Introduction
Non-alcoholic fatty liver disease (NAFLD) is a common chronic non-communicable disease (NCD) that excludes viral, alcoholic, drug-induced hepatitis and other diseases and carries an association of stigma. It is not fully explored in terms of correlations with metabolic and intra-patient heterogeneity. In 2020, experts around the world aiming to better understand the relationship between fatty liver and metabolism in the field of liver disease issued an initiative recommending that NAFLD be renamed metabolic dysfunction-associated fatty liver disease (MAFLD), which is more beneficial in diagnosing metabolic dysfunction, extrahepatic disease, and high-risk liver disease, as well as predicting liver fibrosis [1]. Worldwide, MAFLD has become a major public health issue due to the abnormal buildup of fat in the liver, which occurs even when alcohol intake is moderate [2]. Lifestyle changes and the worldwide obesity pandemic are fast increasing the incidence of this condition, which is intimately linked to metabolic diseases such diabetes, dyslipidaemia, and obesity [3]. In addition to endangering patients’ physical health, MAFLD severely affects their emotional and psychological wellbeing. Researchers and clinicians are paying more and more attention to the correlation between MAFLD and symptoms of depression [4].
Individuals’ health, social functioning, and quality of life can be profoundly affected by depression, a prevalent mental condition [5]. When it comes to MAFLD, the metabolic abnormalities might be worsened by depressive symptoms, creating a vicious cycle of worsening mental and physical health [6]. Finding modifiable risk factors for depression in MAFLD patients is, hence, of the utmost importance.
Regular physical exercise is one adjustable component. The many positive effects of physical and mental exercise on health have been known for a long time [7]. According to Sharifi [8], there is abundant research evidence showing that exercise improves health in general, including mental health issues such as depression. Nevertheless, it is still not known how exactly exercise relates to the reduction of depressive symptoms in MAFLD patients. Additionally, there has been a lack of research on the best forms and intensities of physical exercise for MAFLD patients experiencing depressive symptoms.
In order to fill these gaps in our understanding, this research analysed the relationship between the kinds and amounts of physical exercise and the risk of depressive symptoms in people with MAFLD. Our goal was to help MAFLD patients improve their physical and mental health by gaining a better knowledge of the correlation between their level of physical activity and their feelings of depression. In addition, this research may add to our general knowledge of how exercise might help with the treatment of long-term health conditions and the psychological issues that often accompany them.
Material and methods
Definition of MAFLD
The diagnostic methods that are used for the diagnosis of MAFLD include imaging investigations, blood biomarker testing, and liver biopsies. It is possible for dysregulation of the metabolic process to result in the buildup of fat in the liver. The presence of metabolic dysregulation symptoms, being overweight or obese, or having diabetes mellitus are all variables that increase the likelihood of experiencing metabolic dysfunction [2].
Evaluation of depression
According to Maroufizadeh [9], one method for determining a person’s depression level is the Patient Health Questionnaire-9 (PHQ-9). Any score between 0 and 4 indicates no depression, any score between 5 and 9 indicates mild depression, any score between 10 and 14 indicates moderate depression, any score between 15 and 19 indicates moderately severe depression, and any score between 20 and 27 indicates severe depression.
Independent variable
The Global Physical Activity Questionnaire was used to gather data on the individuals’ levels of physical activity each week [10, 11]. Researchers examined the degree of physical activity in two groups: those who engaged in moderately active leisure pursuits and those who engaged in more strenuous activities. Exercising vigorously includes any sport, fitness programme, or recreational activity that considerably increases the heart rate or breathing rate, such as running or basketball. Mildly active leisure activities included swimming, volleyball, running, or cycling for at least 10 min continuously.
According to the National Health and Nutrition Examination Survey, moderate recreational activities should be rated at 4 points, while vigorous recreational activities should be rated at 8 points. The MET for each week was determined using these results. It was possible to determine the activity’s weekly metabolic equivalent by combining the MET scores, daily duration, and number of days of physical activity.
Covariates
Several studies [12–16] have provided evidence that suggests a strong correlation between physical activity and depression. Other risk factors that have been identified include age, gender, race, smoking, and the family income to poverty ratio (PIR). When the weight was recorded in kilograms, the body mass index was calculated by dividing that number by the square of the height that was measured in metres. This particular set of parameters was selected because we believe that they have the potential to influence the link that exists between physical activity and depressive symptoms.
