Introduction
Cardiovascular disease is the leading cause of death in developed countries [1]. A major risk factor for cardiovascular disease is lipid disorders, so the treatment of dyslipidaemia should always be considered within the context of cardiovascular disease prevention [2, 3]. The most frequently used medications for treating lipid disorders are 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors, commonly referred to as statins [4–6]. Statins have been shown to inhibit the production of apolipoprotein B-100 in hepatocytes and to reduce the production of very low-density lipoprotein (VLDL) [7, 8]. Their effects are pleiotropic and extend beyond lipid metabolism. For example, use of statins improves prognosis in people with acute kidney injury and prevents the occurrence of colorectal cancer [9–11]. They are also used in the primary and secondary prevention of ischaemic heart disease. They reduce the risk of coronary incidents, stroke, and death from cardiac causes [12, 13]. Statins not only prolong life but also improve the quality of life [14].
Despite the substantial scientific evidence supporting the benefits of statins, numerous myths about their side effects have grown over the years. This issue is compounded by the anti-statin movement, dissemination of false information about statin therapy and lack of patient education, resulting in fear of the side effects [15]. An important clinical problem is the gap between those eligible for treatment with statins to prevent cardiovascular disease and those treated. Studies indicate that around 10% of patients refuse treatment with statins, and around 30% discontinue therapy. Fear of side effects was the most common reason for giving up or stopping treatment [16]. A meta-analysis including data from many countries around the world showed that approximately 42% of statin users discontinued treatment during a follow-up period ranging from 6 months to 12 years [17]. Statin withdrawal is associated with increased cardiovascular incident rates and mortality compared to those continuing prescribed therapy [18]. Studied and described side effects of statins are myalgia, increased liver enzyme values, and increased risk of developing diabetes [19].
Side effects associated with the use of statins in clinical trials are relatively rare. However, in clinical practice, doctors often encounter the patient’s refusal to include a statin in their treatment. Although many studies have assessed and verified the frequency of certain side effects, no studies have assessed the scale of “statin phobia” from the perspective of the doctor prescribing treatment.
The aim of this study was to investigate the most common concerns patients raised with their physicians before initiating statin treatment, which led to refusal of treatment, and to identify the most common reasons for discontinuing statins cited by doctors. Their identification will enable efforts to counter misinformation by providing evidence-based information.
Material and methods
A computer-assisted web interview (CAWI) type survey was conducted using a proprietary questionnaire. The questionnaire was distributed online, mainly via Facebook, where it was posted in doctors’ groups (membership of the groups is conditional on the presentation of a medical licence). The mailing database of the Polish Society of Family Medicine was also used. Results were collected over three months, from August to November 2023.
Before completing the survey, respondents were informed of its objectives and how the results would be used, after which they gave their informed consent to participate in the study. Participation in the survey was fully anonymous and voluntary, and the participant had the opportunity to stop the survey at any stage. They were also asked to provide an e-mail address.
The author’s questionnaire consisted of single and one multiple-choice questions. The first part included questions on informed consent and being a doctor. If the answer to one of these questions was negative, the survey was not taken into consideration. The next part concerned the respondent’s socio-economic status, including age, sex, length of service in years, and stage of the doctor’s career (specialist or in the process of specialising in family medicine, doctor without specialisation, specialist or in the process of specialising in a field other than family medicine). Subsequently, the participant was asked whether, in his/her work, he/she encounters refusal of treatment with statins from patients due to fear of a specific side effect. Liver damage, muscle damage, dementia, erectile dysfunction, development of diabetes, cataracts, and prostate cancer were considered. They were then asked to estimate what percentage of patients discontinue statins on their own without first consulting their doctor based on experience from clinical practice. The doctor was then asked whether he or she had encountered adverse reactions to these drugs in his or her patients and, if so, in what percentage. They were also asked about the most common reason for the decision to discontinue appropriate treatment in cases where this situation occurred. The final question concerned the issue of the doctor undertaking education of his patients.
The questionnaire (in English) is included in the supplementary materials. The authors of the study made every effort to eliminate potential errors in survey responses. To limit the multiple completion of the survey by the same user, the e-mail address provided could only be used once. The questionnaire could not be sent if answers to any of the questions were omitted.
The study was conducted in accordance with the Declaration of Helsinki, and approval was obtained from the Bioethics Committee of the Medical University of Wroclaw.
