Cardiovascular diseases are the most common cause of death in Poland. According to the demographic forecast of the Central Statistical Office, in 2045, the number of deaths due to cardiovascular diseases is estimated to peak at 223,300/year and will constitute more than 50% of the estimated total deaths [1]. According to the Polish Cardiac Society, the most common direct causes of death from cardiovascular diseases include myocardial infarction, stroke, hypertension, atherosclerosis, and venous insufficiency. Because of the aging population, in the near future, there might be a significant increase in issues related to morbidity and mortality due to these causes [2]. To meet the challenge of a rapidly aging population, there is an urgent need to develop rapid and reliable methods of diagnosis of cardiovascular diseases. Considering this requirement, new biomarkers with high diagnostic utility in cardiovascular diseases, including hypertension, are constantly being sought (Figure 1).
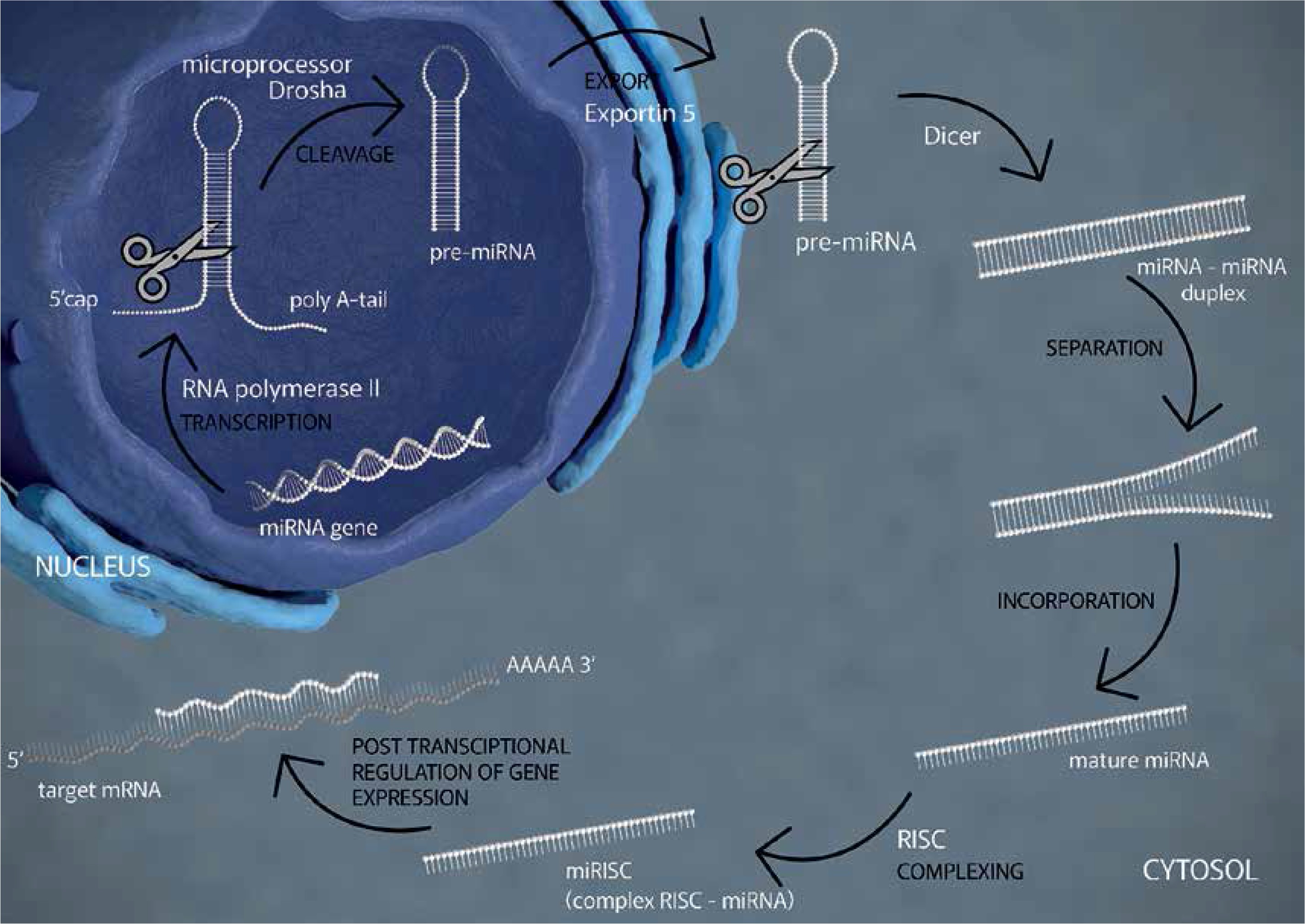
Profiling of microRNAs (miRNAs), which are short, noncoding, single-stranded RNA molecules, is a promising research direction. miRNAs interact with mRNAs and are mainly involved in the regulation of 30% of human genes that are crucial for the development and functioning of the organism and are responsible for cell division, cell differentiation, apoptosis, vessel formation, and carcinogenesis. Low plasma levels of miR-145-5p are observed in patients with acute myocardial infarction, whereas high plasma levels are found to be associated with a genetic predisposition to dilated cardiomyopathy [3]. miR-1-3p plays a key role in the development and physiology of muscle tissues, including the heart, and alterations in its expression lead to hypertrophy, infarction, or cardiac arrhythmias [4]. The miR-423-5p molecule was originally identified as a circulating biomarker of heart disease [5].
Literature data indicate that proprotein convertase subtilisin/kexin type 9 (PCSK9) binds to low-density lipoprotein (LDL) receptors to promote their degradation, thus reducing the rate of LDL cholesterol removal from plasma and subsequently causing a high risk of hypercholesterolaemia. In contrast to the negative role of PCSK9 in the cardiovascular system [6], myosin-binding protein-C (MyBPC3) has a protective role because it regulates myocardial function and protects the myocardial tissue from proteolysis [7].
Our previous study evaluated factors that are potential causes of vascular endothelial dysfunction in men with hypertension and showed an association between disease onset and levels of biomarkers of neutrophil extracellular trap (NET) formation [8].
