Introduction
Acute respiratory distress syndrome (ARDS) is a common clinical syndrome of acute respiratory failure as a result of diffuse lung inflammation and edema. ARDS can be precipitated by a variety of causes [1]. The injury of pulmonary vascular endothelial cells is an important pathological change in the early stage of ARDS [2]. Endotoxin, inflammatory mediators and physical trauma can all cause endothelial cell damage. It is a clinical syndrome of diffuse lung inflammation and edema, usually leading to acute respiratory failure [1, 3]. ARDS is an acute lung injury induced by risk factors such as pneumonia, non-pulmonary infection, trauma, blood transfusion, burns, aspiration, or shock [4]. At present, there is no single examination to identify or exclude diagnosis, largely due to the heterogeneity of ARDS, manifested in its causes, manifestations, and response to treatment [5, 6]. ARDS is a syndrome, not a specific pathological entity, currently identified only by clinical criteria, and diagnosis requires the presence of new or worsening respiratory distress and bilateral chest imaging abnormalities for 7 days or less [7].
Although some ARDS triggers can be self-limiting, while others do not have specific treatments, timely identification and treatment of reversible damage (such as infection, type I hypersensitivity) are essential [3]. Inflammatory factors play an important role in the occurrence and development of ARDS, but there is currently no unified research on the specific magnitude of their impact and whether they have the potential to serve as biomarkers. However, studies have shown that IL-1β can increase endothelial permeability by inhibiting the transcription of VE cadherin [8]. The IL-18 levels in ARDS patients with sepsis are significantly higher than those in patients with sepsis alone, indicating that IL-18 in sepsis is a key cytokine leading to lung injury [9, 10]. In a randomized controlled trial, it was also found that plasma IL-18 levels were associated with mortality in sepsis-induced ARDS [11]. The research results indicate that inflammatory cytokines play a crucial role in the development of sepsis-induced lung injury, and they synergistically interact to promote the progression of inflammation [12].
Metabolomics can reveal the correlations between metabolites or metabolic pathways and physiological and pathological changes, providing new information for the study of disease mechanisms [13]. Multiple studies have shown that metabolites and metabolic pathways are closely related to ARDS, and metabolic disorders often occur in ARDS patients [14, 15]. In the early stages of ARDS, neutrophils migrate from the pulmonary vascular system to the air chamber and can release various harmful metabolic mediators, including reactive oxygen species, proteases, and pro-inflammatory lipid-derived mediators such as prostaglandins and leukotrienes [16]. Plasma metabolites, as small molecules in human blood components, play an important role in human health. They are direct or indirect products of various metabolic activities in the body, encompassing all chemical changes that support life, including energy production, construction of essential substances, and waste disposal [17]. Abnormal levels of these metabolites can reflect oxidative stress and inflammatory status [18],
Mendelian randomization (MR) analysis is an effective method for evaluating potential causal relationships between exposure and outcomes using genetic variation as an instrumental variable (IV). Compared with traditional observational studies, MR analysis is relatively independent of unmeasured confounding factors and can significantly reduce confounding effects. Mediation analysis is used to evaluate the impact of exposure on results through mediation [19]. This study conducted MR analysis based on publicly available genome-wide association studies (GWAS) to evaluate the causal relationship between inflammatory cytokines, plasma metabolites, and ARDS risk, and demonstrated that the pathway from inflammatory cytokines to ARDS is mediated by plasma metabolites.