Statistical analysis
The variables analysed were qualitative and quantitative. Normality of distribution was assessed using the Shapiro-Wilk test. Quantitative variables were presented in the form of mean value and standard deviation. Qualitative variables were presented in the form of percentages. Comparison of qualitative variables was made using the χ2 test. Statistical significance was defined as p < 0.05. Calculations were performed using Statistica 13 software by TIBCO Software Inc. (Palo Alto, CA, USA).
Results
Characteristics of the study group
The survey was completed by 260 doctors, 188 (72%) women and 72 (28%) men. Most respondents were doctors working in primary care residents and family medicine specialists 80%. Most respondents were individuals undergoing specialization (52%). Specialists and doctors without specialization constituted 41% and 7%, respectively. The largest group consisted of doctors with ≤ 5 years of experience (51%), followed by doctors with between 5 and 10 years of experience (29%). The smallest group comprised doctors with more than 10 years of experience (20%). The average length of service in primary care was 8 years, SD 7.25 (Table I).
Reasons for refusing treatment with statins
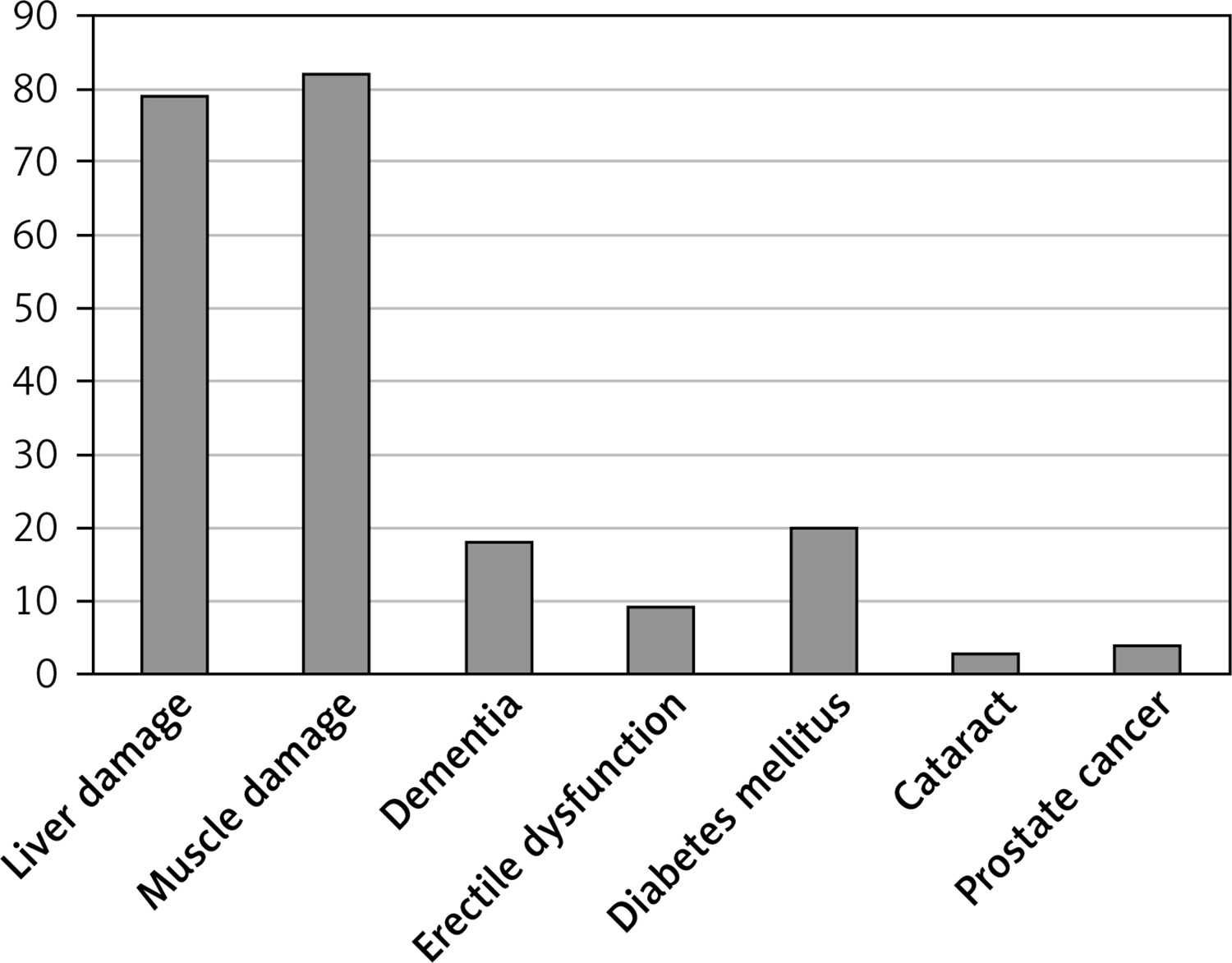
Less than 80% of doctors encountered refusal of statin treatment from patients due to fear of liver or muscle damage. Other reasons were indicated much less frequently (Table II, Figure 1).
