Remnant cholesterol (RC) is defined as the cholesterol carried in triglyceride-rich lipoproteins and their partially metabolized remnants that remains after the calculated or measured low-density lipoprotein cholesterol (LDL-C) and high-density lipoprotein cholesterol (HDL-C). RC was first articulated in the 1970s by Zilversmit as a crucial contributor to atherogenesis related to postprandial particles directly contributing to arterial wall injury [1]. Varbo et al. strengthened the significance of RC in 2013 through Mendelian randomization analyses that leveraged genetic variants in APOA5, LPL, and related loci to establish its role as a causal driver of ischemic heart disease. This was determined to be independent of LDL-C and mediated partially through low-grade vascular inflammation [2]. Complementary analyses anchored to triglyceride-lowering variants (e.g. loss-of-function mutations in APOC3 [3] and ANGPTL3 [4]) showed reductions in coronary heart disease proportional to lifelong reductions in triglyceride-rich lipoproteins. These findings supported the causal mediation pathway of RC and reinforced the need for therapeutic agents now in late-stage development. The biological convergence of lipoproteins driving inflammation, and inflammation amplifying lipoprotein-mediated injury is central to the pathophysiology of atherogenesis. The American Heart Association’s CKMH Presidential Advisory and Scientific Statements reframed the larger landscape, highlighting the interconnectedness of visceral adiposity, dysglycemia, kidney dysfunction, and atherosclerotic disease through overlapping biology and across the life-course – the cardiovascular–kidney–metabolic (CKM) syndrome [5]. Most U.S. adults meet criteria for CKM stages 1 to 3 [6], underscoring the scale of the prevention challenge. Yet, even with optimal LDL-C lowering, residual cardiovascular risk persists. Residual risk has two principal axes: residual cholesterol risk, and residual inflammatory risk, the latter indicated clinically by high-sensitivity C-reactive protein (hsCRP) and championed by Ridker as the obverse side of the prevention coin [7]. Both axes are mechanistically well defined, modifiable, and magnified in the CKM phenotype. The Remnant Cholesterol Inflammatory Index (RCII), defined as the multiplicative product of remnant cholesterol and CRP, attempts to capture both axes in a single, accessible biomarker, and to do so using inputs readily available in most laboratories.
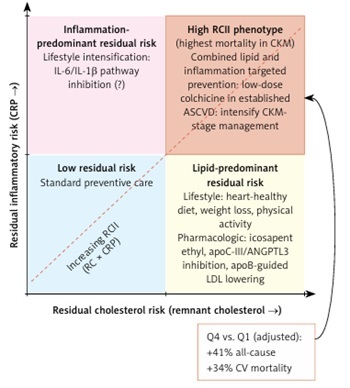
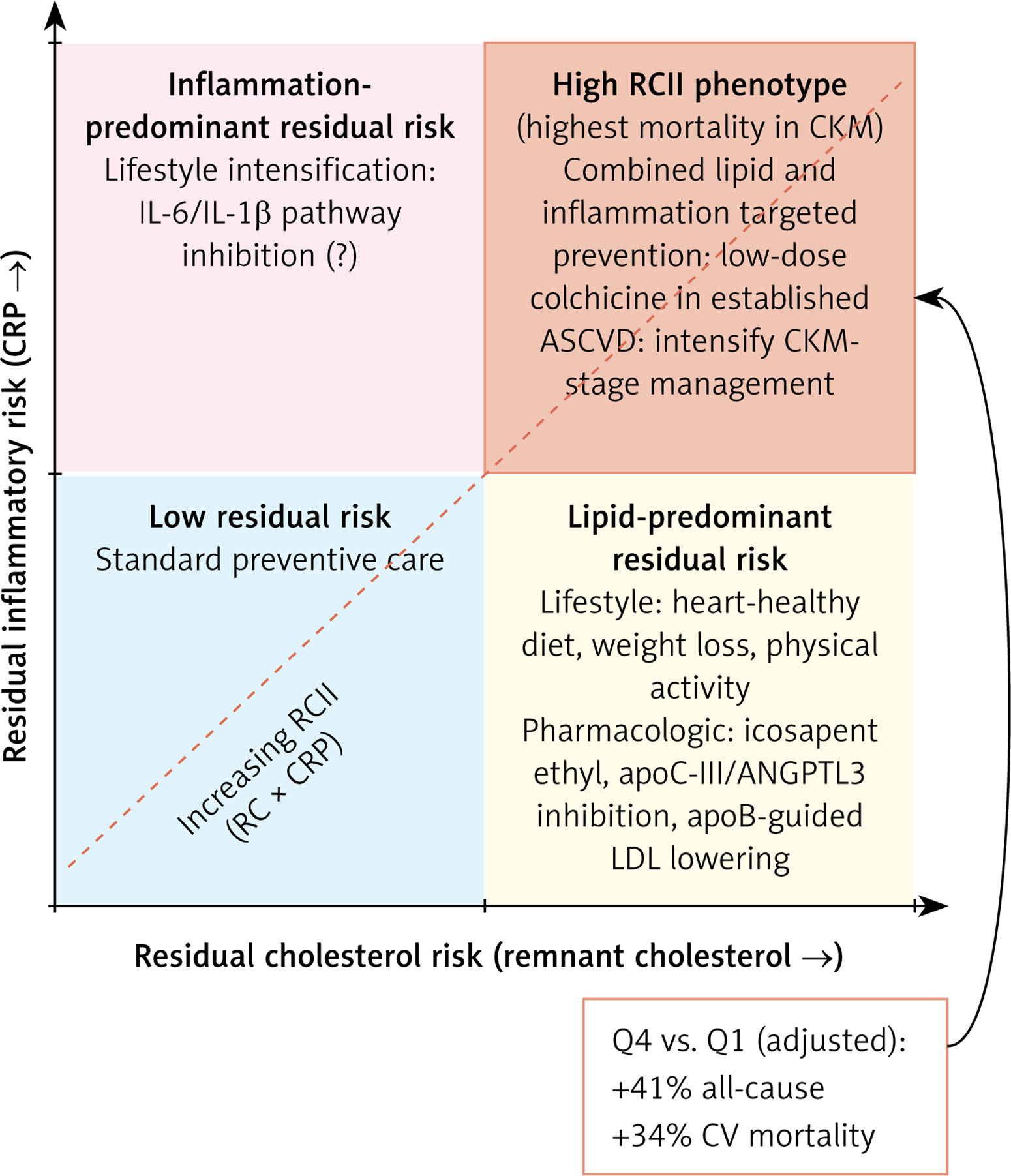
In this issue of Archives of Medical Science, Wang et al. report that a higher RCII is independently associated with all-cause and cardiovascular mortality across the full spectrum of CKM syndrome. A total of 11,917 NHANES participants followed for a median of 13 years showed that individuals in the highest RCII quartile had ~40% higher all-cause mortality risk than those in the lowest quartile after adjustment for socioeconomic status, age, sex, body mass index, and major comorbidities. This relationship was non-linear and demonstrated a threshold-like dose-response. The finding is not only statistically significant, but also clinically relevant as the analysis provides support of a parsimonious composite measure that combines complementary mechanistic pathways and supports the broader case for integrated metabolic–inflammatory phenotyping (Figure 1). The authors share several limitations of their analysis, which deserve careful attention. RC was formula-derived as a snapshot of a dynamic postprandial measure that behaves more like an area under the curve. Within the composite RCII score, the inflammatory component was represented by conventional CRP. hsCRP is commonly used in residual inflammatory-risk