Material and methods
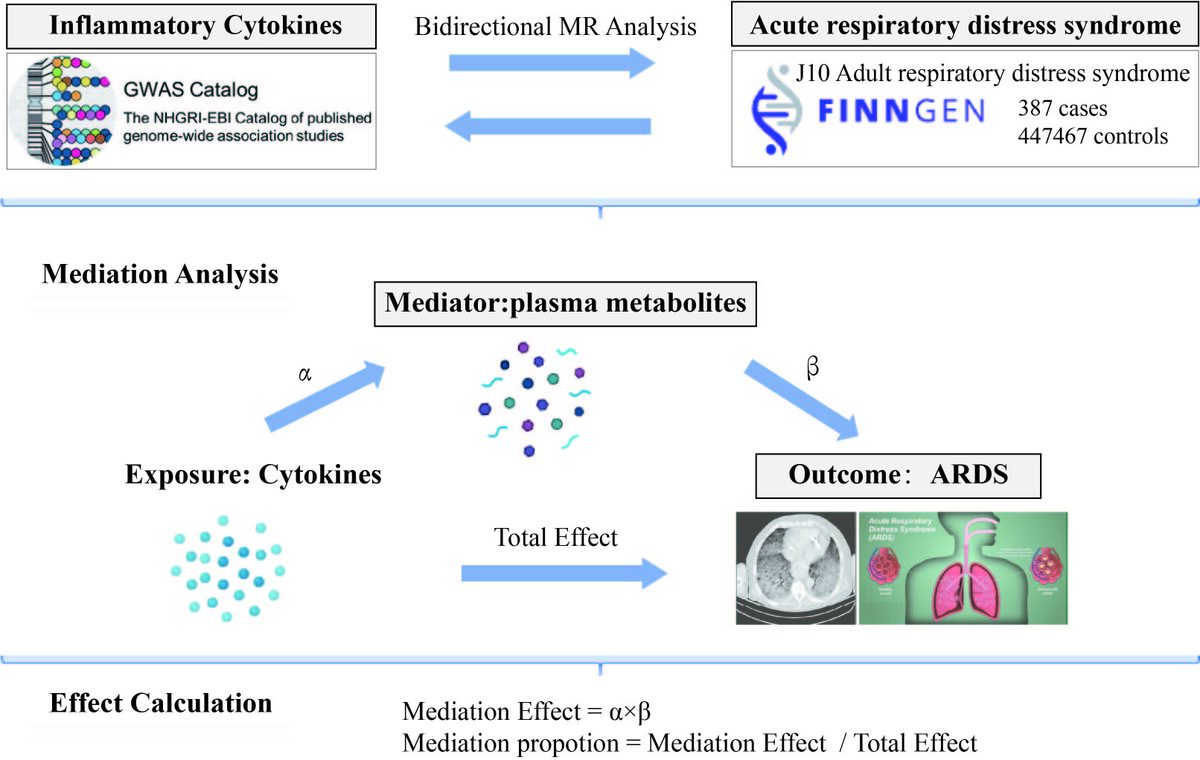
Hypothesis diagram illustrating the causal relationship between inflammatory factors and ARDS
This study has two main components, as shown in Figure 1: (1) MR analysis of 41 inflammatory cytokines on ARDS and reverse MR analysis of ARDS on 41 inflammatory cytokines (Step 1 of Figure 1); (2) mediation analysis to assess the role of plasma metabolites in cytokine-mediated ARDS in 1900 (Figure 1, Step 2). Single nucleotide polymorphisms (SNPs) were defined as IVs. SNP refers to the variation of a single nucleotide in the genome, which is the most common form of genetic variation in the genome. SNPs are widely distributed throughout the genome and can be used to study the relationships between genes, traits, and diseases. MR analysis is based on three core assumptions: the IV is strongly associated with exposure factors; the IV is not associated with confounding factors; the IV affects the outcome only through the exposure, and not by any other pathway.
Data source
The genetic data of cytokines come from the latest summary statistics of a GWAS database, in which Zhao et al. sorted and analyzed the genome-wide genotypes of 14,824 participants with European ancestry, including 91 circulating inflammatory cytokines [20]. The ARDS data were obtained from the FinnGen J10 Acute Respiratory Distress Syndrome summary dataset. This dataset can be accessed at https://www.finngen.fi/en, including 387 cases of ARDS and 44,7467 participants. Data for 1400 metabolites were obtained from the research of Chen et al. in the GWAS database [21], which includes 1091 blood metabolites and 309 metabolite ratios.
Tool variable selection
SNPs associated with certain risk factors in GWAS can be used as IVs to test their causal effects on different outcomes. The selection of IVs is based on three key assumptions: IVs must be significantly correlated with exposure; IVs cannot be associated with any known confounding factors that may alter the association between exposure and outcomes; IVs must be independent of the outcome and can only affect the outcome through their impact on exposure. The relationships between exposure and outcome examined in this study included the following four types: bidirectional MR analysis of inflammatory cytokines in ARDS, MR analysis of inflammatory cytokines to plasma metabolites, and MR analysis of plasma metabolites to ARDS. To replace exposure factors, we first selected SNPs (p < 5 × 10–8) significantly correlated with exposure factors as the threshold. In order to maximize the accuracy of IVs for each exposure factor, we removed some weak instrumental variables using F-statistic > 10 as the standard [22, 23], and selected SNPs that could accurately simulate exposure (inflammatory factors, plasma metabolites, and ARDS). Linkage disequilibrium (LD) means that the allele distribution of two or more SNP loci in a population does not meet the expected independent distribution; that is, some alleles tend to be inherited together rather than independently distributed. Finally, we excluded SNPs with LD in MR analysis, and the LD of SNPs closely related to exposure factors should meet R2 < 0.001 and distance > 10000 kb. To ensure that each IV is aligned with the same effector allele, exposure and outcome data were cross checked, and palindromic SNPs were removed prior to analysis. The palindromic SNPs are SNPs with A/T or G/C alleles.
