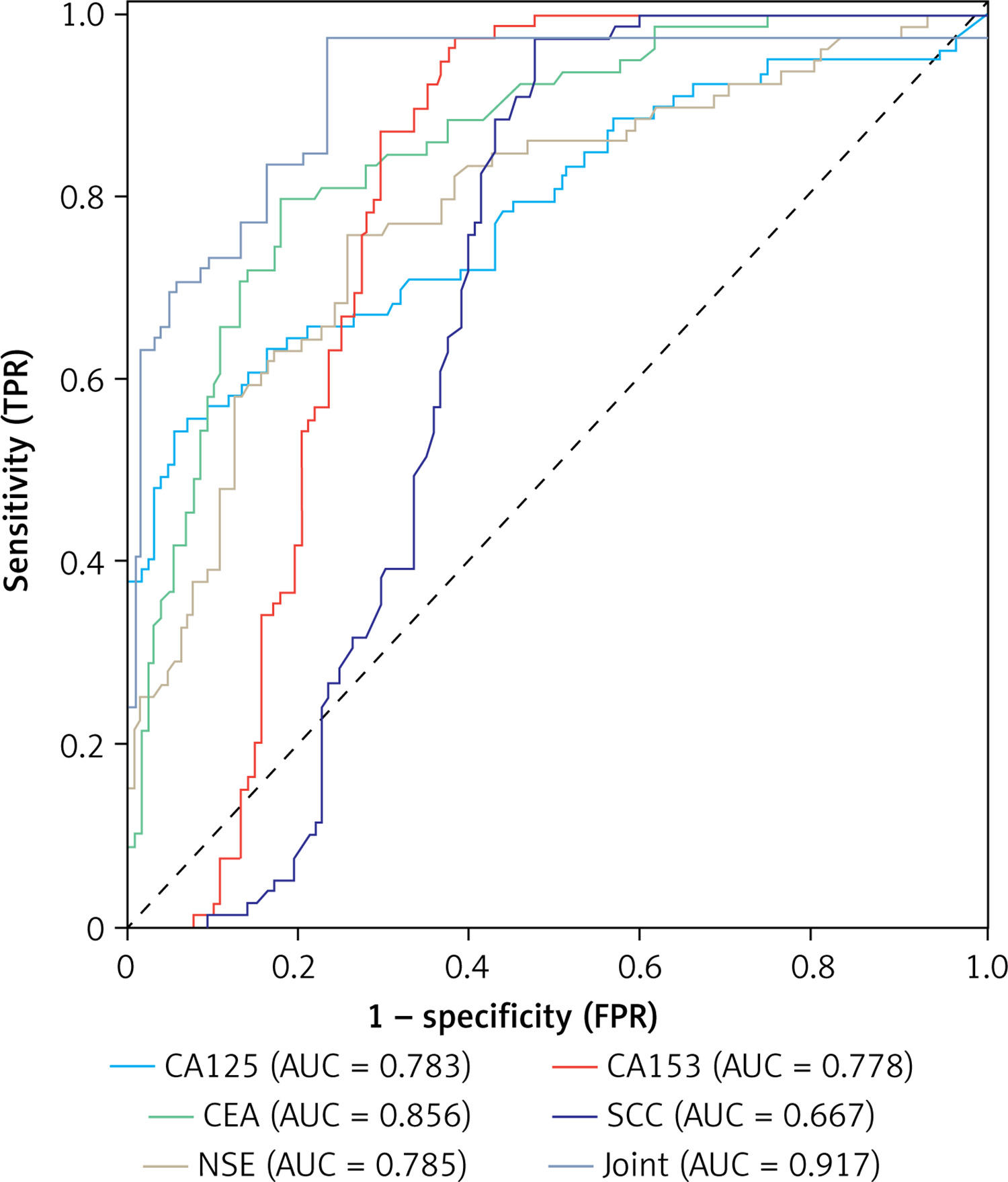
The CTD-ILD diagnosis was used as the state variable, and the levels of each serum tumor marker were used as the test variable, to draw the ROC curve. The ROC curve of each tumor marker was produced by the software calculation. The AUC values of CA125, CA153, CEA, SCC, and NSE were 0.783, 0.778, 0.856, 0.667, and 0.785, respectively. The sensitivity of CA153 and SCC was high, both reaching 97.47%, which meant that these two indicators could detect most patients with CTD-ILD. However, it should be noted that their specificity is relatively low, and there may be many false positive results. The specificity of CA125 was 94.53%, indicating that it could better exclude non-CTD-ILD patients. The p-values of each index were less than 0.05, indicating that the diagnostic value of these tumor markers was statistically significant. In addition, the combined detection and analysis of each tumor marker were performed to further improve the diagnostic efficiency. The five indicators of CA125, CA153, CEA, SCC, and NSE were combined by software, and the ROC curve of combined detection was calculated. The AUC of combined detection was 0.917, the sensitivity was 97.47%, the specificity was 76.56%, and the Youden index was 0.740 (Table IV, Figure 2). Compared with single detection, the AUC of combined detection was significantly improved, indicating that the combined detection has higher accuracy and clinical value in the diagnosis of CTD-ILD, and can provide more reliable diagnostic basis for clinicians.
Table IV
Diagnostic value of serum tumor markers for CTD-ILD
Discussion
ILD is one of the most common and clinically important manifestations of CTD, and also one of the main causes of death in patients with CTD. Genetic risk, epigenetic changes, and regulatory immune diseases are all risk factors for the pathogenesis of CTD-ILD [17, 18]. CTD-ILD can present with varying degrees of inflammation, fibrosis, and a wide range of clinical manifestations, making it difficult for clinicians to establish an early diagnosis and make decisions on treatment options, the best time to intervene, and the appropriateness of therapeutic drugs. In this study, the clinical data of 128 patients with CTD-ILD were retrospectively analyzed and compared with 79 ILD patients without CTD. This study investigated the clinical characteristics of CTD-ILD and its relationship with serum tumor markers. Below, we analyze the research results from multiple perspectives, including disease mechanism and clinical diagnosis.