The purpose of present study was to determine the diagnostic usefulness of selected novel parameters as biomarkers of hypertension: micro-RNA profiling (miR-145-5p, miR-1-3p, miR-423-5p), PCSK9, and MyBPC3. The concentrations of subunits of NADPH oxidase (NOX1, CYBb, and NCF2) and DNase 1, enzymes that activate or degrade NETs with anti-MPO and anti-PR3 antibodies, formed due to immunization with NETs elements, were also estimated.
Methods
The study materials were serum samples obtained from 88 men aged 56–64 years, who were previously working in the metallurgical industry in Białystok in 2009 during the project “Cardiovascular diseases and cancer in the Podlaskie region – the epidemiological situation, prevention, and health promotion”. Written informed consent was obtained from the participants prior to the collection of samples, which were stored at –80°C in accordance with GLP.
The health status of the participants was assessed by a physician on the basis of a complete medical examination and the results of morphological and biochemical tests. The first group comprised healthy men (n = 25) with normal blood pressure – the control group. The second group comprised healthy men (n = 16) with hypertension detected during the study. The third group included men (n = 40) with hypertension, who were receiving cardiological care. The fourth group included men (n = 7) with hypertension and coronary artery disease, who were receiving cardiological care. The diagnosis and classification of hypertensive patients were performed according to the guidelines of the Polish Society of Hypertension as well as the European Society of Hypertension (ESH) and the European Society of Cardiology (ESC).
ELISA
The level of miR-145-5p, miR-1-3p, and miR-423-5p were determined using the microRNA enzyme immunoassay kit (RDM0003H, RDM0019H, RDM0033H BioVendor) in samples of previously isolated RNA using the RNA Isolation Kit Plasma/Serum (RIK002, BioVendor). The levels of PCSK9 and MyBPC3 were determined using the Human PCSK9 or MyBPC3 ELISA kit (RD191473200R, RD191470200R BioVendor), respectively. The levels of IgG class anti-PR3 and anti-MPO antibodies were evaluated by the Anti-PR3-hn-hr ELISA (IgG) kit and the Anti-MPO ELISA (IgG) kit (EA 1201-9601-2 G, EA 1211-9601G Euroimmune), respectively. NOX1, CYBb, NCF2, and DNase 1 contents were measured by ELISA kits (SEA554Hu, SED308Hu, SEA300Hu, and SEB127Hu [Cloud-Clone Corp.], respectively) (Supplementary SI, SII).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Bioethics Committee of the Medical University of Bialystok (R-I-002/159/2009, R-I-002/443/2019, APK.002.111.2020).