Table II
Doctors who encountered refusal of treatment with statins due to a given concern
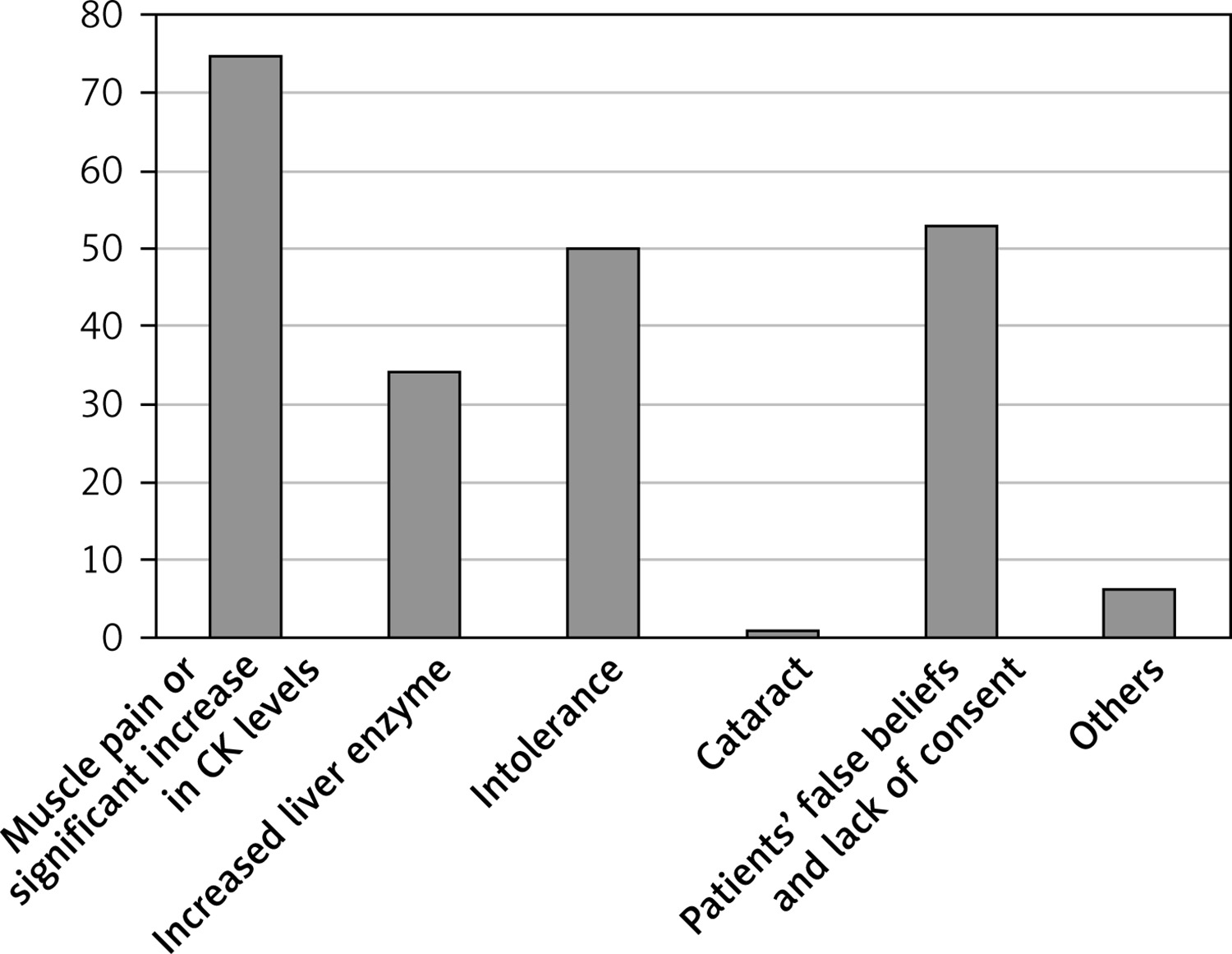
Respondents indicated that around 10–20% of patients discontinue statins on their own. More than three quarters of doctors encountered adverse effects of statins in their practice, which occurred in less than 10% of treated patients. A small proportion of patients (< 10%) required treatment discontinuation for medical reasons. The most frequently cited reasons for doctors deciding to discontinue statins were myalgia or a high increase in CK, disagreement with treatment due to misinformation about the side effects of statins, drug intolerance, and liver enzyme elevations (Table III, Figure 2). As many as 96.5% of doctors reported that they attempt to educate patients.
