Introduction
End-stage renal disease (ESRD) is an important complication of diabetes, which is the leading cause of ESRD worldwide [1–6]. Diabetes is the most common endocrine disease in the world, and hyperglycaemia is the leading cause of hospitalisation of patients with diabetes [7]. Diabetes has many complications that lower the quality of life, like ESRD [8–10]. It has been indicated by many researchers that chronic kidney disease can increase the risk of cardiovascular death [1, 2]. In a meta-analysis of 39 studies and 1,371,990 patients, Tonelli et al. showed that chronic kidney disease causes a higher risk of death, depending on the stage of renal failure [4]. Among patients treated with renal replacement by haemodialysis, deaths are 13–15 times more frequent compared to deaths in non-dialysed patients in the control group [11]. Mortality in patients with ESRD is higher in men than in women, and it prevails in the African-American group of patients [12]. The occurrence of diabetes and obesity in patients with chronic renal failure also increases the risk of death in this group of patients [13, 14].
In the available scientific literature, there are no publications that compare the all-cause mortality in patients with ESRD in the two subgroups of diabetic and non-diabetic patients. Our study involved an analysis of the all-cause mortality in patients with ESRD with diabetes and without diabetes in 2012 compared to general mortality in patients with ESRD in Poland in 2011–2013.
Material and methods
The authors of this article performed a retrospective, population-based study using database records of the Polish National Health Fund. Subject to analysis were data on patients with diabetes or ESRD in 2011, 2012, and 2013, which were compared to the general population in Poland, and additionally data on two subpopulations of patients: patients with diabetes and patients without diabetes, in 2012. Incidence rates were calculated on the basis of the number of patients with diabetes or ESRD and relevant census data. Besides the data from the National Health Fund (NHF), demographic data for the general population of Poland were obtained from the Central Statistical Office in Poland (Central Statistical Office, 2016). End-stage renal disease often requires hospitalisation or various forms of dialysis; therefore, an analysis of hospitalisation cases can provide a good estimate of the incidence of ESRD.
Healthcare services in Poland are financed by the NHF pursuant to the binding act [15] and the regulations of the Minister of Health arising from the act [16, 17]. Healthcare services are provided within the framework of outpatient treatment and inpatient treatment, i.e. hospital care. Provision of healthcare services is described in detail in the regulations of the President of the NHF [18, 19]. In order to conduct an epidemiological analysis for this paper, patient information from the NHF database was used. The Polish National Health Fund settles and pays for health services provided to the patient by healthcare providers. In the database covering the period from 1.01.2011 to 31.12.2013, reports on ESRD according to the International Classification of Diseases (ICD-10): N18.0 – end-stage renal disease (ESRD) were found for the year 2011, 2012, and 2013. The Polish NHF database precludes the distinction of dialysis and non-dialysis patients with ESRD. Furthermore, reports on diabetes-related healthcare services were found in the resources of the fund for the period from 1.01.2012 to 31.12.2012. The main diagnosis in these reports was “diabetes” with the following extensions: E10.X – insulin-dependent diabetes, E11.X – non-insulin dependent diabetes, E12.X – diabetes associated with malnutrition, E13.X – other unspecified forms of diabetes, and E14.X – unspecified diabetes, or at the same time a patient bought medicine from any of these groups: A10A.X (insulin), A10B.X (oral antidiabetic drugs), specialised diagnostic tests. The dates of patient deaths were obtained from the Central List of the Insured.
Statistical analysis
The data were analysed using PQStat 1.6 statistical software of the Polish company PQStat Software. Additionally, Student’s t-test was applied for independent groups. Odds ratio (OR), confidence interval, and statistical significance were also calculated. The differences were considered significant at the 95% confidence level (p < 0.05).