Statistical analysis
All statistical analyses were performed using Statistica version 13.3 (StatSoft, Inc., Tulsa, OK, USA). The data are expressed as median and range. The Shapiro-Wilk test was used to determine whether the data were normally distributed. The Levene test was used to confirm the homogeneity of variations. Analysis of variance (ANOVA) was used to determine the difference between more than 2 mean values. Spearman’s correlation test was used to investigate the relationship between nonparametric quantitative variables. A p-value of < 0.05 was considered to be significant. The comparison of logistic regression models was performed with the use of Receiver Operating Characteristic (ROC) curves.
Results
(Table I).
Table I
Clinical and laboratory data of participants (n = 88), as median with min.–max.
| Results | Normotensive N = 25 | Screen-detected HPT N = 16 | HPT N = 40 | HPT + coronary artery disease N = 7 | P-value |
|---|---|---|---|---|---|
| miR-145-5p [amol/μl] | 0.8 (0.4–1.2) | 1.7* (1.2–2.8) | 1.3* (0.8–2) | 2.5*b (2–2.9) | *< 0.00001 b< 0.01 |
| miR-1-3p [amol/μl] | 2.1 (1.1–4) | 6.4* (5.5–7.6) | 3.8*a (2–5.9) | 7.6*b (6.8–10.4) | < 0.001 |
| miR-423-5p [amol/μl] | 2.2 (0.8–3.5) | 3.4 (2.3–4.5) | 5*a (3.5–5.9) | 6.2*c (5.5–8) | *< 0.000001 a< 0.01 c< 0.001 |
| PCSK9 [ng/ml] | 220 (108–355) | 365* (206–562) | 299* (159–716) | 326* (259–441) | < 0.05 |
| MyBPC3 [pg/ml] | 13 (4–24.7) | 28.6* (15.1–45.2) | 27.1* (13.6–52.9) | 25.9* (17.6–40.5) | < 0.02 |
| Anti-PR3 [RU/ml] | 1.3 (0.1–4.2) | 1.4 (0.3–4.8) | 2.4* (0.2–10.4) | 1.3 (0.8–2.3) | < 0.01 |
| Anti-MPO [RU/ml] | 1 (0.2–3.2) | 2.4* (0.7–6.4) | 1.9* (0.2–8) | 0.9bc (0.4–1.4) | *c< 0.01 b< 0.02 |
| NOX1 [ng/ml] | 13.8 (10.3–17.5) | 10.6* (8.6–14.9) | 9.4* (4.6–12.3) | 11.3 (7.3–13.3) | < 0.01 |
| CYBb [ng/ml] | 1.5 (0.7–2.6) | 1.1 (0.5–1.9) | 0.9* (0.3–2.8) | 0.7* (0.5–1.3) | < 0.04 |
| NCF2 [ng/ml] | 0.4 (0.1–1) | 1.6* (1–1.9) | 3.4*a (2–4.6) | 1.4b (0.9–2.5) | *b< 0.02 a< 0.001 |
| DNASE1 [ng/ml] | 0.93 (0.61–1.28) | 1.314 (0.80–1.61) | 1.94*a (0.98–3.02) | 1.28b (0.70–1.66) | *< 0.000001 a< 0.001 b< 0.01 |
| Age [years] | 59 (56–64) | 58 (56–65) | 59 (56–65) | 58 (56–63) | |
| BMI < 25 [kg/m2] | 27.1 (22–35) | 28.1 (23.1–32.2) | 28.9 (19.7–38.3) | 26.3 (23.2–32.3) | |
| Cholesterol < 200 [mg/dl] | 210 (145–260) | 248 (153–339) | 224 (161–311) | 240 (199–293) | |
| LDL-C < 115 [mg/dl] | 123 (55–169) | 150 (77–235) | 137.5 (93–197) | 145 (121–210) | |
| HDL-C > 40 [mg/dl] | 66 (34–122) | 60 (48–95) | 65 (37–117) | 61 (44–72) | |
| TGs < 150 [mg/dl] | 99 (56–206) | 144 (79–362) | 119 (41–392) | 134 (76–320) | |
| SBP < 140 [mm Hg] | 130 (115–140) | 157.5* (150–180) | 140*a (115–180) | 160 (110–170) | *< 0.02 a< 0.01 |
| DBP < 90 [mm Hg] | 80 (80–85) | 100* (90–100) | 87.5* (80–110) | 100 (70–100) | *< 0.01 |
miRNA assessment
The results showed significantly higher levels of miR-145-5p and miR-1-3p in the second, third, and fourth groups than in the control group. The miR-423-5p level was significantly higher in men with hypertension and in those with hypertension and associated coronary artery disease than in the control group. The highest values of these parameters were observed in the fourth group of patients with hypertension and coronary artery disease. The miR-1-3p level was lower in hypertensive patients than in men with detected hypertension. In contrast, the level of miR-423-5p was higher in hypertensive patients than in men with detected hypertension. Patients with hypertension and coronary artery disease showed higher levels of miR-145-5p and miR-1-3p than hypertensive patients. Moreover, the level of miR-423-5p in patients with hypertension and coronary artery disease was higher than that in men with detected hypertension.