Statistical analysis
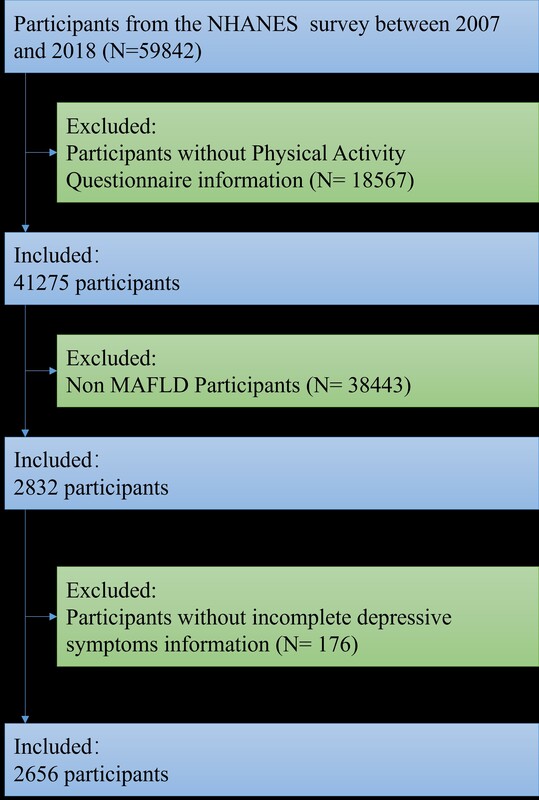
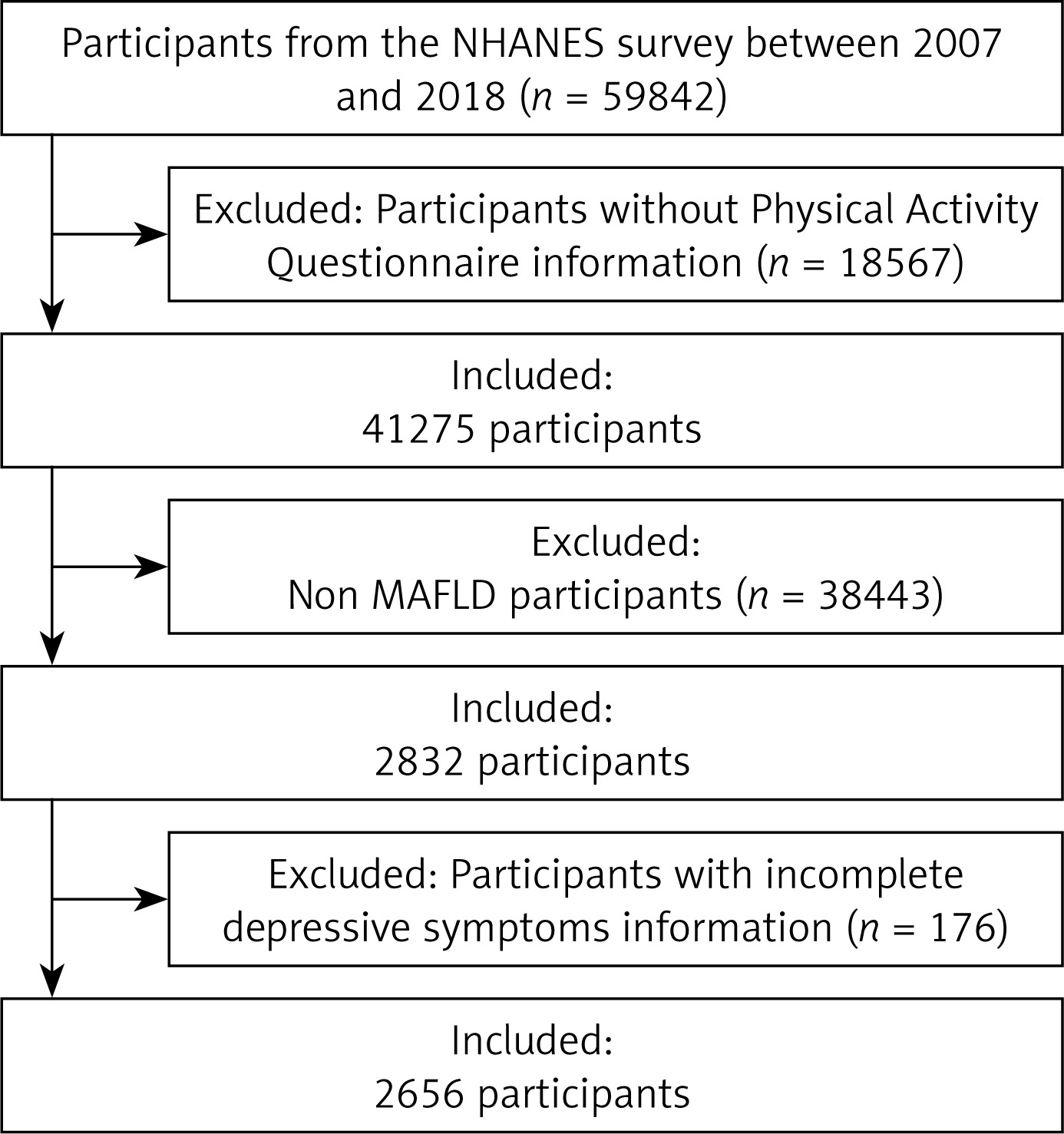
Data from the National Health and Nutrition Examination Survey (NHNES) from 2007 to 2018 were integrated using EmpowerStats version 4.1 (http://www.empowerstats.net/analysis). Figure 1 shows the flow diagram depicting the procedure for selecting research participants. Continuous variables are represented by the mean and standard error when comparing them among covariates, whereas categorical variables are represented by percentages. The National Center for Health Statistics (NCHS) Research Ethics Review Committee has approved the survey and all participants have signed an informed consent form.