MR analysis
Phase one
To estimate the causal effect of inflammatory cytokines on ARDS, we conducted bidirectional MR analyses separately. The inverse variance weighting (IVW) method is a fundamental analytical approach [24]. Results are considered statistically significant when the IVW P-value is less than 0.05 and the direction of effect is consistent across MR Egger, weighted median, simple mode, and weighted mode. MR results are reported as odds ratios (ORs) and corresponding 95% confidence intervals (CI). To evaluate the reverse causal relationship between ARDS and inflammatory cytokines, we used ARDS as the “exposure” and inflammatory cytokines associated with ARDS as the “outcome” to conduct MR analysis. SNPs significantly associated with ARDS (p < 5 × 10–8) were selected as IVs for MR analysis. Based on the P-value of IVW greater than 0.05, the inflammatory factors identified in the forward MR analysis were further identified as exposure factors for ARDS.
Phase two
Through bidirectional MR analysis, inflammatory cytokines with significant causal effects on ARDS were included in further mediation analysis. Furthermore, we investigated whether plasma metabolites have a causal effect on ARDS. Immediately, we conducted multiple two-step MR analyses to explore whether plasma metabolites are mediating factors in the pathway from inflammatory cytokines to ARDS. The coefficient product method was used to evaluate indirect effects, and the standard error of indirect effects was determined using the delta method [25].
Sensitivity analysis
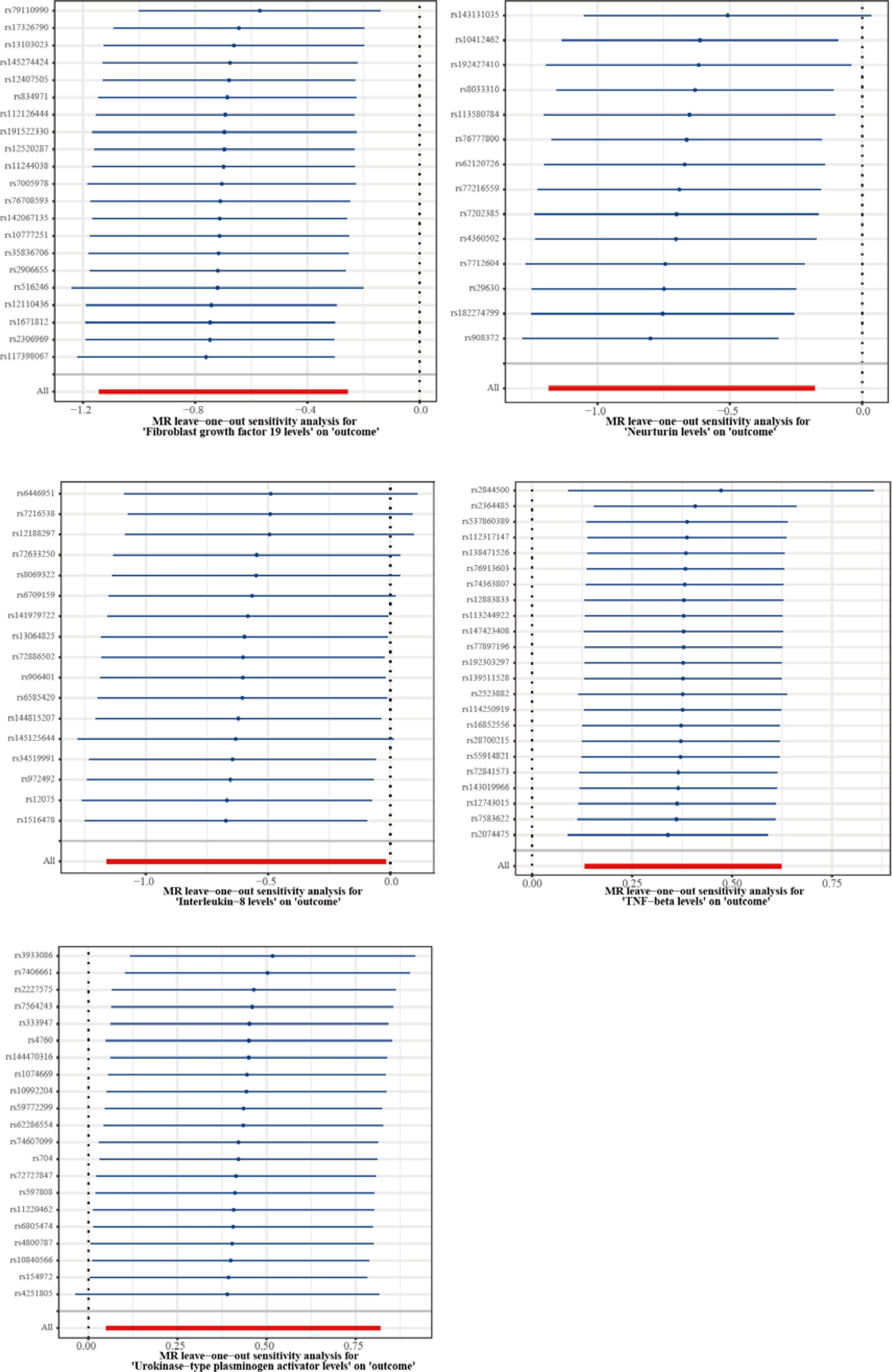
Cochran’s Q test was conducted to evaluate the heterogeneity of each SNP [26], and scatter plots of SNP–exposure and SNP–outcome associations were generated to visualize the test results. Leave-one-out analysis was performed to evaluate whether each SNP would affect the results (by sequentially excluding each SNP and performing IVW on the remaining SNPs to assess the potential impact of specific variants on the estimated values) [27]. Furthermore, we used MR Egger regression to test and correct for potential horizontal pleiotropy.