Evaluation of PCSK9 levels
The PCSK9 levels in the serum of the second, third, and fourth groups were significantly higher than that of the control group. The group of men with detected hypertension showed the highest level of PCSK9.
Evaluation of MyBPC3 levels
The assay results revealed significantly higher levels of MyBPC3 in the second, third, and fourth groups than in the control group; the highest value was noted in men with detected hypertension.
Evaluation of the levels of anti-PR3 and anti-MPO antibodies
The measurement of the amount of anti-PR3 and anti-MPO antibodies in the serum samples of all the participants showed negative results (a positive result is assumed for values ≥ 20 relative units).
Measurement of the levels of NADPH oxidase subunits
Men with detected hypertension and hypertensive patients showed significantly lower NOX1 levels than the control group. The CYBb levels were lower in hypertensive patients and patients with hypertension and coronary artery disease than in the control group. The healthy control group showed the highest levels of NOX1 and CYBb. The NCF2 level was significantly higher in men with detected hypertension and in the hypertensive group than in the control group. The highest NCF2 level was observed in hypertensive patients, and it was significantly higher than that in men with detected hypertension and in patients with hypertension and coronary artery disease.
DNase 1 level measurement
Analysis of DNase1 levels in the serum samples of the participants showed the highest median value of DNase 1 level in hypertensive patients, and this value was significantly higher than those of the other groups.
Correlations
Table II summarizes the obtained correlations between the examined parameters in the studied groups of men.
Table II
Statistics
Discussion
In our initial exploratory mechanistic study, high levels of miR-145-5p, miR-1-3p, and miR-423-5p indicate the involvement of the selected miRNAs in hypertension. Because there are few published studies on this topic, it is difficult to compare the obtained results with literature data, and the available data show contrasting findings. It is believed that both miR-145-5p and miR-1-3p protect vascular smooth muscle cells by regulating processes related to their proliferation and migration. The results of the study by Rizzacasa et al. shed new light on the reason for differences in blood microRNA levels. The authors noted that the circulating miR-423-5p level was downregulated within 24 h of the acute myocardial infarction event and upregulated after 6 months in plasma of the same group of patients [9]. The contradictory results related to miRNA levels from different research centres might also be due to different study methods and differences in patient selection, age, sex, or race. Research on the potential use of miRNAs in medicine has great prospects, but this needs to be validated in a large group of subjects by considering all variables. In the present study, the positive correlations observed between the miRNA molecules tested indicate a significant relationship between them, which confirms the validity of selecting this panel of biomarkers, but no specific suggestion of ability to diagnose a condition can be made on the basis of this small cohort.