Comparison of results in terms of sex and work experience
The results were compared in terms of the impact of sex and seniority. A detailed summary is provided in Table IV. During the study, it was observed that doctors with longer work experience were statistically more likely to encounter side effects of statins in their patients and were more likely to report discontinuing treatment due to muscle pain or elevated liver enzymes. Physicians with the shortest professional experience (≤ 5 years) were less likely to report the experience of refusing statin treatment due to the patient’s fear of developing dementia and diabetes. There were no significant differences in patient education with a negative attitude toward statins in groups divided by sex and work experience.
Table IV
Comparison of results in terms of sex and work experience
Discussion
In the present study, the practical experience of physicians with statin therapy for dyslipidaemia patients was reviewed, mainly in terms of refusal and discontinuation of the therapy. The most common reasons for not taking or discontinuing treatment were due to patients’ fear of liver and muscle damage, which in most cases were not justified. Doctors indicated that a low percentage of patients required termination of therapy. This is confirmed by a large meta-analysis from 2022 [20], which analysed over 4 million patients using statins, and side effects occurred in only 9.1% of them. Therefore, in the remainder of this article, we have undertaken to review all the patients’ fears of statin treatment for veracity and medical justification. Many of these are misconceptions whose harmfulness must be combated. We believe that an explanation based on factual medical data will help doctors in daily practice to dispel myths and contribute to better therapeutic adherence.
One of the most common patients’ concerns about statin treatment is the fear of liver damage. Scientific reports show that this fear is unfounded. The mechanism responsible for the adverse effects of statins on the liver, causing an increase in liver enzymes, has not been fully elucidated [21, 22]. A transient increase in aminotransferase activity occurs during the first 12 weeks of treatment and usually resolves spontaneously. The increase in these enzymes does not correlate with histopathological changes and, therefore, does not meet the criteria for liver damage [23]. A review of large, randomised trials and case reports of patients treated with statins by Law and Rudnicka found that liver and biliary dysfunction during the use of these drugs was comparable to placebo [24]. A retrospective study by Smith et al. revealed a significant increase in alanine aminotransferase (ALT) and aspartate aminotransferase (AST) activity in only 1% of patients treated with statins. Charles et al. found elevated ALT activity in only 0.3% of patients who took a single statin for 4 years [25, 26]. Denus et al. conducted a meta-analysis of 13 randomised, controlled clinical trials. They evaluated almost 50,000 patients treated with statins for lipid disorders as part of cardiovascular disease prevention. The incidence of elevated serum aminotransferases was comparable in the treatment and placebo groups [27]. However, it is important to note that a contraindication to taking statins, according to the European Society of Cardiology (ESC) and European Atherosclerosis Society (EAS) guidelines, is chronic liver disease with serum ALT and AST activity exceeding three times the upper limit of normal. The guidelines recommend the determination of aminotransferases 8 weeks after starting treatment with statins or after increasing the drug dose. An increase in ALT values less than three times the upper limit of normal is not a reason to discontinue treatment [28].
Another concern of patients was muscle damage during statin treatment, which was reported by 84% of respondents. This is referred to as statin-associated muscle symptoms (SAMS). Typically, it is characterised by symmetrical pain, weakness, and cramps in the xiphoid muscles, primarily the thigh, buttock, and trunk muscles. Symptoms generally appear within 4–6 weeks of starting treatment, less frequently after a longer period of use, when it is most often due to a change in dose or the administration of another drug affecting the pharmacokinetics of statins [29]. In most cases, SAMS is not accompanied by elevated CK levels, in contrast to the most severe muscular complication, rhabdomyolysis, where a significant increase in CK 40 times above the upper limit of normal myoglobinaemia and myoglobinuria can be observed, which can lead to acute renal failure. It is a life-threatening condition that occurs infrequently, with an average of 1 per 100,000 patients treated with statins [24].