All analyses were conducted using R (v4.3.3) statistical software. MR analysis was performed using the R software package ‘TwoSampleMR’.
Results
Association between inflammatory cytokines and risk of ARDS
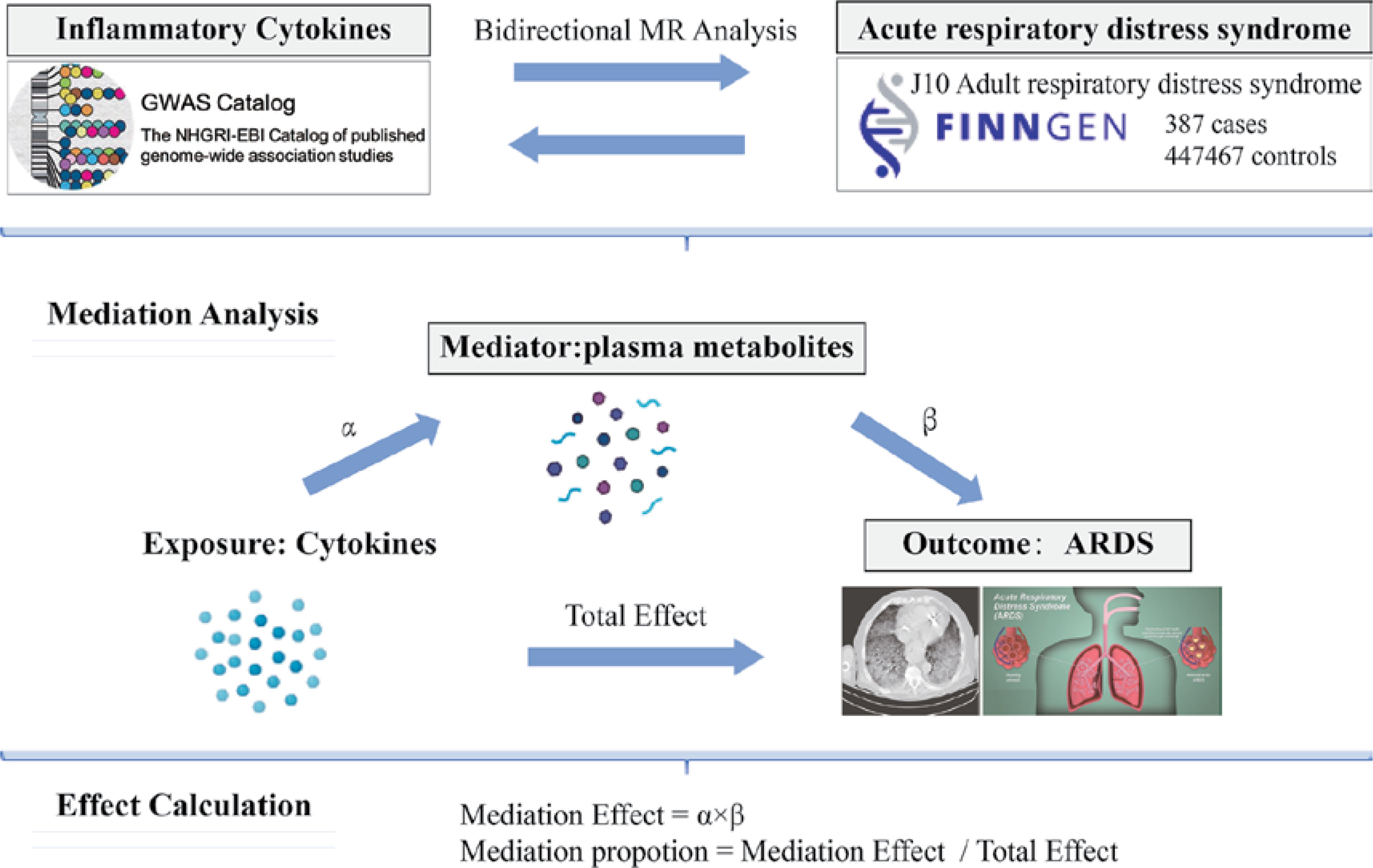
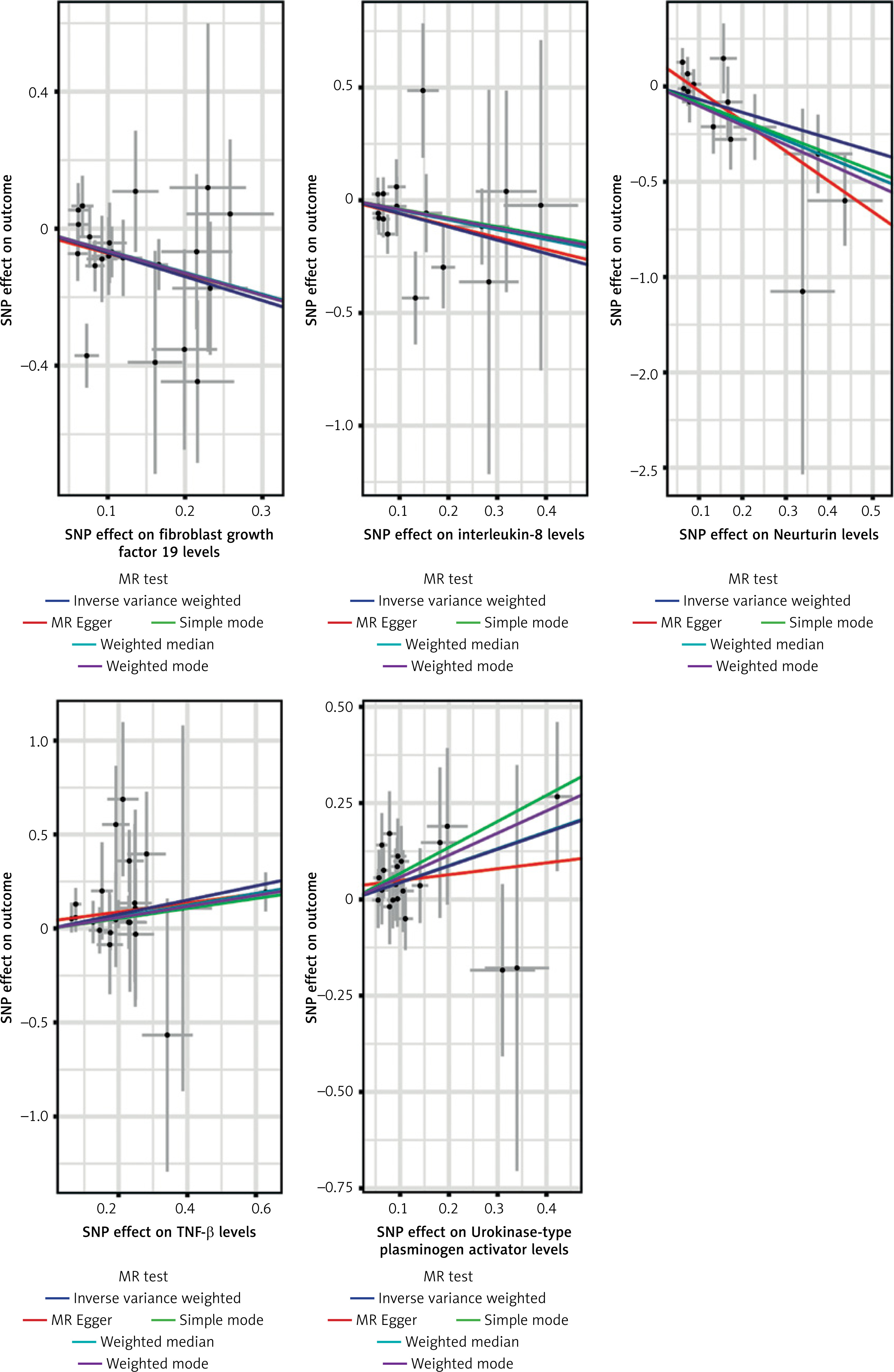
Supplementary Table SI shows the SNPs included in the regional target analysis of inflammatory cytokines. According to the above screening threshold, the F-statistic of all SNPs obtained was greater than 10, indicating a low risk of weak instrument bias. After removing palindromic SNPs, a total of 1597 SNPs were used as IVs. Next, we used these SNPs as IVs representing inflammatory cytokines as the “exposure”, with ARDS as the “outcome” for MR analysis. IVW was used as the primary method, and MR Egger, weighted median, simple mode, and weighted mode served as auxiliary methods for sensitivity analysis. The IVW results showed that fibroblast growth factor 19 levels (OR = 0.497, p = 0.002), interleukin-8 levels (OR = 0.555, p = 0.043), and neurturin levels (OR = 0.506, p = 0.008) were significantly negatively correlated with ARDS; TNF-β levels (OR = 1.459, p = 0.003) and urokinase type plasminogen activator levels (OR = 1.544, p = 0.027) were significantly positively correlated with ARDS (Figures 2, 3). In the MR analysis of ARDS, the Cochran Q test results for these 5 inflammatory cytokines showed no heterogeneity in IVs in the MR analysis. No significant intercept was observed in the MR Egger test results, confirming the absence of pleiotropy bias in IVs in MR analysis (Figure 4, Supplementary Tables SII and SIII). In addition, the leave-one-out method demonstrated the robustness and reliability of our research results, as no single SNP had a significant impact on the results (Figure 5). ARDS was treated as an “exposure”, and 1154 SNPs related to ARDS were obtained as IVs (Supplementary Table SIV). The 91 inflammatory cytokines were designated as “outcomes” according to the above SNP screening criteria. Reverse MR analysis was performed, and the results showed that there was no reverse causal relationship between the genetic prediction of ARDS and the inflammatory cytokines obtained from forward MR analysis. However, there was a significant positive correlation between ARDS and tumor necrosis factor ligand superfamily member 12 levels, monocyte chemoattractant protein-4 levels, neurotrophin-3 levels, C-X-C motif chemokine 9 levels, β nerve growth factor levels, and C-C motif chemokine 19 levels (Supplementary Table SV).

Two-step correlation analysis of inflammatory cytokines mediating ARDS through plasma metabolite pathway
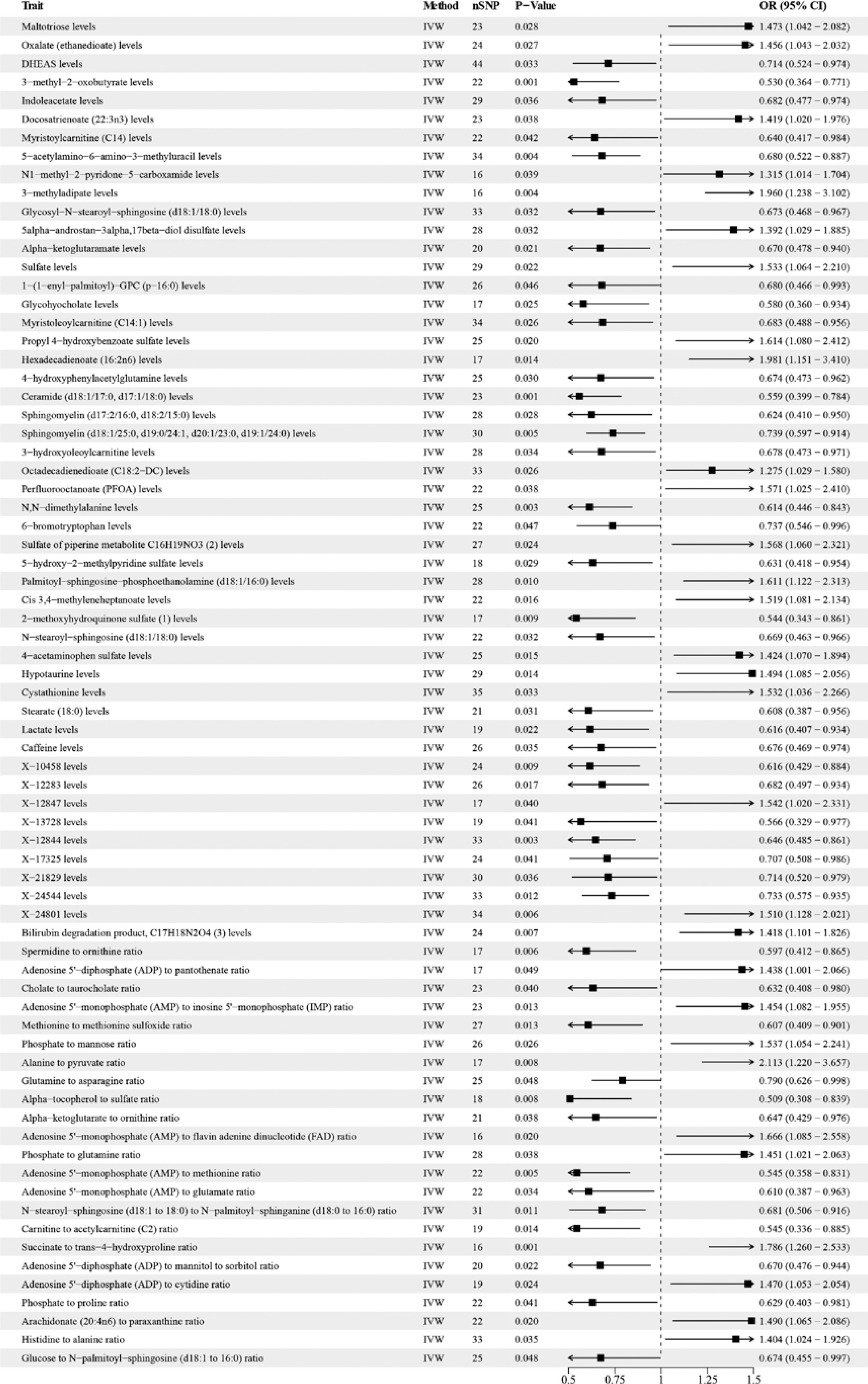
Firstly, 31,638 SNPs were obtained according to the above SNP screening criteria to replace plasma metabolites as the “exposure” (Supplementary Table SVI), and ARDS was used as the “outcome” for MR analysis of 1400 metabolites to ARDS. The IVW analysis results showed that a total of 73 metabolites were associated with ARDS (Figure 6). Sensitivity analysis showed no evidence of horizontal pleiotropy or heterogeneity, and the IVs of each metabolite were relatively robust (Supplementary Tables SVII, SVIII).