For this research, we used the generalized linear model, both univariate and multivariate. Three statistical models were created for convenience: The first model did not account for any of the covariates; the second model adjusted for the commonly used demographic variables (gender, age, and race); and the third model incorporated all of the covariates listed in Table I. We evaluated the threshold and saturation effects of the link, as the study showed a nonlinear relationship. The magnitude of the influence is established in the threshold analysis by a linear relationship, or model I. But in model II, a non-linear relationship was used to compute the segment and inflection point impact sizes. We checked for differences between models I and II using the log-likelihood ratio test.
Table I
Baseline characteristics of participants
Baseline characteristics of participants
Table I shows the demographics and baseline characteristics of the research participants. There was no statistically significant difference in the age or race distribution of the population with depressive symptoms, as shown by a p-value greater than 0.05. There were more female participants and a higher body mass index (BMI) among those who showed symptoms of depression.
Moderate/vigorous recreational activities and depressive symptoms
Moderate recreational activities were negatively associated with the incidence of depressive symptoms in Models 1–3, as shown in Table II. There is a statistically significant negative correlation between the frequency of depressive symptoms and vigorous recreational activities in Models 1 and 2, but no such difference in Model 3. According to the results of the subgroup analysis, women who engaged in moderate levels of recreational activity were less likely to have depressive symptoms (Table III).
Table II
Associations between moderate/vigorous recreational activities and depressive symptoms among the MAFLD population
Exploration of nonlinear relationships
Figure 2 displays the results of a curve fitting investigation on the association between physical activity levels and the likelihood of experiencing depressive symptoms. Table IV shows the outcomes of a log-likelihood ratio test that was performed on both the linear regression model and the two-segment linear regression model at the same time. The p-value was less than 0.001. When fitting, a two-part linear regression model is necessary. Our two-segment linear regression model and recursive approach both pointed to 3 as the inflection point. To determine confidence intervals for thresholds, the bootstrap resampling method was used. We hit a turning point at 3. Statistically, there was a 16.3% reduction in the chance of depressive symptoms for every unit increase in physical activity levels; this link was significant (p < 0.001). The effect size and 95% confidence interval were 0.837 (0.777, 0.902) to the left of the inflection point. On the right side of the inflection point, the effect size, 95% CI, and p-value were 1.002 (0.997, 1.007), suggesting that there was no association between the risk of depressive symptoms (p = 0.365) and each unit increase in physical activity levels.
Figure 2
Association between physical activity levels and depressive symptoms
Note: A solid rad line represents the smooth curve fit between variables. Blue bands represent the 95% of confidence interval from the fit. All variables were adjusted for age, gender, race, body mass index, smoking status and family PIR.