Clinical studies show that SAMS affect 7–29% of patients, which is not supported by randomised placebo-controlled blinded studies, where the percentage is much lower, ranging from 1.5 to 5% [30, 31]. In The Effects of Statins on Muscle Performance (STOMP) study involving 420 volunteers randomly allocated to test and control groups, symptoms of myalgia were reported by 9.4% of those treated with 80 mg of atorvastatin and 4.6% of those receiving placebo [32]. In other randomised trials, the frequency of SAMS was similar in both groups. Studies have been conducted using high doses of statins in patients. Not enough data were available to perform subgroup analyses based on dosage [33–35]. The risk of SAMS increases with statin dose but also with the presence of other risk factors (genetic factors, patient characteristics, and interactions with other drugs) [36].
In case of suspicion of SAMS in a patient taking statins, the physician should order a serum CK analysis. However, it should be remembered that high-intensity physical exertion, the use of drugs that inhibit the metabolism of statins (fibrates, antifungal azole drugs, macrolide antibiotics), drugs and substances that negatively affect muscle tissue (steroids, immunosuppressants and antipsychotics, i.e., steroids and antipsychotics such as haloperidol, risperidone, opioids, alcohol) are often responsible for muscle complaints or the nocebo effect [29]. The nocebo effect is related to the perception of discomfort associated as a side effect of the drug through the patient’s negative attitudes towards its use and the expectation that a particular side effect may occur [37]. The Samson study, which included 60 patients with a history of statin treatment interruption due to SAMS, assessed the above phenomenon. During the monthly periods, the subjects were randomised to alternately take 20 mg of atorvastatin or a placebo or remain pill-free. The cycle was repeated four times. The frequency of reported SAMS was similar in both groups: those receiving the drug and placebo [38].
Approximately 17% of physicians have encountered the opinion that statins cause dementia. The incidence of dementia is age-related, and with an increasingly ageing population, the number of people with dementia is steadily rising [39]. Numerous studies have been carried out to investigate the possible effects of statins on the development of dementing disorders. However, evidence from the literature indicates the opposite [40]: the use of statins has been found to have a beneficial effect in reducing the incidence of general dementia, Alzheimer’s disease, and mild cognitive impairment. This is because statins inhibit the formation of many intermediates in the cholesterol synthesis pathway. Some of these compounds are involved in the deposition of amyloid and senile plaques in the brain, responsible for Alzheimer’s disease [41]. There was also a 10-year follow-up of patients with the ApoE4/ApoE4 genotype. This study showed that the incidence of Alzheimer’s disease was significantly lower in statin users than in the control group [42]. The protective effect of statins against dementia was also supported by a large study in Taiwan, which found an inverse correlation between statin dose and risk of dementia [43].
The experience of patients’ fear of statins due to the alleged risk of erectile dysfunction was reported by 8% of doctors. Statins have been shown to improve vascular endothelial function by reducing the concentration of low-density lipoproteins that act adversely on it. As a result, nitric oxide activity in the walls of the penile capillaries increases and erectile function is improved. This effectiveness has been confirmed in several studies [44, 45]. On the other hand, statins may impair erectile function as they reduce the synthesis of testosterone. Several studies supporting this thesis can be found in the literature. Meta-analyses of randomised placebo-controlled trials addressing this topic facilitate assessment of the effect of statins on erectile function. One meta-analysis involving a review of seven studies on the effects of rosu- and atorvastatin on erection found positive effects on erection. Limitations of this meta-analysis were the small group of included patients (686) and the fact that it was characterised by high heterogeneity [46]. The Hope 3 study involving a group of 2153 patients and a follow-up period of 5.8 years was particularly significant. Rosuvastatin and its effect on erection compared with placebo were analysed. The results showed a slight improvement among patients taking statins compared to placebo [47].
Undoubtedly, the topic of the effect of statins on erectile function has not been definitively investigated, especially in light of studies reporting a decrease in testosterone levels during therapy with 3-hydroxy-3-methylglutaryl-coenzyme A reductase inhibitors and thus possible induction of hypogonadism [48, 49]. Although the meta-analyses and studies cited reveal a positive effect of statins on erectile function, there is a need for further, larger-group and well-designed placebo-controlled studies investigating this correlation.
Another myth about statins encountered by 4% of doctors was the alleged risk of cataracts during their use. Statins have not been shown to increase the risk of developing cataracts. Meta-analyses of randomised placebo-controlled trials have not proven a keratogenic effect of statins [50]. On the contrary, some studies have suggested a protective effect of statins on the risk of cataracts, but the results were not reliable enough to draw a definite conclusion. Given the significant benefits of statins in patients with cardiovascular conditions, the presumed risk of cataracts should not deter their use.