Secondly, five inflammatory cytokines, identified in the MR analysis of inflammatory cytokines on ARDS, were used as “exposures,” and 73 metabolites identified by MR analysis of metabolites on ARDS were used as “outcomes.” These two positive results were subjected to MR correlation analysis. IVW test results showed that there were 18 potential causal associations (5 inflammatory cytokines and 18 metabolites, Supplementary Table SIX). Sensitivity analysis further confirmed that our results do not have horizontal pleiotropy or heterogeneity.
Mediation analyses of potential plasma metabolites
To elucidate the potential mechanisms underlying the occurrence and progression of ARDS, we employed mediation analysis to identify the potential pathways involved in metabolic mediated inflammatory cytokines leading to ARDS. We analyzed the 18 metabolites mentioned above to determine their mediating roles in the 5-inflammatory-cytokine-ARDS pathways mentioned above. Finally, we identified two metabolites involved in two mediating relationships between two inflammatory cytokines and ARDS. The total effect of TNF-β levels on ARDS is 0.377 (95% CI: 0.131–0.623), indicating a positive causal effect of TNF-β levels on ARDS; that is, an increase in TNF-β levels increases the risk of ARDS, and this effect is statistically significant. The total effect of FGF19 levels on ARDS is –0.699 (95% CI: –1.143– –0.255). The causal effect of FGF19 levels on ARDS is negative, indicating that elevated FGF19 levels may reduce the risk of ARDS, and this effect is also statistically significant. The direct effect on ARDS is –0.581 (95% CI: –0.918–0.243), and the level of ceramide (d18:1/17:0, d17:1/18:0) has a negative effect on ARDS, indicating that an increase in ceramide (d18:1/17:0, d17:1/18:0) levels reduces the risk of ARDS. The direct effect of α-tocopherol to sulfate ratio on ARDS is –0.675 (95% CI: –1.17–0.175). An increase in α-tocopherol to sulfate ratio is associated with a reduced risk of ARDS, indicating its protective effect on ARDS. Specifically, ceramide (d18:1/17:0, d17:1/18:0) partially mediated the effect of TNF-β levels on ARDS (β = –0.053, SE = 0.032), with a mediation proportion of 14.1%. The α-tocopherol to sulfate ratio mediated the effect of fibroblast growth factor 19 on ARDS (β = 0.124, SE = 0.029), with a mediation proportion of 17.7%.
Discussion
ARDS is closely linked to immune system and inflammatory responses, with both local and systemic inflammatory responses potentially contributing directly to lung injury [1]. The inflammatory cytokines in bronchoalveolar lavage fluid of the ARDS disease model are closely related to the severity of inflammation [28]. There are increasing reports on the relationship between inflammatory cytokines and ARDS. Previous studies have shown that the recruitment of circulating immune cells into the alveolus triggered by chemokines can lead to endothelial and epithelial damage. For example, during the migration of monocytes to the lungs, IFN-β-dependent release of TNF-related apoptosis-inducing ligand promotes epithelial cell apoptosis [29].
Metabolomics can reveal the correlation between metabolites or metabolic pathways and physiological and pathological changes, providing new information for the study of disease mechanisms [13]. Metabolites are downstream products of various intracellular biomolecules, including genes and protein transporters, which enable metabolomics to provide us with information on the metabolic status of the body’s health and disease, as well as to identify biomarkers of drug response [15, 30]. Multiple studies have shown that metabolites and metabolic pathways are closely related to ARDS. The metabolic changes such as oxidative stress metabolism and energy level disorders described in the pathology of ARDS patients are consistent with the metabolic information changes generated by ARDS experiments and clinical studies [15, 31].