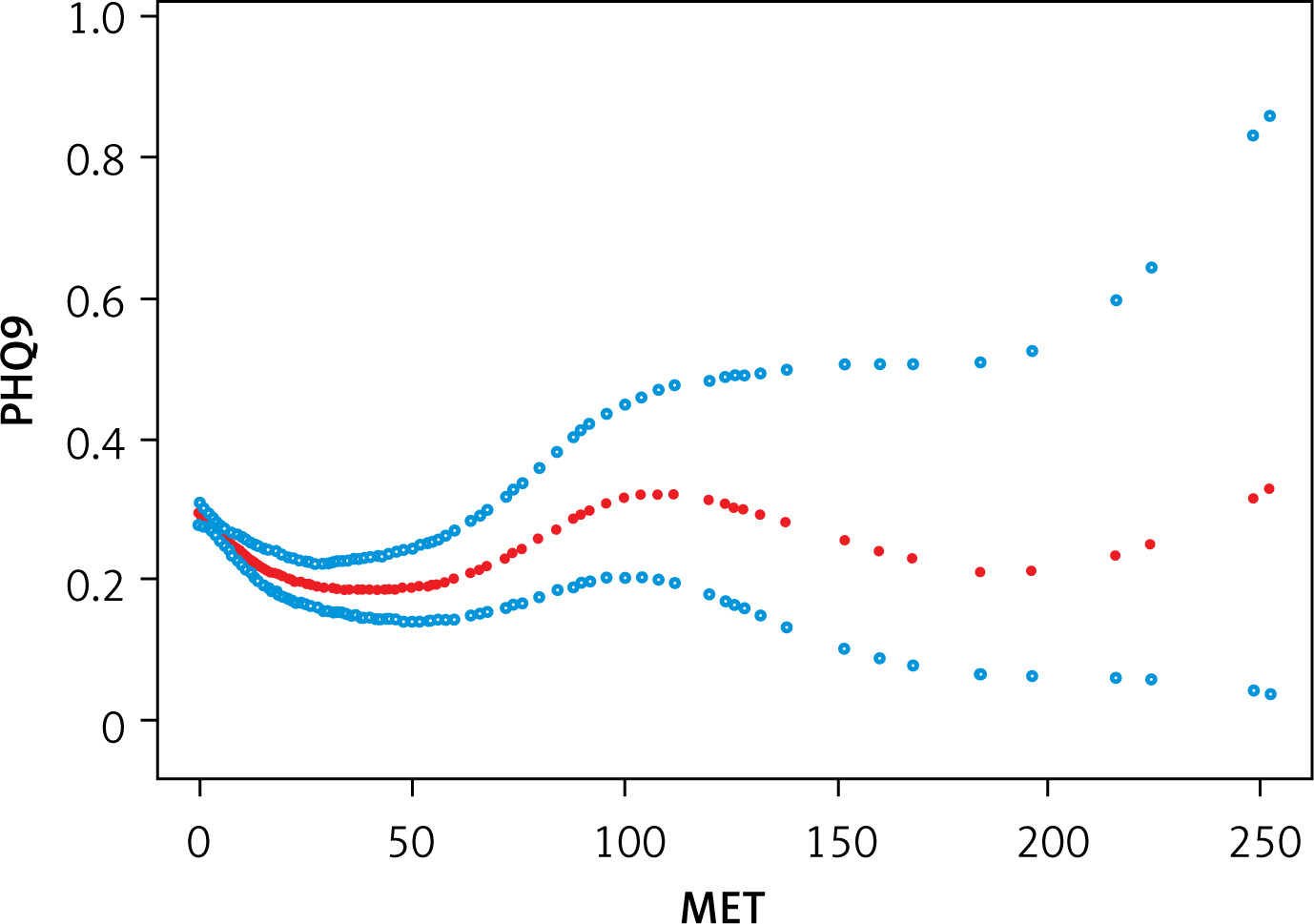
Table IV
Results of the two-piecewise linear regression model
Discussion
We discovered a non-linear relationship between levels of moderate recreational activities and depressive symptoms in the MAFLD sample in this epidemiological study of American adults. Unlike intense recreational activities, moderate recreational activities are associated with a lower incidence of depression symptoms.
There were 2656 people who took part in this survey. As people’s lives have changed in recent years, the participation rate in athletic activities has become more and more negative. Table I shows that there is a correlation between depressive symptoms and BMI, family PIR, gender, and smoking status. Depression is linked to several ailments, according to previous research. Young people with lower levels of education and smoking are at a higher risk, according to a study [17].
Many studies have shown that regular physical exercise both prevents depression and helps relieve its symptoms; therefore engaging in moderate leisure activities is an effective way to improve health [18]. According to this research, mild forms of recreational activity alleviated depressive symptoms, but strenuous forms of recreation did not. The frequency of depressive symptoms did not show significant differences according to moderate levels of recreational activities and male sex when subgroup analysis was performed on the female and male populations of MAFLD. One possible explanation is that there is a lack of research on the optimal frequency, intensity, duration, and type of walking interventions, even though moderate recreational activities like walking have been found to significantly improve depressive symptoms in some populations [19]. Behavioural activation theory suggests that depressive symptoms may be alleviated when people replace passive activity with recreational activities [20].
Based on the findings of this research, it is recommended that moderate recreational activities be classified as protective variables linked with mental health issues in the community of people with MAFLD. Furthermore, they are able to construct appropriate exercise prescriptions depending on the requirements of each person and/or the pathological problems that they are experiencing. This includes the participation of sports scientists and PA specialists from health institutions.
The fact that the sample only contained data from the United States is one of the limitations of this study. In the future, additional data from other countries should be added for analysis, and this constraint should be taken into consideration.
In conclusion, the purpose of this study was to investigate the impact of various levels of recreational activity on depressive symptoms in individuals diagnosed with MAFLD. The findings of this study revealed that moderate recreational activities had a protective effect on depressive symptoms, whereas vigorous recreational activities did not have a protective effect on depressive symptoms.
Chenghui Wang and Tong Zhou are the first author. These authors contributed equally to this work.