Results
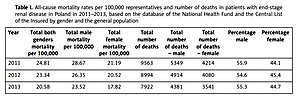
According to the data obtained from the Central Statistical Office, there were 38,501,000 people living in Poland in 2011, including 18,432,000 men and 20,069,000 women. In 2012 the number of inhabitants amounted to 38,533,789 people, including 18,651,441 men and 19,882,348 women. In 2013 there were 38,793,441 people living in Poland, including 18,629,535 men and 20,163,906 women [20]. The number of patients with diabetes in Poland in 2012 amounted to 2,227,453, including 975,364 men and 1,252,089 women. 36,306,336 people in Poland did not suffer from diabetes in 2012, including 17,676,077 men and 18,630,259 women [21]. The total male mortality rate per 100,000 representatives and total male number of deaths were higher in all years than the female mortality rate (Table I) in patients diagnosed with ESRD by gender in 2011, 2012, and 2013. A comparison between the all-cause mortality in diabetic patients with ESRD (ICD-10: N18.0 and E10-E014.X) and the non-diabetic population in Poland in 2012 showed significant differences between populations of diabetic and non-diabetic patients. No diabetes was found in 53.24% of male and female patients who died of ESRD. 51.94% of those who were diabetic and died of ESRD were men, whereas 43.3% of those who were non-diabetic and died of ESRD were women.
Table I
All-cause mortality rates per 100,000 representatives and number of deaths in patients with end-stage renal disease in Poland in 2011–2013, based on the database of the National Health Fund and the Central List of the Insured by gender and the general population
Female diabetic and non-diabetic patients were older at the time of death than male diabetic (p < 0.001) and non-diabetic (p < 0.001) patients. At the time of death male diabetic patients were younger than male non-diabetic patients (p < 0.001), but female diabetic patients were older at the time of death than the non-diabetic female patients (p < 0.001) (Table II).
Table II
The number of deaths in diabetic and non-diabetic patients with end-stage renal disease (ESRD) in Poland in 2012 by gender, based on the National Health Fund and the Central List of the Insured
| Parameter | Patients with ESRD with diabetes | Patients with ESRD without diabetes | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| Number | 2026 | 1871 | 2888 | 2209 |
| Percentage | 52.0 | 48.0 | 56.7 | 43.3 |
| Age (median) | 68.0 ±11.2* | 73.0 ±11.5* | 69.0 ±14.2* | 72.0 ±13.9* |
| Age (average) | 67.5 (95% CI: 67.0–67.9) | 70.8 (95% CI: 70.3–71.3) | 67.1 (95% CI: 66.6–67.6) | 69.1 (95% CI: 68.6–69.7) |
In the age group up to 44 years, death occurred three times more frequently in male non-diabetic patients than in male diabetic patients. In the same age group death was two times more frequent in female non-diabetic patients than in female diabetic patients (Table III). Table IV presents all-cause mortality rates for people with ESRD with diabetes per 100,000 representatives of the general population in Poland in 2012 and for non-diabetic patients per 100,000 representatives of the general population in Poland in 2012, having subtracted the number of people with diabetes. The all-cause mortality rate for diabetic patients was significantly higher than all-cause mortality for both male and female non-diabetic patients, p < 0.0001. It was found that mortality was significantly higher, p < 0.0001, in male patients as compared with female patients, for both diabetic and non-diabetic patients (Table IV).
Table III
Percentage rates in age groups for all-cause mortality in males and females in diabetic and non-diabetic patients with end-stage renal disease in Poland in 2012, based on the databases of the National Health Fund and the Central List of the Insured
| Age range [years] | Patients with diabetes (%) | Patients without diabetes (%) | ||
|---|---|---|---|---|
| Male | Female | Male | Female | |
| < 44 | 1.41 | 1.09 | 4.76 | 2.57 |
| 45–64 | 28.51 | 15.69 | 25.82 | 17.40 |
| 65–74 | 29.79 | 26.31 | 24.84 | 36.06 |
| > 75 | 40.29 | 56.91 | 44.58 | 43.97 |
Table IV
All-cause mortality rates for diabetic and non-diabetic patients with end-stage renal disease in Poland in 2012 by gender and per 100,000 representatives of the general population, based on the databases of the National Health Fund and the Central List of the Insured, having subtracted patients with diabetes
| Patients with diabetes | Patients without diabetes | ||
|---|---|---|---|
| Male | Female | Male | Female |
| 147.59 ±29.07* | 105.13 ±26.77* | 9.58 ±6.29* | 6.87 ±2.27* |
Discussion
89,009 people died in the United States of America (USA) in 2013 of ESRD, which gives an average mortality rate of 27.91/100,000 representatives of the general population [22]. 20–25% of patients with ESRD die in the USA on an annual basis, whereas 35% of patients survive for 5 years. However, only 3% of patients with ESRD and kidney transplantation die within 5 years [23].