3.5% of doctors reported that they had faced refusal of treatment with statins because of patients’ fear of developing prostate cancer. Statins have not been shown to increase the risk of prostate cancer. On the contrary, according to meta-analyses of the studies published to date on this topic, statins may reduce this risk, especially that of advanced and fatal cancers [51]. It is possible that statins will be one of the therapeutic pathways for prostate cancer in the future, but further research is needed for this to reach the strength of a recommendation [52].
The fear of developing diabetes because of treatment with statins was encountered by 20% of doctors. Statins, niacin, thiazide diuretics, and β-blockers are categorised as diabetogenic drugs [18]. In the JUPITER study (Justification for the Use of Statins in Primary Prevention: An Intervention Trial Evaluating Rosuvastatin), patients treated with rosuvastatin 20 mg/dl for 1.9 years with one or more risk factors for diabetes had 28% more cases of diabetes compared with placebo. In patients without risk factors for diabetes treated with rosuvastatin 20 mg/dl, there was no increased incidence of diabetes [53]. In the SPARCL (Stroke Prevention by Aggressive Reduction in Cholesterol Levels) study, 34% of those taking statins developed diabetes within 4.9 years [34, 54]. A large retrospective cohort study from 2021 found that statin use was associated with diabetes progression, including a greater likelihood of starting insulin treatment, significant hyperglycaemia, acute glycaemic complications, and increased prescriptions for hypoglycaemic drugs. Secondary analysis showed a dose-dependent relationship, with higher statin doses linked to faster diabetes progression [55]. A 2024 meta-analysis assessed the effect of statin therapy on new-onset diabetes. It found that statins cause a modest, dose-dependent increase in the number of new-onset diabetes diagnoses. However, the adverse effects of statins on cardiovascular risk that may result from these small increases in glycemia are already accounted for by the overall reduction in cardiovascular risk seen with statin therapy in these studies [56]. During treatment with statins, patients who are obese, have elevated triglycerides, and suffer from hypertension are most at risk of developing diabetes. Patients with the above burdens are at high risk of developing diabetes even if they are not taking statins. Patients without risk factors for diabetes treated with statins did not show an increased incidence of diabetes [18, 57].
The authors are aware of the limitations of the study, which undoubtedly include the data collection methodology. The survey was distributed through a social network and the mailing database of the Polish Society of Family Medicine, but the authors are unable to provide the percentage of respondents who completed the survey from each source. This resulted in a clear overrepresentation of doctors from this specialty. Additionally, probably due to the fact that more women work in primary health care and that women are more willing to participate in surveys, men constituted only 32%. Moreover, the questions in the questionnaire were based on the subjective estimate of the respondent and did not specify the period of time to be taken into account. This contributed to the high generalization of the results. Another significant limitation was the superficially collected interview about the characteristics of the study group. There were no questions about the respondent’s place of residence and work. This prevented better comparison of results and identification of risk factors for given responses.
Doctors frequently encounter refusal of treatment with statins and discontinuation of therapy, often due to circulating misconceptions among patients that are not fully understood. We hope that the arguments cited based on factual medicine will make it easier for doctors to educate their patients. Increasing the proportion of patients properly treated for dyslipidaemia will translate into a decrease in cardiovascular mortality.
In conclusion, many misconceptions about the side effects of statins circulate among patients, often leading to refusal to start or continue therapy. In our study group, nearly 80% of the doctors interviewed had encountered refusal of statin treatment from patients due to fear of liver or muscle damage. Scientific studies clearly show that adverse effects in patients treated with statins are rare, and their incidence is comparable to the placebo group. Statins play a crucial role in the prevention of cardiovascular disease, and emphasis should be placed on educating patients and healthcare professionals to reduce misconceptions about the side effects of these drugs. One proposed solution is to create and place informational materials in the form of advertisements on television and radio. These could highlight key facts such as the significant role of lipid disorders in mortality and strategies to address them such as a healthy lifestyle and statins. Additionally, medical facilities could provide information brochures that patients could read while waiting for a medical appointment. However, doctors should have the opportunity to use reliable knowledge provided at scientific conferences and in open access articles. It is important that education is carried out on a large scale. Scientific societies such as the Polish Lipid Association and the Polish Society of Family Medicine are particularly important in the continuous education of doctors and improving their competences in the area of lipid-lowering therapy. In cases of high resistance to treatment with statins, it is worth offering patients other cholesterol-lowering substances, for example alirocumab, which, according to research, provides clinically significant reductions in LDL-C [58].