studies often set at a ≥ 2 mg/l threshold. Without a direct comparison to conventional CRP, it is unclear whether hsCRP provides a stronger or more clinically useful signal. The analytic participant flow figure raises another question. Over 34,000 of ~101,000 NHANES participants were excluded as they did not have CKM risk, yet recent national estimates suggest that roughly 90% of U.S. adults meet criteria for CKM stages 1 to 3 [6]. That discrepancy may reflect strict CKM definitions or methodological staging choices; however, it may affect generalizability and warrants future external validation. We agree with the authors that the most important remaining questions are pragmatic. Does RCII significantly impact PREVENT score-based risk estimation? [8]. Does it improve discrimination, reclassification, or the selection of patients for targeted interventions? Non-HDL-C has the reputation as an inexpensive, fasting-independent marker of total apoB-containing atherogenic burden [9], so would a combined non-HDL-C × hsCRP inflammatory index outperform RCII? Additional questions include whether RCII can be an actionable clinical tool through formal reclassification metrics, added to prospective cohorts with serial biomarker measurement, and/or a comparative study design.
Figure 1
Two axes of residual cardiovascular risk in cardiovascular–kidney–metabolic (CKM) syndrome. Residual cholesterol risk is demonstrated by two intertwined, yet independent biological mechanisms: 1) remnant cholesterol (RC) carried in apoB-containing triglyceride-rich lipoproteins and 2) residual inflammatory risk indexed by high-sensitivity C-reactive protein (hsCRP). The remnant cholesterol inflammatory index (RCII = RC × hsCRP) integrates both axes. The high-RCII phenotype (upper-right) carries the greatest mortality burden in CKM and aligns conceptually with combined lipidand inflammation-targeted prevention
ASCVD – atherosclerotic cardiovascular disease, CKM – cardiovascular–kidney–metabolic.
RCII is a potentially useful marker of foundational biologic pathways rather than a new discovery. In the post-statin era, operational biomarkers are changing the concept of residual cardiovascular risk with the possibility to improve staging and treatment for CKM syndrome. Cardiometabolic medicine is moving toward integrated care and team-based models. The CardioMetabolic Health Alliance proposed this framework over a decade ago [10]. In parallel, precision-prevention prioritizes equity-aware risk assessment [11]. Importantly, the World Heart Federation’s recent Roadmap on integrated care portrays cardiovascular disease as a central node within a network of long-term conditions, calling explicitly for person-centered, multidisciplinary care across the cardiometabolic spectrum [12]. A measurable composite biomarker like RCII may align with this vision: easy to measure, biologically grounded, and capable of nudging the conversation past LDL-C alone. The findings of Wang et al. in this issue urge us to consider residual cholesterol and inflammatory risk together rather than as separate problems, and to move past the silos of treating the heart, kidney, and lipid metabolism as separate organ systems [8]. The prospective application of clinical composite indices may lead to actionable approaches to comprehensive disease prevention in addition to predicting risk. Future research should consider trials of combined lipid and anti-inflammatory measures and therapeutic strategies. These efforts may determine whether a composite measure such as RCII should be incorporated into clinical decision-making and more individualized guidance of clinical care. Integrating measures of RC and inflammation: risky business, perhaps. But this is precisely the kind of risk worth taking.