The high levels of PCSK9 in all groups of hypertensive men observed in our study may be a direct cause of the high levels of total cholesterol and LDL-cholesterol in these patients. This hypothesis was confirmed by the observation of the highest PCSK9 levels in men with diagnosed hypertension along with the highest levels of total cholesterol and LDL-cholesterol in this group of subjects. Moreover, the analysis of the impact of PCSK9 on the ability to classify patients into the group of people with hypertension showed that the model significantly loses quality (p < 0.000001) in the case of the analysis of only cholesterol and LDL-cholesterol levels, excluding PCSK9. The area under the ROC curve (AUC) illustrating the ability to classify the model increased significantly with the simultaneous analysis of these 3 parameters (p = 0.001378) in these patients. High levels of PCSK9 are a risk factor for cardiovascular events such as acute myocardial infarction, premature myocardial infarction, heart failure, or atrial fibrillation [10]. Our results indicate that PCSK9 may also be a risk factor for hypertension. Modern therapeutic strategies attempt to use specific miRNA molecules that can target and thus regulate the expression of PCSK9. The results of numerous studies prove the effectiveness of using PCSK9 inhibitors on the lipid profile. The FDA (US Food and Drug Administration) and EMA (European Medicines Agency) have approved the use of selected PCSK9 inhibitors (alirocumab and evolocumab) in patients with primary hypercholesterolaemia or mixed dyslipidaemia in addition. The beneficial effect of the use of PCSK9 inhibitors has also been shown in myocardial infarction, stroke, and cardiovascular events [11, 12].
The positive correlation observed in our study between PCSK9 and MyBPC3 levels in patients with screen-detected hypertension and the similar direction of changes observed in the levels of these studied proteins in other groups of men indicate a significant relationship between them. Studies by other authors have shown that cardiac MyBPC is rapidly released into the blood after myocardial injury and therefore may be a biomarker of early phase myocardial infarction [13]. It is estimated that 1 in 100 people in the world carries a mutation of the MYBPCS3 gene – the “myocardial infarction risk gene”. Given the function of this protein, the highest levels of MyBPC3 observed in men with detected hypertension suggests the existence of a potential mechanism to protect the myocardium from the consequences of chronic high blood pressure.
DNase 1 also has protective functions in the cardiovascular system, reduces thrombin production, and protects against the development of venous thrombosis during aging, probably through hydrolysis of free circulating DNA derived from NETs [14]. The increased level of DNase 1 observed in the present study in the same group of men with an increased amount of NET biomarkers may suggest a protective effect of this enzyme against the effects of NETs in the vascular system. However, the very high negative correlation between DNase 1 and patient age indicates that this protective mechanism may be impaired in older men.
We also showed a high negative correlation of age with NOX1, which may be related to the impairment of neutrophil function in nonspecific killing mechanisms related to NADPH oxidase activity in elderly people. The low levels of NOX1 and CYBb observed in all hypertensive men in the present study may be a result of aging. Moreover, given the results of a previously published work, the reduced NOX1 and CYBb levels may be due to “wear and tear” of the oxidase subunits in the formation of NETs. The increased formation of NETs in hypertensive men in all the study groups was confirmed by the high concentration of NCF2, which was released into the extracellular environment due to cell lysis. Low levels of oxidase subunits are a natural mechanism to protect not only against excessive production of reactive oxygen species (ROS) and NETs mediated by this enzyme but also to lower blood pressure. Low levels of NOX1 and CYBb may also be the result of high levels of miRNAs. Xu et al. showed that miR-423-5p inhibits ROS production by blocking NOX4 [15].
Based on literature data, we hypothesize that NET formation in hypertensive men may be accompanied by the activation of autoimmune processes due to easy access of lymphocytes to autoantigens present in NET structures in the circulatory system. Our negative results for anti-MPO and anti-PR3 antibodies in all the studied groups of men exclude the development of autoimmune processes associated with NETs during hypertension.
In conclusion, our results demonstrate that the focus should not be on the determination of single proteins or miRNA molecules, but researchers should aim to establish a biomarker profile specific for a given disease. Circulating miRNAs are promising diagnostic and prognostic markers for many diseases, but their number and ability to regulate various processes is a critical limitation of their therapeutic use. PCSK9 appears to have the highest diagnostic potential as an early biomarker of screening-detected hypertension, and its highest levels in men with detected hypertension were accompanied by the highest levels of total cholesterol and LDL-cholesterol. Moreover, because of the significant role of PCSK9 in cholesterol metabolism, it should be considered as a risk factor for cardiovascular diseases.