The pathogenesis of CTD-ILD is complex, involving multiple aspects such as genetics, epigenetic changes and immune regulation diseases [19]. This study found that patients with CTD-ILD showed more obvious clinical manifestations such as arthralgia, rash, Raynaud’s phenomenon, and dry mouth and dry eyes than ILD patients without CTD, which may be related to the systemic inflammatory response and autoimmune injury caused by CTD. In addition, the significant reduction of serum albumin and total protein levels in the combined group suggested that CTD, as a chronic wasting disease, might lead to a decrease in the nutritional status of the body and further affect the prognosis of patients. However, ILD is sometimes the first manifestation of CTD, and about 70% of patients may not have any respiratory symptoms, only chest HRCT abnormalities. The study confirmed that respiratory symptoms are the most common symptoms of CTD-ILD [20]. However, it is easy to attribute the symptoms of fatigue and dyspnea on exertion to old age, anemia or other non-rheumatic diseases related cardiac or pulmonary complications, which ultimately delays the diagnosis of CTD-ILD [21]. Therefore, for patients confirmed or suspected of having CTD, it is necessary to be alert to the manifestations of CTD in the lung, and corresponding diagnosis and treatment should be carried out as soon as possible. In addition, CTD is a chronic wasting disease, which may not only lead to metabolic abnormalities, but also reduce protein intake through the accumulation of lesions in the gastrointestinal tract, and increase protein excretion by involving the kidneys [22]. Intravenous immunoglobulin can be used as an adjunct to the treatment of CTD. Pulse immunoglobulin therapy is an effective option in the salvage treatment of CTD patients with severe or progressive disease after conventional immunosuppressive therapy [23]. Albumin and total protein are indicators reflecting the nutritional status of the body. CTD-ILD should be considered when ILD patients have arthralgia, rash, oral ulcers, and reduced levels of albumin and total protein.
Regarding disease mechanism, in this study, serum tumor markers (CA125, CA153, CEA, SCC, and NSE) were significantly elevated in patients with CTD-ILD. In patients with CTD-ILD, the elevated levels of these markers may indicate active disease. Inflammatory activity plays a key role in the pathogenesis of CTD-ILD, and elevated markers may reflect the degree and extent of inflammation [24]. Although these tumor markers are usually associated with malignancies, a recent study showed that they may also be abnormally expressed in non-neoplastic diseases such as ILD [25]. The increase of these markers may be related to the inflammatory response, tissue damage and repair process caused by CTD, but the specific mechanisms need to be clarified with further research. CA125, CA153, and CEA are all glycoproteins. Research has demonstrated that increases of serum CA125, CA153, and CEA levels may be closely related to the severity of ILD, and can be used as biomarkers related to its pathology, which is helpful for the detection of the disease [26, 27]. In addition, a study found that the serum levels of CA125, CA153, NSE, and CEA in patients with Sjogren’s syndrome complicated with ILD were significantly higher than those in non-ILD patients [28]. Another study found that CA125 expression in idiopathic nonspecific ILD and idiopathic pulmonary fibrosis was significantly higher than that in CTD-ILD patients [29]. This differs from the results of the present study and may reflect bias due to the small number of patients in this study. In addition, due to the differences in environmental factors, the possibility of large differences in the expression of tumor markers in CTD-ILD patients in different regions cannot be excluded. The reason for the increase of serum tumor markers is still unclear.
Early diagnosis is highly important for the treatment and prognosis of CTD-ILD patients. However, due to the diverse clinical manifestations of CTD-ILD and the possible lack of specific symptoms, early diagnosis can be challenging. ROC curve analysis showed that the combined detection of CA125, CA153, CEA, SCC, and NSE had a high clinical evaluation value for CTD-ILD. Through the auxiliary diagnosis analysis of combined detection, it was found that the sensitivity and specificity of combined detection of multiple tumor markers were 97.47% and 76.56%, respectively. It indicates that the combined detection had high clinical application value in the diagnosis of CTD-ILD. Through the detection and analysis of serum tumor markers, clinicians can better judge whether a patient has CTD and provide a basis for treatment. In addition, the dynamic changes of serum tumor markers can also be used to evaluate the therapeutic effect and predict disease progression, so as to optimize clinical diagnosis and treatment programs and improve the quality of life of patients. This finding provides a new strategy for the clinical diagnosis of CTD-ILD. Traditional diagnostic methods mainly rely on clinical manifestations, imaging, and laboratory tests, but these methods often lack specificity or sensitivity. As a non-invasive and simple method, the detection of serum tumor markers can make up for the shortcomings of traditional diagnostic methods to a certain extent. Combined detection of multiple tumor markers can improve the diagnostic accuracy of CTD-ILD and provide strong support for the early treatment of patients.
In conclusion, CTD patients with ILD as the initial manifestation mainly present with clinical symptoms such as arthralgia, rash, Raynaud’s phenomenon, dry mouth, and dry eyes. The levels of serum albumin and total protein are significantly lower, while the levels of serum tumor markers (such as CA125, CA153, CEA, SCC, and NSE) are significantly higher. The combined detection of tumor markers has a high clinical evaluation value for CTD-ILD, which provides new biomarkers and diagnostic methods for early diagnosis of CTD-ILD. This finding not only enriches our understanding of the pathophysiological mechanism of CTD-ILD, but also provides new ideas and a basis for clinical diagnosis and treatment.