Research also showed that cytokine-induced lung inflammation leads to changes in metabolic patterns such as decreased energy status, ATP depletion, and significantly increased glycolytic activity, which are closely associated with disease phenotypes [32–34]. Therefore, we investigated the causal effects of inflammatory cytokines on ARDS, assuming plasma metabolites as potential mediators for fractionation. The results support the mediating role of metabolites in the pathogenesis of ARDS driven by inflammatory cytokines.
With the wide availability of GWAS data, MR mediation analysis can use a large number of public data resources for analysis. These rich data resources enable researchers to analyze a wide range of exposure, mediation, and outcome variables. MR mediation analysis provides a powerful and reliable method for causal inference and mediation effect analysis by combining the advantages of genetics and statistics. MR analysis uses genetic variations as IVs to assess potential causal relationships between exposure and outcomes, which can minimize the influence of confounding factors on causal estimation [35]. The combination of mediation analysis and MR analysis is used to evaluate the impact of exposure on outcomes through mediation, which can prevent bias in estimated values due to unmeasured confounding between exposure, mediation, or outcomes [36]. Therefore, we conducted mediation analysis through two-step MR to evaluate the causal relationship between inflammatory cytokines, plasma metabolites, and ARDS, and determined that the pathway from inflammatory cytokines to ARDS is mediated by plasma metabolites. In a two-step MR study supported by large-scale GWAS and FinnGen data resources, we identified 24 significant associations, indicating potential causal effects of 24 unique inflammatory cytokines and plasma metabolites on the risk of ARDS. Among the 5 inflammatory cytokines, three may have a direct effect on the risk of ARDS, while two may have a mediating effect through the plasma metabolite pathway.
In bidirectional MR analysis studies, fibroblast growth factor 19 levels, interleukin-8 levels, neurturin levels, TNF-β levels, and urokinase type plasminogen activator levels were found to be influencing factors for ARDS risk. Tumor necrosis factor alignment and superfamily member 12 levels, monocyte chemoattractant protein-4 levels, neurotrophin-3 levels, C-X-C motif chemokine 9 levels, β nerve growth factor levels, and C-C motif chemokine 19 levels, in turn, may be the result of ARDS progression. In addition, there were 19 associations between plasma metabolites and ARDS risk in two-step MR analysis, of which two were shown to have mediating effects in the cytokine to ARDS pathway through mediation analysis (TNF-β levels → ceramide (d18:1/17:0, d17:1/18:0) levels → ARDS; fibroblast growth factor 19 levels → α-tocopherol to sulfate ratio → ARDS. These results may suggest that changes in the levels of the first five inflammatory cytokines may play a central role in inducing ARDS mechanisms, among which TNF-β levels and fibroblast growth factor 19 levels may indirectly affect ARDS through metabolite mediated pathways. Huijuan et al. suggested that acute lung injury (ALI) and acute respiratory distress syndrome (ARDS) are characterized by pulmonary microvascular endothelial cells (PMVEC) barrier dysfunction and proinflammatory cytokine influx into lung tissue, resulting in pulmonary edema. Ceramide overproduction is an important mediator of pulmonary hyperinflammation and pulmonary edema in ALI [37]. Hu et al. reported that α-tocopherol (α-TOH) reduces the inflammation and oxidative stress of lung tissue by inhibiting the NF-kB signaling pathway, thereby alleviating lipopolysaccharide (LPS)-induced ALI [38].
These findings provide further insights into the complex interactions between inflammatory cytokines and metabolites in the development of ARDS, promoting the development of innovative strategies for ARDS prevention and treatment. If future case-control studies nested within large population cohorts are validated, our results may make new contributions to the development of risk stratification of ARDS based on metabolites and the determination of new therapeutic targets, thus significantly improving the management and treatment strategies of ARDS.
However, the study has some limitations. There is potential for confounding or bias in MR analyses, especially due to unmeasured pleiotropy. Due to the predominantly European dataset used, demographic stratification bias may have been introduced, limiting the generalizability of the conclusions to other racial groups. Therefore, further research involving diverse racial groups is warranted. Additionally, while several metabolites with a causal relationship with ARDS were identified, there remain unproven metabolites whose role in the disease is not fully understood, hampering a comprehensive analysis and interpretation of the findings. Although we have explored the mediating role of plasma metabolites between different cytokines and the risk of ARDS, considering the direct effects of various cytokines and plasma metabolites, as well as the differences in the effects of certain metabolites not acting as mediators, the mechanisms by which different cytokines affect ARDS still require further clarification.