Our study showed that the average all-cause mortality rate for male and female patients with ESRD in Poland in 2011 was 17.66/100,000 of the representatives of the general population, and in 2012 it was 15.89/100,000 representatives of the general population. In 2013 the mortality rate was 12.50/100,000 of the representatives of the general population. Over 3 years a decrease by 30% in the all-cause mortality in people with ESRD was observed in Poland.
Hoffman et al. proved that the impact of diabetes on survival after ESRD is time-dependent, but they did not prove the differences between sexes. In our study males up to 74 years of age with ESRD and diabetes had a higher mortality rate than females. An interesting result is that women older than 75 years had a higher mortality rate than men (Table III) [24]. Navaneethan et al. reported an increased risk for all-cause mortality among patients with diabetes and chronic kidney disease, who had HbA1c levels < 6%, and among those who had HbA1c levels ≥ 9%, but they do not compare the mortality with non-diabetic patients [6].
Tonelli et al. presented a meta-analysis of 39 studies from around the world and showed that the occurrence of end-stage renal disease increases the risk of death from 38% to 1100% [4].
De Jager et al. reported that death was 13–15 times more frequent in patients treated with haemodialysis as compared to the control group [11].
Janeczko et al. presented data on mortality rates for 26 years of observation of patients with type 2 diabetes as compared to mortality rates for representatives of the general population, and they showed that the standard mortality rate for men with diabetes and kidney diseases was 20 times higher, and for the same group of women it was 18 times higher, than the standard mortality rate for the representatives of the general population [25]. Małyszko et al. reported that cardiovascular death was more frequent in patients with chronic renal failure [26]. Rutkowski et al. revealed that 53.5% of patients on dialysis in Poland die of cardiovascular diseases [27]. Gurm et al. observed that out of 55,189 patients with acute coronary syndrome, including 579 patients with renal replacement therapy (haemodialysis), 13% of the dialysed patients and 4.8% of those who did not receive renal replacement therapy died [28].
In the USA, 50% of patients with end-stage renal disease die of cardiovascular diseases [29]. In the USA the mortality rate for patients with chronic renal failure, as opposed to end-stage renal disease, amounted to 117.9/1000 patients in 2013, whereby the rates for men and women were 128.7/1000 patients per year and 110/1000 patients per year, respectively [29].
Other researchers reported the death rate in patients with end-stage renal disease who were treated with haemodialysis at the level of 22% in the United States, 16% in Europe, and 7% in Japan [30, 31]. Having observed 3702 patients aged over 77 years of age, Kurella-Tamura et al. reported a mortality rate for renal replacement therapy patients per year at 58%. For this group of patients, mortality per year in the pre-renal replacement period was 13% [32].
Foley et al. reported that the mortality rate in male diabetic patients with end-stage renal disease was 30 times higher as compared to the mortality rate in the general population. Nine per cent of patients with end-stage renal disease died of cardiovascular diseases [1].
In our study all-cause mortality rates for female and male diabetic patients with end-stage renal disease in Poland in 2012 were more than 15 times higher than the all-cause mortality rate in non-diabetic patients with ESDR. All-cause mortality rates for patients with ESRD in Poland in 2012 per 100,000 representatives of the general population are presented in Table I. Various complex haemodynamic and metabolic factors, such as renal failure, age, hypertension, diabetes, lipid disorders, and lack of physical exercise, contributed to the increased risk of cardiovascular death [33–36].
Our research had certain limitations that prevented the determination of the cause of chronic renal failure, type of diabetes, metabolic control of diabetes, and occurrence of hypertension. The study was a retrospective study on patients reported to the Polish National Health Fund.
The study is a unique comparative study on all-cause mortality in patients with ESRD conducted on two cross-sectional groups: patients with diabetes and patients without diabetes.
Our research is based on the reported diagnoses of end-stage renal disease in Poland in 2011–2013. It is original and unique because it shows how the occurrence of diabetes can affect the all-cause mortality in patients with end-stage renal disease. The results of the study show the necessity to intensify healthcare for diabetic patients to prevent the development of complications of diabetes and related problems.
In conclusion, mortality rates for people with ESRD in Poland in 2012 were higher for men than for women in the general population and both in the group of diabetic and non-diabetic patients. Mortality rates for diabetic men and women with ESRD in Poland in 2012 were 15 times higher than mortality rates for non-diabetic men and women with ESRD. Special attention should be paid to the prevention and treatment of diabetes as ways of increasing life expectancy of patients with ESRD.